Meibomian gland dysfunction (MGD) is a chronic, diffuse abnormality of the meibomian glands. The Japanese MGD Working Group (2010) defined it as “a condition in which the function of the meibomian glands is diffusely impaired due to various causes, accompanied by chronic discomfort” 4). In recent years, MGD has been positioned as the main cause of evaporative dry eye, and clinical practice guidelines that comprehensively organize diagnosis, testing, and treatment have been published 3).
Internationally, the International Workshop on Meibomian Gland Dysfunction (IWMGD 2011) defines it as “a chronic, diffuse abnormality of the meibomian glands, commonly characterized by terminal duct obstruction and/or qualitative/quantitative changes in glandular secretion” 1), 10). In TFOS DEWS III (2025), MGD is positioned as a major contributor to dry eye, and device-based treatments such as warm compresses, eyelid hygiene, IPL, and low-level laser are incorporated into the management algorithm 8). In Japan, the Dry Eye Society has established the “Dry Eye Clinical Practice Guidelines” (2019), emphasizing MGD as a cause of evaporative dry eye9).
Meibomian glands are a type of large sebaceous gland located within the tarsal plates of the eyelids. When observed with non-contact meibography, normal eyes have 25 to 30 glands in the upper eyelid and 15 to 20 in the lower eyelid 5). Each gland has numerous acini branching from a central duct, and the acinar epithelial cells (meibocytes) produce meibum via holocrine secretion. Meibum contains over 100 types of lipids (mainly wax esters, cholesterol esters, polar phospholipids, and sphingolipids) and more than 90 types of proteins, forming the lipid layer of the tear film’s outermost layer to prevent evaporation of the aqueous layer and reduce surface tension to maintain tear film spread 1). The lipid layer thickness (LLT) is normally 60 to 100 nm, and it becomes thinner in MGD 1).
In a Japanese population-based study (residents aged 6 to 96 years), the age-specific prevalence of MGD is as follows 3).
Age group
MGD prevalence
19 years or younger
0%
20s
11.8%
30s
5.6%
40s
21.6%
50s
32.8%
60s
41.9%
70s
48.4%
80s
63.9%
Many studies have shown that MGD increases and worsens with age. In terms of sex, it is more common in men and postmenopausal women3). A study by Arita et al. using non-contact meibography reported that approximately 86% of dry eye patients have concomitant MGD5). Racial differences have also been noted, with a higher prevalence (3.5–19.9%) reported in Asians than in Caucasians1). In Japan, the Dry Eye Society estimates that there are tens of millions of patients, including potential cases, making it one of the most frequently encountered chronic diseases in daily practice3).
Secondary: ocular infection, seborrheic dermatitis, etc.
Clinically, the hyposecretory type is more common, and among them, obstructive MGD (oMGD) is the most prevalent. The main pathophysiology of hyposecretory MGD is summarized as “hyperkeratinization of the ductal epithelium and atrophy of the acini” 3). Atrophic MGD is a condition where the acini are diffusely atrophied, and both mechanisms of secondary obstruction and primary acinar cell damage have been proposed.
The hypersecretory type of MGD includes seborrheic MGD (sMGD), which is also recognized in contrast to obstructive meibomianitis. When the tarsal plate of the upper eyelid is lightly pressed, normal individuals secrete clear meibum, but in seborrheic MGD, secretion is abnormally increased, and foam formation is observed in the tear fluid along the lower eyelid margin. Related diseases include posterior blepharitis, meibomianitis, and meibomitis-related keratoconjunctivitis (MRKC), and it is important to organize these concepts 3).
Internationally, the IWMGD 2011 classifies MGD into low-delivery and high-delivery types, with obstructive MGD being the most common among the low-delivery type 1).
QHow are MGD and dry eye related?
A
MGD is the most common cause of evaporative dry eye. When meibomian gland dysfunction leads to thinning of the tear film lipid layer, tear evaporation increases, tear osmolarity rises, and inflammation occurs on the ocular surface. MGD can lead to dry eye and cause chronic ocular discomfort.
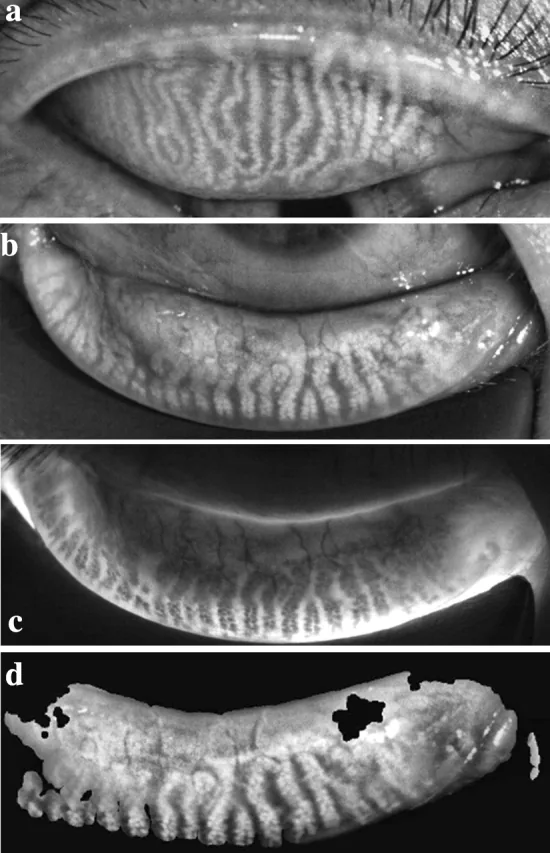
Li B, et al. Comparison of the therapeutic effect of Meibomian Thermal Pulsation LipiFlow® on obstructive and hyposecretory meibomian gland dysfunction patients. Int Ophthalmol. 2020. Figure 1. PMCID: PMC7669766. License: CC BY.
Meibography of the upper and lower eyelids shows tortuosity, irregular arrangement, and partial dropout of meibomian glands. This directly demonstrates morphological abnormalities characteristic of MGD and is suitable for explaining the main clinical findings.
A sticky sensation, often described as “gooey,” is also characteristic4). Symptoms are often worse in the morning, and patients may report fluctuations in visual function. However, no specific subjective symptoms have been identified to distinguish MGD from other ocular surface diseases3). The Ocular Surface Disease Index (OSDI) questionnaire is widely used to assess subjective symptoms. MGD symptoms significantly impact quality of life, causing not only ocular irritation but also visual impairment, so it is important to systematically assess the degree of interference with daily activities1).
In diagnosing MGD, four findings are useful: meibomian gland orifice obstruction, eyelid margin vascular dilation, displacement of the mucocutaneous junction, and irregularity of the eyelid margin3).
Eyelid Margin Findings
Orifice obstruction findings: plugging, pouting (pointed elevations around the orifice), and ridge (ridge-like structure covering multiple orifices).
Eyelid margin vascular dilation: Capillary dilation and telangiectasia around the orifices.
Displacement of the mucocutaneous junction (MCJ): Anterior or posterior deviation. Easily observed with fluorescein staining.
Eyelid margin irregularity: Irregular contour of the line in contact with the cornea.
Meibum Gland Evaluation
Meibum characteristics: Normal meibum is clear oil. In MGD, it appears cloudy, granular, or toothpaste-like.
Shimazaki classification: Expressibility under moderate thumb pressure is graded 0 to 3, with grade 2 or higher considered abnormal.
Meibography: Infrared camera observation of gland dropout, shortening, and distortion.
Thinning of the tear film lipid layer: Lipid layer thickness (LLT) can be assessed with an interferometer.
Shimazaki’s meibum grade is evaluated on the following 4-point scale4), 12).
Grade 0: Clear meibum is easily expressed with light pressure
Grade 1: Cloudy meibum is expressed with light pressure
Grade 2: Cloudy meibum is expressed with moderate or greater pressure
Grade 3: No meibum is expressed even with firm pressure
The non-contact meibography developed by Arita et al. in 2008 is a minimally invasive device that simply attaches an infrared transmission filter (700–850 nm) and a small infrared CCD camera to a slit-lamp microscope 5), 11). Infrared light passes through the tarsal plate and is reflected by meibum, so meibomian glands are observed as highly reflective (white). In MGD patients, various findings such as gland dropout, shortening, tortuosity, mottling, and dilation are mixed 5).
The degree of gland dropout is classified into the following four grades according to the Arita meiboscore 5).
Meiboscore
Area of gland dropout
Grade 0
No dropout
Grade 1
Less than one-third of the total
Grade 2
One-third to two-thirds
Grade 3
Two-thirds or more
Contact lens wearers have been reported to have more meibomian gland dropout than non-wearers. The changes become more noticeable with longer years of wear and are observed with both soft and hard contact lenses16).
The following factors are associated with the development of MGD3).
Aging and Hormonal Factors
Aging: The most important risk factor, leading to acinar atrophy and decreased function
Men and postmenopausal women: Higher prevalence
Androgen deficiency: Androgens promote lipid synthesis in the meibomian glands and suppress keratinization. Deficiency, receptor abnormalities, and anti-androgen drugs are associated with obstructive MGD1)
Estrogen: Suppresses lipid secretion and has a pro-inflammatory effect on the ocular surface1)
Ocular and External Factors
Soft contact lens wear: Promotes mechanical obstruction of the openings
Visual display terminal (VDT) work: Increased evaporation due to reduced blinking
Smoking, rural residence, Asian ethnicity: Reported associations with MGD3)
Long-term use of glaucoma eye drops: Toxicity of preservatives and the drug itself
History of ocular surgery: Reports of MGD exacerbation after cataract and refractive surgery
Medications: Isotretinoin, antihistamines, antidepressants, etc.
Systemic diseases
Diabetes mellitus: An association with MGD has been reported3). In a cross-sectional study of 302 eyes with dry eye disease complicated by type 2 diabetes, the DED-DM group had significantly more severe orifice obstruction grade (P<0.0001), lid margin vascular dilation (P<0.0001), upper lid meibomian gland dropout (P=0.003), and non-invasive BUT (P=0.011) compared to the DED-only group7)
Dyslipidemia, hypertension, hyperthyroidism: An association with MGD has been reported3)
Rosacea, Sjögren’s syndrome, Stevens-Johnson syndrome, graft-versus-host disease: Associated with MGD via ocular inflammation3)
Demodex infection
Demodex folliculorum parasitizes the eyelash roots, while Demodex brevis parasitizes the meibomian glands and sebaceous glands1). The infestation rate increases with age, reaching 100% in those aged 70 years or older1). In a cohort study of 150 cases, Demodex was detected in 90% of patients with anterior blepharitis and 60% of patients with MGD1). D. folliculorum directly damages hair follicle basal cells, causing reactive hyperkeratinization and forming cylindrical dandruff. D. brevis physically obstructs the meibomian glands, inducing granulomatous reactions and promoting the development of chalazia1). Demodex also acts as a bacterial vector, triggering inflammation, and can cause delayed-type hypersensitivity reactions in patients with rosacea1). Zhang et al. reported a case of MGD in a 46-year-old man in whom 15 Demodex brevis were detected in expressed meibum despite few external findings, demonstrating the usefulness of direct meibum microscopy6).
QIs there an association between contact lenses and MGD?
A
Soft contact lens wear is considered a risk factor for MGD. Mechanical friction during blinking due to lens wear may cause shortening and dropout of meibomian glands and obstruction of the orifices. MGD may be a cause of contact lens intolerance, and MGD treatment may improve wearing comfort.
The diagnostic criteria for hyposecretory MGD proposed by the Japanese MGD Working Group in 2010 require all three of the following items to be positive4). These criteria are widely used in Japan3).
Item
Content
1. Subjective symptoms
Ocular discomfort, foreign body sensation, dryness, sensation of pressure, etc.
2. Abnormal findings around the orifice
One or more of the following: telangiectasia, displacement of the mucocutaneous junction, or irregularity of the eyelid margin
3. Findings of orifice obstruction
Both obstructive signs (plugging/pouting/ridge) and reduced expressibility (Shimazaki grade 2 or higher)
The evaluation of MGD combines the following tests3).
Slit-lamp microscopy for meibum observation: semi-quantitative assessment of meibum quality and quantity
Anatomical observation of the eyelid margin: confirm the four findings described above
Meibography: non-contact type is the international standard, short duration, and minimally invasive5). Quantified using the meiboscore.
Tear film break-up time (BUT): decreased in MGD but not a specific test
Fluorescein staining: most versatile for evaluating corneal and conjunctival epithelial damage
Tear film lipid layer thickness (LLT) measurement: interferometry shows thinner LLT in MGD patients, but cutoff values are not established
Tear osmolarity measurement: currently limited clinical utility
In vivo confocal microscopy, tear evaporation measurement, inflammatory biomarkers in tears, bacteriological examination, and biochemical analysis of meibum all currently have limited roles as routine tests3). Although elevated IL-1α, IL-1β, and MMP-9 in tears are important in the pathogenesis, clinical application has not been achieved due to lack of standardization of equipment and conditions1).
In outpatient clinics in Japan, it is recommended to incorporate non-contact meibography into the slit-lamp microscope workflow 5).
Have the patient place their face on the chin rest of the slit-lamp microscope
Observe the area around the meibomian gland openings and the eyelid margin under diffuse light (plugging/pouting/ridge, vascular dilation, MCJ displacement, eyelid margin irregularity)
Perform fluorescein staining and measure corneal and conjunctival epithelial damage (SPK) and tear film breakup time (BUT) using a blue filter
Switch to an infrared transmission filter, observe the upper and lower meibomian glands with meibography, and record still images or video. Determine the meiboscore
Return to diffuse light, compress the center of the eyelid with the thumb or expressing forceps, and evaluate the quality and expressibility of meibum (Shimazaki classification)
The series of tests is usually completed within 3 to 5 minutes, with minimal burden on the patient. Meibography provides visual feedback to the patient and helps improve treatment motivation 5).
Aqueous tear-deficient dry eye (ADDE): Evaluate decreased Schirmer test values and assess for Sjögren’s syndrome. According to TFOS DEWS II, evaporative and mixed types account for the majority of cases
Posterior blepharitis / Meibomianitis: Related diseases that form a continuous spectrum with MGD. Conceptual organization is important 3)
Meibomianitis-related keratoconjunctival epitheliopathy (MRKC): A term frequently used in Japan, referring to corneal and conjunctival epithelial damage secondary to meibomianitis
There is no single gold-standard treatment for MGD; a stepwise and combined approach is fundamental 1,3). The Japanese Dry Eye Clinical Practice Guideline 2019 also identifies MGD as the main cause of evaporative dry eye and presents a treatment algorithm with warm compresses and lid hygiene as first-line therapy 9). The TFOS DEWS III Management and Treatment Report (2025) proposes stepwise management combining warm compresses, in-office device treatments, IPL, low-level light therapy (LLLT), lid scrub, anti-Demodex therapy, and blepharoexfoliation as a standard approach for MGD 8).
Conservative Treatment (First-Line)
Warm compresses: Raise the eyelid temperature above the melting point of meibum to promote secretion. It is recommended to use a commercially available warm eye mask twice daily for at least 5 minutes.
Eyelid hygiene: Wipe the eyelid margin with a cotton ball moistened with water or a commercial cleansing agent. Daily continuation is the principle.
Meibum expression: Performed as an outpatient procedure using Arita meibomian gland forceps at intervals of 10 days to 1 month. Obstructive MGD is a good indication.
Artificial tears: Used for tear supplementation and ocular surface moisturization.
Azithromycin hydrate ophthalmic solution: Improves subjective symptoms, eyelid margin findings, and meibum grade. Not covered by insurance for MGD alone, but efficacy and effectiveness are recognized for blepharitis17).
Tetracycline oral: Not covered by insurance. A regimen of doxycycline 100 mg twice daily, tapered over 3–4 months, is used.
Corticosteroid ophthalmic solution: In Japan, covered by insurance only when blepharitis is present. 0.1% fluorometholone or similar is used short-term in combination.
Omega-3 fatty acids oral: Treated as a supplement in Japan and not covered by insurance.
Intense pulsed light (IPL) therapy: A broadband high-intensity non-laser light of 500–1200 nm is applied to the periorbital area1), 8). The light energy absorbed by oxyhemoglobin in skin blood vessels generates heat, inducing thermal coagulation of abnormal vessels, bacterial reduction, Demodex elimination, meibum liquefaction, suppression of epithelial turnover, fibroblast activation, and collagen synthesis promotion1). A randomized controlled trial (RCT) of 88 eyes reported that three consecutive sessions (at 4-week intervals) significantly reduced tear levels of IL-17α and IL-61). Multiple RCTs have shown improvements in subjective symptoms, lid margin findings, meibum grade, tear break-up time (BUT), and corneal epithelial damage. However, it is necessary to confirm whether the treatment is approved and covered by insurance in Japan before considering it at a specialized facility. Adverse events include eyelid redness and swelling in up to 13% of cases, all mild and reversible1).
Thermal pulsation therapy (e.g., LipiFlow): The LipiFlow® (TearScience) is a vectored thermal pulsation (VTP) device that simultaneously applies 42.5°C heating from the conjunctival side of the eyelid and pulsatile compression from the outer eyelid in a distal-to-proximal direction for 12 minutes1). It is the only device that directly heats the inner surface of the meibomian glands, raising the upper eyelid temperature from 36.9°C to 41.1°C and the lower eyelid temperature from 37.0°C to 42.0°C1). A single treatment significantly improves meibum secretion score, Ocular Surface Disease Index (OSDI), Standard Patient Evaluation of Eye Dryness (SPEED), and tear break-up time (TBUT) at 1 month, with long-term results lasting up to 3 years1). An RCT of 400 eyes showed that a single LipiFlow treatment was significantly superior to twice-daily 10-minute warm compresses plus eyelid hygiene, with 86% of patients requiring no additional treatment at 12 months1). It has also been shown to be at least as effective as a 3-month course of oral doxycycline1). The new semi-transparent activator (Activator Clear) facilitates placement confirmation and has achieved a 100% treatment completion rate2). This therapy is not covered by insurance in Japan. A similar device, MiBo Thermoflo®, heats with an external paddle at 42.2°C but has a smaller effect on eyelid temperature elevation1).
Intraductal probing: A Maskin probe (1 mm → 4/6 mm stepwise) is inserted into the obstructed duct to physically open it1). In a cohort of 25 cases, 96% obtained immediate symptom improvement, but in a 49-case RCT, objective findings showed limited improvement1). Because it is invasive and provides little improvement in objective findings, it is usually not performed3).
The main procedures performed in the outpatient setting are as follows.
Meibum expression: Performed to expel obstructive material and improve gland function. The Arita-style meibomian gland expression forceps (Inami) are designed to reduce pain during expression. Treatment is continued at intervals of 10 days to 1 month, combined with home warm compresses and eyelid hygiene. The expressed meibum in hyposecretory MGD is cloudy or toothpaste-like.
Plugging removal: If a large plugging causes discomfort, remove it with forceps after topical anesthesia. If the obstruction is deep within the orifice, press the lid margin with a cotton swab or use meibum expression forceps. If a meibomian gland infarction protrudes like wax, incise and remove it with an injection needle.
Internal hordeolum puncture: If a pus point is clearly visible, puncture with a 21–25G injection needle, express pus with a cotton swab, and prescribe antibiotics.
Chalazionsteroid injection: Using a 1 mL syringe and 27–28G needle, inject triamcinolone acetonide 2 mg (Kenacort-A® 40 mg/mL, 0.05 mL) into the mass from the conjunctival side. The cure rate with 1–2 injections is 60–90%, equivalent to chalazion excision. Healing time is about 5 days to 2.5 weeks. Injecting from the conjunctival side rather than the skin side prevents white drug deposits and skin depigmentation. If no improvement after 2 injections, consider IPL treatment. If sebaceous carcinoma is suspected, perform surgery for pathological examination.
Medical fee: Warm compresses, meibum expression, plugging removal, and internal hordeolum puncture are billed as “ocular procedures.” Meibum expression and plugging removal are coded under the diagnosis “meibomian gland infarction.” Kenacort-A® is not covered by insurance for the diagnosis “chalazion” but can be claimed as “symptomatic treatment of inflammatory diseases of the external eye.”
Details of antibiotics and anti-inflammatory drugs
Tetracyclines: Doxycycline and minocycline are more lipophilic than tetracycline and accumulate in ocular tissues and eyelids at low doses1). They are used primarily for anti-inflammatory rather than antibacterial effects, controlling inflammation by inhibiting MMP-8, MMP-9, TNF-α, lipase production, and free fatty acid production1). A 60-case RCT reported that the minocycline combination group showed significant improvement in all clinical parameters and IL-6, IL-1β, IL-17α, TNF-α, and IL-12p70 compared to the control group1), 13). Side effects include photosensitivity and gastrointestinal symptoms; they are contraindicated in pregnant women and children14).
Azithromycin: A macrolide that binds to the 50S ribosomal 23S rRNA and inhibits bacterial protein synthesis. In addition to its antibacterial action, it suppresses the expression of NF-κB, IL-6, IL-8, TNF-α, and MMP-9, and induces anti-inflammatory TGF-β11). A 1% ophthalmic formulation (AzaSite®, USA) is available, and short-term administration has been reported to provide therapeutic effects lasting 3 months. Oral azithromycin is used in regimens of 500 mg for 3 days for 3 cycles (7-day intervals) or 1 g once weekly for 3 weeks, but there is a risk of QT prolongation, requiring caution in patients with a history of cardiac disease1).
Cyclosporine A 0.05% ophthalmic: Approved in the USA as Restasis® for aqueous-deficient dry eye. It inhibits T-cell IL-2 production and exerts anti-inflammatory effects1). Its efficacy for MGD alone is limited, and it is not usually used as monotherapy3).
Lifitegrast 5.0% ophthalmic: An LFA-1 antagonist approved by the US FDA for dry eye. Dedicated evidence for MGD has not been established1).
Oral omega-3 fatty acids: Supplementation with EPA/DHA alters the fatty acid composition of meibum1). The DREAM study (n=499) reported in 2018 no significant differences in OSDI, Schirmer, or BUT between the omega-3 and control groups, and evidence is conflicting1). In Japan, these are considered supplements, so they are considered adjunctively3).
Demodex infestation increases with age, reaching 100% in those aged 70 years and older1). Demodex folliculorum parasitizes the eyelash roots, and Demodex brevis parasitizes the meibomian glands and sebaceous glands. The former causes reactive hyperkeratosis and forms cylindrical dandruff, while the latter causes gland obstruction and granulomatous reactions1).
Tea tree oil (TTO: derived from Melaleuca alternifolia) is effective for demodicosis1). Specifically, a protocol using 50% TTO lid scrub once a week in the clinic and 10% TTO daily at home for one month has been reported to reduce eyelid margin inflammation, decrease tear IL-1β and IL-17 levels, and improve ocular surface irritation symptoms1). The active anti-mite component of TTO is terpinen-4-ol, and commercial products such as Cliradex® are available1). Oral ivermectin 200 μg/kg as a single dose (day 0 and day 7) has also been reported to improve Demodex counts, Schirmer, and BUT in refractory posterior blepharitis1).
Zhang et al. reported a case of a 46-year-old male with MGD who had few external findings and no Demodex detected by eyelash epilation, but 15 D. brevis were directly detected in expressed meibum after lid margin disinfection, and symptoms improved with TTO lid scrub 6). This is an important case demonstrating the usefulness of direct meibum microscopy for Demodex detection.
QWhat tests are used to diagnose MGD?
A
According to the diagnostic criteria of the Japanese MGD Working Group 2010, all three of the following items must be positive: (1) subjective symptoms such as ocular discomfort, (2) abnormal findings around the orifice (one or more of vascular dilation, MCJ migration, and irregular lid margin), and (3) orifice obstruction findings (both plugging and reduced expression of grade 2 or higher on the Shimazaki scale). Meibography and meibum observation are also useful as supplementary tests.
QHow should warm compresses be performed?
A
Wet a clean towel and warm it in a microwave, or apply a commercially available warm eye mask to both eyes for 5 to 10 minutes. It is important to maintain the eyelid temperature at around 40°C; note that a hot towel tends to cool down due to evaporative heat. A guideline is to continue for at least 5 minutes twice a day. Gently massaging the eyelids after warming promotes the expulsion of melted meibum.
The main pathology of hyposecretory MGD is summarized as “hyperkeratinization of the ductal epithelium and atrophy of the acini” 3). Acinar atrophy may occur not only secondary to meibomian gland obstruction but also as a primary impairment of gland cells due to aging, among other causes.
Progression from ductal obstruction to acinar atrophy
Hyperkeratinization of the ductal epithelium and increased meibum viscosity cause obstruction of the terminal ducts 1). Obstruction leads to increased intra-acinar pressure, progressing to acinar atrophy and loss. Gland loss reduces lipid secretion, thinning the tear film lipid layer.
Elevation of meibum melting point
Normal meibum has a melting point of about 19–32°C and remains fluid at the ocular surface temperature of 33–37°C 1). In MGD, an increase in sphingolipids such as ceramides raises the meibum melting point; in severe cases, it may not liquefy unless heated above 40°C 1). This is the rationale for warm compresses and thermal pulsation therapy.
Influence of sex hormones
Androgens activate lipid synthesis genes and suppress keratinization-related genes in meibocytes (meibomian gland cells) 1). Androgen deficiency, receptor dysfunction, or administration of antiandrogen drugs are associated with obstructive MGD. Conversely, estrogen promotes lipid catabolism and stimulates the production of inflammatory cytokines such as IL-6 and TNF-α 1). The association between postmenopausal hormone replacement therapy and dry eye is partially explained by decreased adrenal androgen production due to hypothalamic-pituitary-adrenal axis suppression 1).
Contribution of bacteria and inflammation
Lipases produced by commensal bacteria (mainly staphylococci) on the eyelid margin break down meibum lipids, increasing free fatty acids that trigger inflammation 1). In patients with blepharitis, increased lipase activity and matrix metalloproteinase (MMP) production have been observed. In the tear fluid of MGD patients, concentrations of IL-1α, mature IL-1β, MMP-9, IL-6, IL-8, and TNF-α are elevated and correlate with the severity of ocular surface epithelial damage 1). IL-1 promotes epithelial cell proliferation and hyperkeratinization, forming a vicious cycle in obstructive MGD.
PPAR-γ (peroxisome proliferator-activated receptor γ) belongs to the nuclear receptor superfamily and acts as a transcription factor involved in lipid synthesis and sebocyte differentiation. It is thought to play an important role in meibocyte differentiation and lipid synthesis, and is attracting attention as a target for elucidating the pathogenesis of MGD 3).
Sphingolipids and melting point
In MGD, the proportion of ceramides and sphingolipids in meibum increases, reducing the stability of the meibum lipid film 1). The rise in ceramide content directly increases the melting point of meibum, making it liquefy only when heated above 40°C. Sphingolipids not only alter the physicochemical properties of meibum but also regulate cellular processes such as cell proliferation, differentiation, apoptosis, and inflammation, further complicating the pathogenesis of MGD 1).
Diabetes and ocular surface changes
Type 2 diabetes is an exacerbating factor for MGD. A cross-sectional study of 302 eyes by Hao et al. reported that the DED-DM group showed significantly worse upper eyelid margin irregularity, eyelid margin vascular dilation, orifice plugging grade, eyelid margin thickening, upper meibomian gland dropout, ciliary injection, and noninvasive breakup time (NIBUT) compared to the DED-only group, and that blood glucose levels were significantly correlated with NIBUT, eyelid margin thickening, and eyelid margin irregularity 7). A pathogenic mechanism involving chronic inflammation and microvascular damage affecting the eyelid margin and glandular tissue has been proposed.
LipiFlow Translucent Activator: The new semi-transparent activator (Activator Clear) of LipiFlow facilitates confirmation of placement position due to its translucent material, and Hu et al. reported a 100% treatment completion rate2). Improvement in subjective symptoms and meibum score up to 3 months after treatment has been confirmed. In a long-term observational study by Blackie et al., a single LipiFlow treatment sustained improvement in meibum secretion and dry eye symptoms for 12 months, with 86% not requiring additional treatment15).
Intranasal neurostimulation: Pulsed stimulation of the anterior ethmoidal nerve in the nasal cavity induces lacrimal gland secretion via the nasolacrimal reflex pathway. In animal experiments, daily stimulation for 3 minutes over 3 weeks increased tear volume, lipid and protein concentrations, and decreased tear osmolarity1). In human RCTs, the Allergan TrueTear® Intranasal Tear Neurostimulator (ITN) has been reported to induce conjunctival goblet cell degranulation, increase tear meniscus height, raise meibomian gland temperature in the central lower eyelid, and increase tear film lipid layer thickness1). A non-randomized open-label study reported improvements in Schirmer values, corneal and conjunctival staining, and subjective symptoms with use 4 or more times daily for 180 days1). Findings also show that intranasal stimulation immediately changes meibomian gland morphology (area and perimeter), suggesting it may become a new therapeutic strategy for promoting meibum secretion through neuromodulation1).
Sex hormone therapy: In a multicenter randomized trial by Schiffman et al., topical testosterone ophthalmic solution (0.03%) significantly improved the viscosity of meibomian gland secretions compared to the control group after 6 months of treatment, as reported at the ARVO abstract stage1). Some studies have shown that topical androgens increase tear film lipid layer thickness and BUT, but currently no approved ophthalmic product exists in Japan or the United States1). Application of 5% testosterone cream in menopausal women (OSDI improvement), transdermal DHEA in postmenopausal patients, and ophthalmic application of female hormone replacement therapy are also discussed, but all lack sufficient evidence and have not been introduced into daily clinical practice1).
IL-1 receptor antagonist (Anakinra): Recombinant human IL-1RA (Kineret™) is a biologic approved for rheumatoid arthritis, and off-label use in dry eye has shown efficacy1). Since IL-1 in the tear fluid of MGD patients plays a central role in pathogenesis, it is a promising therapeutic target, but clinical trial results for MGD have not yet been published1).
Induction of gland morphological changes by IPL: A cohort study of 35 cases reported that IPL induced an increase in the longest diameter of acini and unit density, and reduced inflammatory cells around the glands1). This suggests the possibility of tissue repair effects beyond mere symptomatic treatment.
Meibomian gland gene expression profile: In MGD, changes in the expression of over 400 genes in the meibomian gland have been reported. Androgen-responsive genes, keratinization-related genes, and lipid synthesis-related genes are considered major targets, and the possibility of molecular targeted therapy is being explored1).
Mibo Thermoflo®, IRPL, and low-level laser: Comparative trials of new devices such as external heating devices, IRPL (broadband light), and low-level laser are ongoing, but no device has been reported to show efficacy exceeding that of LipiFlow at this time1).
In MGD treatment, there are many areas with limited evidence, and accumulation of evidence through Japan-led RCTs is a future challenge3). In particular, there is a need for establishment of standardized protocols for conservative treatments feasible in Japan (warm compresses, eyelid hygiene, meibum expression), domestic trials for expanding insurance coverage of doxycycline and azithromycin, and multicenter trials for regulatory approval of IPL and LipiFlow.
Sabeti S, Kheirkhah A, Yin J, Dana R. Management of meibomian gland dysfunction: a review. Surv Ophthalmol. 2020;65(2):205-217. doi:10.1016/j.survophthal.2019.08.007.
Hu JG, Dang VT, Chang DH, Goldberg DF, McKinnon C, Makedonsky K, et al. Performance of a Translucent Activator for LipiFlow Vectored Thermal Pulse (VTP) Treatment of Meibomian Gland Dysfunction. Clinical ophthalmology (Auckland, N.Z.). 2022;16:963-971. doi:10.2147/OPTH.S354738. PMID:35386613; PMCID:PMC8977218.
Arita R, Itoh K, Inoue K, Amano S. Noncontact infrared meibography to document age-related changes of the meibomian glands in a normal population. Ophthalmology. 2008;115(5):911-915. doi:10.1016/j.ophtha.2007.06.031.
Zhang N, Liang L. Demodex in Meibum. Ophthalmology. 2024.
Hao Y, Wu B, Feng J, He J, Zang Y, Tian L, et al. Relationship between type 2 diabetes mellitus and changes of the lid margin, meibomian gland and tear film in dry eye patients: a cross-sectional study. International ophthalmology. 2025;45(1):261. doi:10.1007/s10792-025-03636-w. PMID:40553413; PMCID:PMC12187884.
Jones L, Craig JP, Markoulli M, Karpecki P, Akpek EK, Basu S, et al. TFOS DEWS III: Management and Therapy. American journal of ophthalmology. 2025;279:289-386. doi:10.1016/j.ajo.2025.05.039. PMID:40467022.
Nelson JD, Shimazaki J, Benitez-del-Castillo JM, Craig JP, McCulley JP, Den S, et al. The international workshop on meibomian gland dysfunction: report of the definition and classification subcommittee. Investigative ophthalmology & visual science. 2011;52(4):1930-7. doi:10.1167/iovs.10-6997b. PMID:21450914; PMCID:PMC3072158.
Arita R, Minoura I, Morishige N, Shirakawa R, Fukuoka S, Asai K, et al. Development of Definitive and Reliable Grading Scales for Meibomian Gland Dysfunction. American journal of ophthalmology. 2016;169:125-137. doi:10.1016/j.ajo.2016.06.025. PMID:27345733.
Shimazaki J, Sakata M, Tsubota K. Ocular surface changes and discomfort in patients with meibomian gland dysfunction. Arch Ophthalmol. 1995;113(10):1266-1270. doi:10.1001/archopht.1995.01100100054027.
Lee H, Min K, Kim EK, Kim TI. Minocycline controls clinical outcomes and inflammatory cytokines in moderate and severe meibomian gland dysfunction. American journal of ophthalmology. 2012;154(6):949-957.e1. doi:10.1016/j.ajo.2012.06.009. PMID:22967863.
Wladis EJ, Bradley EA, Bilyk JR, Yen MT, Mawn LA. Oral antibiotics for meibomian gland-related ocular surface disease: a Report by the American Academy of Ophthalmology. Ophthalmology. 2016;123(3):492-496. PMID: 26707417.
Blackie CA, Coleman CA, Holland EJ. The sustained effect (12 months) of a single-dose vectored thermal pulsation procedure for meibomian gland dysfunction and evaporative dry eye. Clin Ophthalmol. 2016;10:1385-1396. doi:10.2147/OPTH.S109663.
Arita R, Itoh K, Inoue K, Kuchiba A, Yamaguchi T, Amano S. Contact lens wear is associated with decrease of meibomian glands. Ophthalmology. 2009;116(3):379-384. doi:10.1016/j.ophtha.2008.10.012. PMID: 19167077.