Dry eye syndrome is a condition in which the stability of the tear film is reduced due to various factors. It causes ocular discomfort and visual disturbances, and may be accompanied by damage to the ocular surface.
The definition by the Japanese Dry Eye Society (2016 revision) is as follows.
“A condition in which the stability of the tear film is reduced due to various factors, causing ocular discomfort and visual disturbances, and may be accompanied by damage to the ocular surface.”
A key feature of the Japanese definition is that it positions reduced tear film stability as the core of the pathology. Positive findings of epithelial damage from fluorescein staining and similar tests are excluded from the diagnostic criteria, allowing reliable diagnosis of tear film stability-decreased DED (short BUT type).
The previous definition (2006, Dry Eye Society) described dry eye as “a chronic disease of the tear film and corneal/conjunctival epithelium caused by various factors, accompanied by ocular discomfort and visual abnormalities.” Japan revised its diagnostic criteria three times—in 1995, 2006, and 2016—and is internationally recognized as a leading country in dry eye clinical practice7).
The TFOS DEWS II (2016) defines dry eye as “a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film, and accompanied by tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities.” While the Japanese definition places decreased tear film stability at the forefront, the international definition also explicitly includes increased tear osmolarity, ocular surface inflammation, and neurosensory abnormalities.
Koumi Study (large-scale cross-sectional study of residents aged 40 and older): Dry eye was confirmed in 12.5% of men and 21.6% of women7)
Epidemiological studies targeting high school students have reported a high frequency of BUT-shortened DED7)
A DED prevalence survey of 4,393 office workers also showed an association with VDT work7)
Prevalence outside Japan:
Reported widely between 7.4% and 33.7% depending on diagnostic criteria and target population
It most commonly affects people in their 40s to 50s, with a higher prevalence in women. It is one of the leading reasons for ophthalmology visits, and its prevalence is increasing with the widespread use of digital devices1).
The estimated number of patients with Sjögren’s syndrome in Japan is 500,000 to 1,000,000, predominantly affecting middle-aged and older women around their 40s, with a female-to-male ratio of approximately 14:1. Sjögren’s syndrome is classified into primary (approximately 70%) and secondary (approximately 30%, associated with collagen vascular diseases) types. Among collagen vascular diseases, rheumatoid arthritis is often accompanied by severe dry eye (secondary Sjögren’s syndrome).
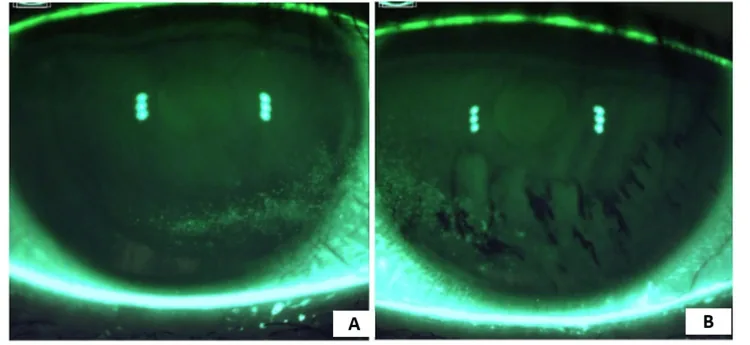
Maiti S, et al. Recalcitrant Dry Eye Disease in a 31-Year-Old Female: Favorable Outcomes Following Complete Ocular Lavage Facilitated by an Irrigating Eyelid Retractor. Cureus. 2025. Figure 2. PMCID: PMC11887804. License: CC BY.
Corneal staining under medical treatment. A shows persistent superficial punctate keratitis in the inferonasal region of the right eye, and B shows persistent superficial punctate keratitis in the inferonasal region of the left eye with an irregular staining pattern. This corresponds to the superficial punctate keratitis discussed in Section “2. Main Symptoms and Clinical Findings.”
Ocular dryness (accompanied by oral dryness in Sjögren syndrome)
QWhy do tears come out even though I have dry eye?
A
An unstable tear film stimulates the cornea and sends signals to the brain, inducing reflex tear secretion. However, these reflex tears are only temporarily increased in volume and are insufficient to restore tear film stability, so the underlying problem is not resolved. This is why tearing occurs in dry eye patients.
In Sjögren’s syndrome cases, conjunctival epithelial damage is prominent and difficult to improve even with punctal occlusion to increase moisture (involvement of immunological inflammation and blink friction)
Dry eye is broadly classified into aqueous-deficient type and hyperevaporative type, with many cases presenting with a mixture of both. Furthermore, the decreased wettability type (short BUT type) is more commonly reported in Asians and is characterized by markedly reduced tear film stability despite normal tear secretion.
Aqueous-deficient type
Sjögren syndrome: A chronic inflammatory autoimmune disease of the lacrimal and salivary glands. Estimated 500,000 to 1,000,000 patients. Most common in middle-aged and older women around their 40s (female-to-male ratio 14:1)
Meibomian gland dysfunction (MGD): Decreased quality and quantity of the lipid layer accelerates tear evaporation. One of the main causes of dry eye.
Abnormal blinking: Decreased blink rate and incomplete blinking when using digital devices1)
Environmental factors: Dryness, air conditioning, wind, low humidity. Humidifiers and side-panel glasses are effective1)
Contact lens wear: Approximately 150 million contact lens wearers worldwide. Lens wear causes tear film instability and increases the risk of DED symptoms8)
Mask-associated dry eye (MADE): Exhaled air leaking from the upper edge of a face mask creates airflow toward the ocular surface, promoting tear evaporation. The prevalence has been reported to be approximately 18.3%. Securing the upper edge of the mask with medical tape to block airflow is an effective preventive measure4)
Other causes include post-LASIK/PRK (usually transient), eyelid abnormalities (lagophthalmos, entropion), neurotrophic keratopathy (trigeminal nerve dysfunction), Stevens-Johnson syndrome, and vitamin A deficiency.
In a cross-sectional study of 108 eyes of type 2 diabetes (DM) patients and 194 eyes of non-DM patients, the DM group had significantly higher rates of lid margin irregularity, meibomian gland orifice obstruction, increased gland thickness, vascularization, and shortened NIBUT12)
Blood glucose level (HbA1c) correlated with NIBUT and lid margin thickening12)
QWhy does prolonged use of digital devices worsen dry eye?
A
During screen work, the blink rate significantly decreases from approximately 16 times/min to 5–7 times/min, and incomplete blinks (blinks where the eyelids do not close fully) increase9). With incomplete blinking, the lipid layer is not evenly spread over the entire corneal surface, leading to increased tear evaporation in areas where the oil layer is thin. Practicing the 20-20-20 rule (every 20 minutes, look at something 20 feet away for 20 seconds) and consciously performing complete blinks are recommended9).
A definitive diagnosis of dry eye is made when both of the following two criteria are met.
Subjective symptoms (ocular discomfort, visual function abnormalities)
Tear film breakup time (BUT) of 5 seconds or less
With the 2016 revision, findings of epithelial damage by fluorescein staining were removed from the mandatory criteria for definitive diagnosis. This change reflects the clinical reality in Japan, where tear film instability-type dry eye (shortened BUT type) accounts for the majority of cases.
Under the previous diagnostic criteria (2006 version), dry eye (definitive case) was defined as meeting all three elements: subjective symptoms, tear film abnormalities, and corneal/conjunctival epithelial damage.
The Japanese Dry Eye Clinical Practice Guidelines recommend the use of questionnaires that meet reliability, validity, and responsiveness for symptom assessment7).
Diagnostic Criteria for Sjögren’s Syndrome (1999 Revision, Ministry of Health and Welfare Research Group)
Diagnosis is made when 2 or more of the following 4 criteria are met:
Biopsy pathology: 1 or more foci per 4mm² (≥50 lymphocytes periductal infiltration) in labial salivary gland or lacrimal gland biopsy
Oral examination: Stage 1 or higher on sialography, or decreased salivary secretion (gum test ≤10 mL/10 min, Saxon test ≤2 g/2 min) + decreased function on salivary gland scintigraphy
Ophthalmologic examination: Schirmer test ≤5 mm/5 min and rose bengal (van Bijsterveld score ≥3) or positive fluorescein staining
Serological examination: Positive anti-SS-A/Ro antibody or positive anti-SS-B/La antibody
In dry eye, symptoms and objective examination findings often diverge, so questionnaires have been developed to quantify subjective symptoms. TFOS DEWS III also positions symptom assessment as the foundation for diagnosis and treatment efficacy evaluation1). The Japanese Dry Eye Diagnostic Guidelines also emphasize the reliability, validity, and responsiveness of questionnaires7).
OSDI (Ocular Surface Disease Index): A 12-item questionnaire that is the most widely used internationally as a patient-reported outcome (PRO) in clinical trials. It consists of three subscales: “ocular symptoms,” “vision-related function,” and “environmental triggers.” Scores of 0–12 are classified as normal, 13–22 as mild, 23–32 as moderate, and 33–100 as severe. Specificity is 0.83 and sensitivity is 0.60.
SPEED (Standard Patient Evaluation of Eye Dryness): An 8-item questionnaire that evaluates symptom frequency and severity. Scored 0–28. With a sensitivity of 0.90 and specificity of 0.80, it is suitable for longitudinal monitoring in daily clinical practice.
SANDE (Symptom Assessment in Dry Eye): The most concise questionnaire with only 2 items. It evaluates frequency and severity using a Visual Analog Scale (VAS).
QWhich should I use, OSDI or SPEED?
A
Choose according to your purpose. OSDI has 12 items and can also evaluate the impact on quality of life, and is internationally standardized as a PRO in clinical trials1). SPEED has 8 items, can be administered quickly, and with a high sensitivity of 0.90, is suitable for longitudinal monitoring in daily clinical practice. Using both together is also effective.
TFOD (Tear Film Oriented Diagnosis) — 6 Patterns of Breakup
This diagnostic classification, unique to Japan, was proposed by the Japanese Dry Eye Society. By identifying the cause of reduced tear film stability through tear film breakup patterns observed immediately after eye opening, it directly links to TFOT (Tear Film Oriented Treatment).
Area break
Pattern: After eye opening, no upward movement of fluorescein is observed, and BUT occurs immediately over a wide area. Accompanied by mucous plaque/filament.
Suggested pathology: Severe aqueous-deficient dry eye. Also associated with severe epithelial damage.
First-line treatment: Increase tear volume by inserting punctal plugs in both the upper and lower lacrimal puncta.
Line break
Pattern: Linear vertical breakup in the lower cornea immediately after eye opening. Accompanied by inferior SPK. BUT is typically 2–3 seconds.
Suggested pathology: Aqueous-deficient dry eye (mild to moderate)
BUT-shortened dry eye is a special type in which tear volume is normal (normal Schirmer value) and vital staining findings are almost absent, yet BUT is markedly shortened and strong subjective symptoms are present. It is thought to be caused by decreased wettability due to abnormal membrane-associated mucin expression.
QWhat is BUT-shortened dry eye?
A
This is a type of dry eye in which BUT is shortened despite normal tear volume (normal Schirmer value). It is the most common type in Japan, and was previously classified as “suspected dry eye” under conventional diagnostic criteria. With the 2016 revision, it became formally diagnosed as dry eye, and treatment selection based on TFOD is important. Diquafosol sodium and rebamipide are considered effective.
Add 1–2 drops of saline to a fluorescein strip, shake well, and shake off excess fluid
Gently touch the strip to the tear meniscus at the lateral one-third of the lower eyelid for staining (it is important not to alter the tear volume)
After gently closing the eye, quickly open and hold it open, then measure the time in seconds until tear film breakup (appearance of a dark spot)
Measure three times, average, and round to the nearest whole number
Also record the breakup pattern at eye opening (for TFOD)
In Japanese criteria, ≤5 seconds is abnormal (in DEWS II, ≤8–10 seconds is abnormal) 5)
Non-invasive BUT (NIBUT):
Because fluorescein instillation itself affects tear film stability, non-invasive measurement methods using Placido disk reflection images have been developed. Sensitivity is 82–84% and specificity 76–94%, and infrared illumination can suppress reflex tearing 5). In Japan, the Keratograph 5M (Oculus) and Idra (SBM) are available.
Fluorescein staining: A basic test to detect abnormalities of the corneal and conjunctival epithelium. The NEI scale divides the cornea into 5 zones, each scored 0–3 (total 0–15)5). The barrier function of the conjunctival epithelium is more fragile than that of the corneal epithelium, and in dry eye, the conjunctival epithelium is impaired equally or more severely. Using a blue-free filter allows clearer observation of the conjunctival epithelium.
Lissamine green and rose bengal: Stains dead cells and mucus of the conjunctiva. The van Bijsterveld score (rose bengal, 9 points maximum) is used in the ophthalmologic diagnostic criteria for Sjögren syndrome (≥3 points positive). Lissamine green is less toxic and better tolerated than rose bengal.
Schirmer test:
Uses 5 mm × 35 mm filter paper with 1 mm interval graduations.
Method I (without anesthesia): Without topical anesthetic, with eyelids open and blinking freely, the paper is placed at the lateral one-third of the lower eyelid for 5 minutes. Interpretation: ≤5 mm abnormal, 5–10 mm borderline, ≥10 mm normal. In Sjögren syndrome, the result may be 0 mm5)
Method II (nasal mucosa stimulation reflex): Stimulates the nasal mucosa (along the nasal septum) with a cotton swab to measure reflex tear secretion. ≤10 mm is considered abnormal. Performed only on the side with a low value in Method I. Useful for evaluating reflex lacrimal secretion in severe dry eye such as Sjögren syndrome and GVHD
Although reproducibility is limited, it is useful as a screening tool.
Tear meniscus evaluation: 75–90% of the total tear volume on the ocular surface is present in the tear meniscus. The normal value is approximately 0.2 mm. Observing before staining allows direct assessment of tear volume, which is useful for diagnosing aqueous-deficient dry eye. Anterior segment OCT (AS-OCT) can objectively measure tear meniscus height (TMH), area, and volume6).
Tear osmolarity: Measured with a TearLab osmometer. Less than 300 mOsm/L (interocular difference <8) is normal, 300–320 is mild, 320–340 is moderate, and above 340 is severe5).
MMP-9 test (InflammaDry): A point-of-care test that measures MMP-9 in tears. A result of 40 ng/mL or higher is positive. It is useful for deciding whether to start anti-inflammatory treatment, but may yield false positives in allergic conjunctivitis or infections5).
Lactoferrin test: Lactoferrin is an antibacterial and anti-inflammatory protein produced by the acinar cells of the lacrimal gland. Its levels decrease in dry eye patients and can be measured using the TearScan 270 MicroAssay System5).
Lipid layer thickness (LLT): Quantitatively assessed in interferometric color units (ICU) using the LipiView interferometer. Measurement range is 0–240 ICU. It also features automatic detection of incomplete blinks6).
Meibography: An examination that visualizes meibomian gland structure using infrared transillumination. Meibomian gland dropout is graded on a 4-point scale (0 = 0–25% loss, 1 = 26–50%, 2 = 51–75%, 3 = 76–100%)6). The degree of dropout and structural changes guide MGD treatment decisions.
Anterior segment OCT (AS-OCT): In addition to quantitative measurement of the tear meniscus, it can acquire corneal thickness and epithelial thickness maps, as well as cross-sectional images of meibomian glands6).
Confocal laser scanning microscopy: Used for cell-level evaluation of the cornea. It can assess nerve fiber density, inflammatory cell density, and epithelial cell morphology, and is useful for differentiating corneal neuropathic pain and neurotrophic diseases6).
Functions: Meibography, bulbar conjunctival hyperemia assessment, TMH measurement, and NITBUT measurement can all be performed with a single device. It automatically quantifies hyperemia on a 0–4 scale and displays a 360-degree color map of the corneal surface6).
LipiView II (J&J Vision)
Function: Meibomian gland evaluation and quantitative lipid layer assessment using interferometry. Equipped with a video module that automatically calculates incomplete blinking6)
Drug-induced toxic keratopathy: Characterized by less conjunctival epithelial damage compared to corneal epithelial damage (dry eye damages both the cornea and conjunctiva)
Epiphora (lacrimal duct obstruction): Perform BUT and Schirmer test to differentiate between lacrimal passage obstruction and reflexive hypersecretion (which is actually dry eye)
Sjögren’s syndrome: Prominent conjunctival epithelial damage, difficult to improve with punctal occlusion, positive autoantibodies
This is a treatment concept recommended by the Japanese Dry Eye Society. TFOD identifies the cause of reduced tear film stability, and treatment is selected according to the maintenance of homeostasis of the causative tear film layer.
TFOT Stratified Treatment Table
Treatment target layer
Treatment
Lipid layer
Warm compresses, eyelid hygiene, small amount of eye ointment, diquafosol sodium (lipid layer spread enhancement)
The following are the currently available eyedrops widely used under Japanese health insurance.
0.1% / 0.3% Sodium hyaluronate ophthalmic solution (Hyalein®):
Used for corneal epithelial protection and moisture retention. The Japanese Dry Eye Diagnostic Guidelines “recommend” hyaluronic acid eyedrops7).
3% Diquafosol sodium ophthalmic solution (Diquas® / Diquas LX®):
P2Y2 receptor agonist. Promotes water and mucin secretion and lipid layer spreading. Developed in Japan. The Japanese Dry Eye Diagnostic Guidelines give it a “recommend for implementation” rating (strong recommendation)7).
2% Rebamipide ophthalmic solution UD (Mucosta® ophthalmic solution UD):
Promotes mucin production and has anti-inflammatory effects. The Japanese Dry Eye Diagnostic Guidelines give it a “recommend for implementation” rating (strong recommendation)7).
Artificial tears (Soft Santear etc., preservative-free):
The basic treatment. Preservative-free formulations are preferable. The Japanese Dry Eye Clinical Practice Guideline “suggests” (weak recommendation) artificial tears7).
0.3% Ofloxacin Ophthalmic Ointment (Tarivid® Ophthalmic Ointment):
Preservative-free; the oily components spread over the tear film. Used off-label as a protective agent for severe cases.
When reflex tear secretion is reduced, it is desirable to use preservative-free eye drops. If inflammation is thought to be involved in symptom exacerbation, consider concomitant use of steroid eye drops.
Hyalein Mini Ophthalmic Solution (0.1%) 6 times/day
Hyalein Mini Ophthalmic Solution (0.3%) 6 times/day + Flumetholon Ophthalmic Solution (0.1%) 4 times/day (keep the duration of steroid use to the minimum necessary)
Prescription Example (Sjögren’s Syndrome Complicated)
Cyclosporine eye drops: Suppress T-cell-mediated inflammation. Available as 0.05% (Restasis®) and 0.09% nanoemulsion (Cequa®)1). At the time of the 2019 Japanese Dry Eye Clinical Practice Guidelines, these were not covered by insurance in Japan, but some formulations have been approved in recent years7).
Lifitegrast eye drops (Xiidra®): Inhibit LFA-1/ICAM-1 interaction, suppressing T-cell activation and migration to the ocular surface1). Available overseas.
Steroid eye drops: Used short-term during acute exacerbations to control inflammation. The Japanese Dry Eye Clinical Practice Guidelines suggest their use (with attention to elevated intraocular pressure)7).
Lifestyle modifications are the foundation of dry eye management1). Management of digital device use time, indoor humidification, adequate sleep, and a diet containing omega-3 fatty acids are recommended1). However, the DREAM trial (Dry Eye Assessment and Management, 535 participants, multicenter double-blind RCT) found that 12-month intake of omega-3 fatty acids (EPA 2000mg + DHA 1000mg/day) did not result in significant improvement in OSDI scores compared to placebo (between-group difference -1.9, p=0.21)3). The additional benefit of high-dose omega-3 fatty acid supplements may be limited. Glasses with side panels and moisture-retaining eyewear reduce evaporation and improve symptoms1).
MGD is the main cause of evaporative dry eye and requires active treatment1).
Warm compress: Warm the eyelids for 5–10 minutes to melt meibomian gland lipids (melting point 32–35°C)
Eyelid hygiene: Clean the base of the eyelashes to maintain eyelid margin hygiene
LipiFlow®: Vectorized thermal pulsation therapy. An automated device that warms the meibomian glands from the inside while applying compression from the outside1)
IPL (Intense Pulsed Light): Exerts effects through anti-inflammatory action and gland function recovery1)
QAre warm compresses really effective for dry eye?
A
It is effective for evaporative dry eye caused by meibomian gland dysfunction (MGD)1). The melting point of meibomian gland lipids is approximately 32–35°C, and warm compresses melt and expel the lipids, improving the lipid layer. Automated devices such as LipiFlow enable more efficient heating and expression, and prospective studies have reported improvements in BUT and OSDI at 3 months post-treatment1).
It is indicated for aqueous-deficient dry eye that does not respond adequately to eye drop therapy. The Japan Dry Eye Clinical Practice Guideline recommends the use of punctal plugs7).
Silicone Plugs:
Eagle Vision: Super Eagle™ Plug (3 sizes: S/M/L, select by measuring punctal diameter)
FCI: Punctal Plug® F (one size, head gel-swelling, low risk of migration and extrusion)
Liquid Plug (Keeptear®, Koken):
An atelocollagen liquid plug. Main features:
Storage temperature: 2–10°C refrigerated (denatures at room temperature)
Gelates at 36°C and occludes the canaliculus
Re-liquefies at 40°C or higher (warm water used for removal)
Volume: 300μL (for 2 puncta)
Covered by insurance
Selection of insertion site:
Severe aqueous-deficient cases (e.g., Sjögren’s): Insert into both upper and lower puncta
Mild or BUT-shortened type: One side (lower punctum) only
Average punctum diameter: 0.5–0.8 mm. The upper punctum tends to be smaller than the lower punctum.
In BUT-shortened dry eye, epiphora and blurred vision may occur, so caution is required. Additionally, if ocular surface inflammation is active, it is preferable to insert after controlling the inflammation.
QAre punctal plugs indicated for all dry eye patients?
A
No. The indication for punctal plugs is aqueous tear-deficient dry eye that does not respond adequately to eye drops7). Severe cases associated with Sjögren’s syndrome, Stevens-Johnson syndrome, and GVHD are also good indications. On the other hand, in short BUT-type dry eye where tear volume is not necessarily reduced, punctal plugs may cause tearing and blurred vision, so caution is required. Additionally, if ocular surface inflammation is active, it is preferable to insert the plugs after controlling the inflammation.
Surgical punctal occlusion (cautery): When punctal plugs cannot be retained, or in cases of enlarged punctum
Autologous serum eye drops: Contains growth factors, vitamin A, etc., and is effective for refractory epithelial defects that resist all other treatments. The Japanese Dry Eye Clinical Practice Guideline generally recommends not performing this treatment, but it is used in severe refractory cases7).
Dry eye glasses (with side shields): When control is insufficient even with eye drops and punctal occlusion
Muscarinic receptor (M3) agonists: Cevimeline hydrochloride hydrate, Pilocarpine hydrochloride. Approved for xerostomia (dry mouth), but also reported to be effective for ocular symptoms (side effects: note sweating and gastrointestinal symptoms).
The Japanese Dry Eye Clinical Practice Guidelines recommend against NSAID eye drops and recommend against autologous serum eye drops for general dry eye7).
The tear film consists of three layers from the outside: the lipid layer (derived from meibomian glands), the aqueous layer (derived from lacrimal glands), and the mucin layer (derived from goblet cells and corneal epithelium). This structure forms a stable tear film that protects the cornea and conjunctiva, supplies nutrition, maintains refractive power, and provides antibacterial action.
Two Stages of Tear Film Formation (Upon Eye Opening)
Stage 1: When the upper eyelid rises upon opening, the aqueous fluid stored in the lower tear meniscus is drawn upward and spread across the corneal surface
Stage 2: The lipid layer extends upward, pulling the aqueous layer along with it
When tear volume is extremely low, Stage 1 fails and area breaks occur. Poor wettability (membrane-associated mucin abnormality) causes spot/dimple breaks, while accelerated aqueous layer evaporation causes random breaks.
The lacrimal gland, as the main lacrimal gland, secretes the aqueous components of tears (water, electrolytes, and proteins)2). This secretion is under strict neural control by the parasympathetic, sympathetic, and sensory nerves2).
Afferent pathway: Corneal polymodal nociceptors (trigeminal polymodal nociceptors) are the primary drivers of reflex tear secretion. Corneal mechanoreceptors and cold receptors have weaker secretory stimulation effects2)
Efferent pathway (parasympathetic): Promotes secretion of water, electrolytes, IgA, and proteins2)
Efferent pathway (sympathetic): Primarily regulates protein secretion2)
Rapid responses to environmental changes are possible, and slight changes in tear electrolyte concentration correlate with dry eye2).
Membrane-Associated Mucins and Corneal Epithelial Wettability
Membrane-associated mucins (MUC1/MUC16) maintain the wettability of the corneal epithelium. When their expression is impaired, the phospholipid (hydrophobic) cell membrane is exposed, reducing wettability. This leads to short BUT-type dry eye and increased higher-order aberrations.
T-lymphocyte infiltration around ducts of lacrimal and salivary glands → inflammation with epithelial cells → B-lymphocyte infiltration → lymphoid follicle formation
Lymphocyte infiltration around intralobular ducts, intralobular and interstitial fibrosis
Etiological hypotheses: genetic predisposition + immunological factors + environmental factors (EBV, HTLV-I, and HCV infection reported to be involved)
Lacrimal gland damage → decreased reflex secretion → irreversible epithelial damage → vicious cycle. Conjunctival epithelial damage is prominent and difficult to improve even with punctal occlusion (involvement of immunological inflammation and blink-related friction)
DEWS II classifies based on the presence or absence of subjective symptoms and ocular surface findings. When both subjective symptoms and ocular surface findings are positive, a diagnosis of dry eye is made. Cases with ocular surface findings but no subjective symptoms are considered a ‘neuroparalytic state (sensory dysfunction)’ and are managed preventively.
TFOS DEWS III (2025) presents an evidence-based treatment algorithm based on diagnostic subtypes (aqueous deficient / evaporative / mixed)1). A systematic approach combining tear supplementation, tear retention, tear stimulation, ophthalmic supplements, and meibomian gland treatment according to disease subtype is recommended1).
Actively treating dry eye (particularly evaporative dry eye / MGD) before cataract surgery or LASIK improves postoperative visual outcomes and patient satisfaction1). Prospective studies have reported that LipiFlow treatment before LASIK significantly improves OSDI and BUT at 3 months postoperatively1). TFOS DEWS III recommends that preoperative dry eye management should be standard of care1).
Motzigvatrep ophthalmic suspension 0.3% (Avarept® Suspicious Ophthalmic Suspension): The world’s first dry eye treatment with TRPV1 antagonistic action. It was approved in Japan by Mochida Pharmaceutical in December 2025 and launched by Senju Pharmaceutical in April 2026. By inhibiting the TRPV1 channel, a nociceptor on the ocular surface, it directly suppresses subjective symptoms derived from neural sensitization such as “stinging and gritty sensation”, which differs from existing drugs such as tear supplementation (artificial tears), secretion promotion (diquafosol, rebamipide), and anti-inflammatories (cyclosporine). The dosage is 1 drop 4 times daily. Phase 2b trial (SJP-0132, a Japanese domestic multicenter randomized double-masked dose-ranging study) showed significant improvement in DEQS (Dry Eye-Related Quality-of-Life Score)13), and based on this, the Phase 3-02 trial led to approval. Although it is difficult to differentiate from existing drugs in tear volume and staining scores, it is positioned as a new option for subjective symptom-dominant type (neuralgia-like symptoms) and cases with residual symptoms despite existing treatment.
Perfluorohexyloctane (Miebo®): A novel tear stabilizer approved by the US FDA in 2023. It targets evaporative dry eye disease by physically suppressing tear evaporation. It is available as a prescription drug in the United States and may be classified as a medical device in other regions. Approval status in Japan requires confirmation1).
Nasal neurostimulation: Electrical stimulation of the trigeminal nerve triggers the nasolacrimal reflex to promote tear production. TFOS DEWS III describes this as a neuromodulation option1).
Varenicline nasal spray (Tyrvaya®): Stimulates nicotinic receptors on peripheral trigeminal nerve endings to induce reflex tear secretion. Approved for dry eye in the United States1).
Biological tear substitutes: Autologous serum, allogeneic serum, and platelet-rich plasma (PRP) are being studied as options for refractory cases1).
Low-level light therapy (LLLT): Anti-inflammatory effects on MGD have been reported1).
Jones L, Craig JP, Markoulli M, Karpecki P, Akpek EK, Basu S, et al. TFOS DEWS III: Management and Therapy. American journal of ophthalmology. 2025;279:289-386. doi:10.1016/j.ajo.2025.05.039. PMID:40467022.
Dartt DA. Neural regulation of lacrimal gland secretory processes: relevance in dry eye diseases. Progress in retinal and eye research. 2009;28(3):155-77. doi:10.1016/j.preteyeres.2009.04.003. PMID:19376264; PMCID:PMC3652637.
Dry Eye Assessment and Management Study Research Group. n-3 Fatty Acid Supplementation for the Treatment of Dry Eye Disease. N Engl J Med. 2018;378(18):1681-1690. doi:10.1056/NEJMoa1709691. PMID:29652551; PMCID:PMC5952353.
Boccardo L. Self-reported symptoms of mask-associated dry eye: a survey study of 3,605 people. Contact Lens Anterior Eye. 2022;45(2):101408. doi:10.1016/j.clae.2021.01.003. PMID:33485805; PMCID:PMC7816875.
Nodecker K, Madabhushi S, Brocks D. Analysis of Prosthetic Replacement of the Ocular Surface Ecosystem Anterior Surface Condition Using Noninvasive Keratograph Break-Up Time. Eye Contact Lens. 2024;50:52-55. doi:10.1097/icl.0000000000001050.
Garcia-Terraza AL, Jimenez-Collado D, Sanchez-Sanoja F, et al. Reliability, repeatability, and accordance between three different corneal diagnostic imaging devices for evaluating the ocular surface. Front Med (Lausanne). 2022;9:893688. doi:10.3389/fmed.2022.893688. PMID: 35966863; PMCID: PMC9372285.
Craig JP, Alves M, Wolffsohn JS, Downie LE, Efron N, Galor A, et al. TFOS Lifestyle Report Executive Summary: A Lifestyle Epidemic - Ocular Surface Disease. The ocular surface. 2023;30:240-253. doi:10.1016/j.jtos.2023.08.009. PMID:37659474.
Wolffsohn JS, Lingham G, Downie LE, et al. TFOS Lifestyle: Impact of the digital environment on the ocular surface. Ocul Surf. 2023;28:213-252. doi:10.1016/j.jtos.2023.04.004.
Sullivan DA, da Costa AX, Del Duca E, Doll T, Grupcheva CN, Lazreg S, et al. TFOS Lifestyle: Impact of cosmetics on the ocular surface. The ocular surface. 2023;29:77-130. doi:10.1016/j.jtos.2023.04.005. PMID:37061220; PMCID:PMC11246752.
Markoulli M, Ahmad S, Arcot J, Arita R, Benitez-Del-Castillo J, Caffery B, et al. TFOS Lifestyle: Impact of nutrition on the ocular surface. The ocular surface. 2023;29:226-271. doi:10.1016/j.jtos.2023.04.003. PMID:37100346.
Song W, Wu X, Cheng C, et al. Relationship between type 2 diabetes mellitus and changes of the lid margin, meibomian gland and tear film in dry eye patients: a cross-sectional study. BMJ Open Diabetes Res Care. 2024;12(1):e003745.
Hori Y, Wada T, Omatsu K, et al. Efficacy and Safety of SJP-0132 in Patients With Dry Eye Disease: A Phase 2b Randomized, Double-Masked, Dose-Finding Study. Am J Ophthalmol. 2026;283:163-175. doi:10.1016/j.ajo.2025.11.036. PMID: 41352685.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.