Phlyctenular keratoconjunctivitis (PKC) is a disease in which nodular inflammation of the cornea or conjunctiva occurs due to a T-cell-dependent type IV (delayed-type) hypersensitivity reaction to exogenous antigens. Based on the lesion site, it is classified into conjunctival phlycten, limbal phlycten, and corneal phlycten, collectively referred to as phlyctenular keratoconjunctivitis.
Historically, this disease has been discussed in relation to tuberculosis, but it is now understood as a delayed-type hypersensitivity reaction to bacterial antigens associated with blepharitis and meibomianitis, not limited to Mycobacterium tuberculosis. In tuberculosis-endemic areas or children with a history of tuberculosis exposure, tuberculosis-related PKC should still be considered in the differential diagnosis2).
Clinical studies from Japan have reported in detail the association between phlyctenular keratitis and meibomian gland inflammation in young patients, showing the involvement of C. acnes, a history of chalazion, and a higher prevalence in young women1). Since then, the concept of treating phlyctenular keratoconjunctivitis as the phlyctenular type of MRKC has been widely adopted in Japan1,3).
PKC is common in children and young adults. In Japanese series of young patients, female sex, history of chalazion, and concurrent meibomian gland inflammation are prominent1). In regions with a high prevalence of tuberculosis, Mycobacterium tuberculosis remains an important cause of childhood PKC, and cases of PKC associated with tuberculosis have been reported even after 20002).
QIs phlyctenular keratoconjunctivitis a disease that commonly affects children?
A
It is a disease that predominantly occurs in children and adolescents, especially in girls. Children with a history of chalazion or meibomian gland inflammation are prone to recurrence. Onset in adults is relatively rare, but cases with underlying blepharitis can occur at any age. In adults and the elderly, it may present as similar ocular surface inflammation against a background of blepharitis or dry eye-like superficial keratopathy.
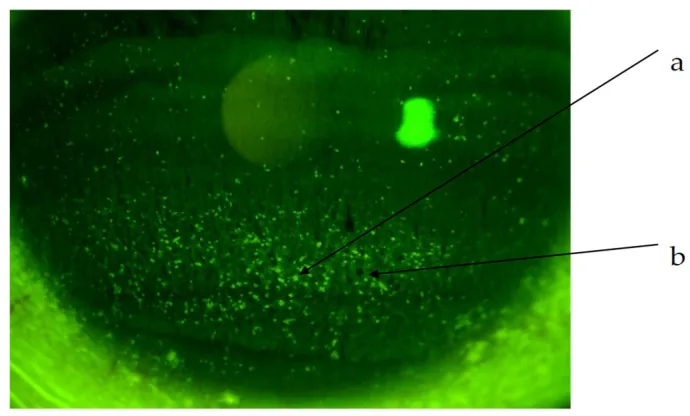
Diagnostics (Basel). 2024 Feb 23; 14(5):487. Figure 2. PMCID: PMC10930652. License: CC BY.
Under fluorescein staining, granular corneal epithelial lesions and staining abnormalities are shown. The image demonstrates the involvement of the pupillary area, making it useful for explaining clinical findings.
Redness and foreign body sensation: The most common chief complaints. In cases of isolated conjunctival phlyctenules, symptoms are often mild to moderate ocular irritation.
Eye pain and photophobia: These become prominent when corneal lesions are present. Photophobia is severe in serious cases, and tuberculosis-associated PKC tends to present with more intense photophobia2).
Tearing: Caused by superficial inflammation and nerve stimulation.
Visual impairment: Occurs when lesions involve the central cornea or when severe cases lead to corneal thinning and opacification.
White to yellow nodule near the limbus. Associated with superficial vascular aggregation and epithelial defect.
Limbal phlycten
Nodular elevation at the corneal limbus. May be accompanied by vascular invasion.
Corneal phlycten
Nodular infiltration with superficial vascular invasion toward the nodule (fascicular keratitis).
Migratory phlycten
A form that progresses across the corneal surface. Elevated leading edge with a trailing vascular bundle.
Conjunctival phlycten is a white to yellow nodular elevated lesion on the bulbar conjunctiva near the corneal limbus, accompanied by superficial vascular aggregation and epithelial defect. It commonly occurs in the interpalpebral fissure.
Corneal phlycten commonly occurs in the lower peripheral cornea but can also occur in the interpalpebral fissure. It is characterized by a white, oval nodular cellular infiltration in the cornea with superficial vascular invasion toward it and corresponding bulbar conjunctival hyperemia. In severe cases, corneal opacity and thinning occur, leading to significant visual impairment. Because neovascularization forms in a bundle toward the nodular lesion, it is also called fascicular keratitis.
Migratory phlyctenules (marching phlyctenules) involve phlyctenules that progress across the corneal surface. They present with an elevated leading edge and a trailing vascular bundle.
In the domestic concept of MRKC, clinical findings are generally classified into the following two types1,3).
Phlyctenular type: Characterized by nodular cellular infiltration and superficial vascular invasion in the cornea. More common in young women, and an association with C. acnes has been suggested1).
Non-phlyctenular type: Without cellular infiltration, mainly presenting with superficial punctate keratopathy (SPK). Against a background of blepharitis and meibomianitis, involvement of C. acnes and staphylococci is presumed.
A multicenter cross-sectional study reported that the severity of meibomian gland inflammation correlates with the severity of keratitis, and that patients with phlyctenular MRKC have more morphological changes such as dropout and loss of meibomian glands 3).
Meibomianitis: Characterized by redness, swelling, and obstruction of the gland openings; its severity correlates with the severity of keratoconjunctival inflammation.
History of chalazion: Many patients have recurrent chalazia before onset. This is considered a reflection of local meibomian gland inflammation.
Anterior/posterior blepharitis: Patients with underlying rosacea or seborrheic dermatitis often have concurrent blepharitis.
Important in young MRKC: Formerly Propionibacterium acnes. It has been reported to be frequently detected in phlyctenular MRKC in young women 1). It colonizes the meibomian glands, and its bacterial antigens trigger a type IV hypersensitivity reaction.
Staphylococcus aureus
Important in blepharitis-related MRKC: Staphylococcal proteins associated with chronic blepharitis are considered representative antigens that induce delayed-type hypersensitivity on the ocular surface. In non-phlyctenular MRKC, involvement of C. acnes and S. aureus is presumed.
Mycobacterium tuberculosis
Important in tuberculosis-endemic areas: Caused by hypersensitivity to tuberculin protein of Mycobacterium tuberculosis. Since 2000, cases of childhood tuberculous PKC have been reported, including not only pulmonary and lymph node tuberculosis but also sinus tuberculosis 2). In children with PKC from endemic areas, tuberculosis screening should be performed 2).
Viruses and Others
Causes of atypical cases: Herpes simplex virus (HSV), especially HSV-2-related PKC, has been reported 4). Other causes include Chlamydia, Dolosigranulum pigrum, and intestinal parasites (Hymenolepis nana).
History of tuberculosis exposure or residence in a TB-endemic area: The risk of TB-associated PKC increases 2).
Atopic predisposition: Can be associated with chronic eyelid inflammation.
Contact lens wear: A risk factor for chronic ocular surface irritation and changes in the bacterial flora.
QIs there a link with tuberculosis?
A
Tuberculin protein from Mycobacterium tuberculosis is one of the classic causative antigens of PKC. In developed countries, C. acnes and Staphylococcus aureus are the main causes, but in TB-endemic areas, tuberculosis remains an important cause 2). In children with PKC, especially those from TB-endemic areas, screening with chest X-ray, tuberculin skin test (Mantoux test), and QuantiFERON-TB Gold test is recommended. TB-associated PKC requires systemic anti-tuberculosis therapy 2).
The diagnosis of PKC is based on the medical history and characteristic clinical findings. The presence of nodular lesions near the corneal limbus and superficial vascular aggregation, along with meibomianitis, makes the diagnosis almost certain. In young women with a history of chalazion, the presence of nodular cell infiltration and superficial vascular invasion makes diagnosis straightforward.
Slit-lamp microscopy: Observe at low magnification with diffuse light to confirm the presence of meibomianitis. The presence of redness, swelling, or obstruction of the meibomian gland openings is important.
Fluorescein staining: Evaluate epithelial defects at the nodule site and distribution of SPK.
Observation of meibomian glands: Meibography or in vivo confocal microscopy (IVCM) is useful to evaluate loss and morphological changes of meibomian glands3).
If tuberculosis is suspected, perform chest X-ray, tuberculin skin test (PPD/Mantoux), and QuantiFERON-TB Gold test. In a case report by Wiriyachai et al., even when routine culture, staining, and PCR were negative, PCR using formalin-fixed paraffin-embedded (FFPE) tissue detected Mycobacterium tuberculosis2). A literature review in the same paper reported pediatric PKC associated with pulmonary tuberculosis, lymph node tuberculosis, cutaneous tuberculosis, and sinus tuberculosis2).
If chlamydia is suspected, perform conjunctival swab immunofluorescence or PCR. If herpes simplex virus is suspected, perform HSV-1/HSV-2 IgG and IgM serology and conjunctival swab PCR4).
Associated with collagen disease. Accompanied by limbal ulceration, infiltration, and scleritis.
Herpetic keratitis
Dendritic lesions or geographic ulcers. HSV-2-related PKC has been reported, requiring differentiation 4).
Other differential diagnoses include rosacea keratitis, trachoma, infectious corneal ulcer, and Acanthamoeba keratitis. In severe recurrent cases, cell infiltration and vascular invasion may be pronounced and mistaken for necrotizing keratitis, but differentiation is possible based on the presence or absence of severe meibomianitis.
The core of treatment consists of three pillars: reduction of antigen load by controlling meibomianitis, suppression of ocular surface inflammation, and treatment of underlying infection1,3). The basic approach is a combination of antibacterial eye drops and low-concentration steroid eye drops, and in cases with meibomianitis, oral antibiotics should be actively combined.
Conjunctival phlyctenule is mainly treated with antibacterial eye drops plus low-concentration steroid eye drops. In cases complicated by meibomianitis, oral cefcapene or oral clarithromycin is added.
Corneal phlyctenule additionally benefits from application of Ecolicin® eye ointment to the meibomian gland openings. In the early stage with severe ocular surface inflammation, antibacterial drugs and steroids are used together, and antibacterial-centered treatment is continued until bacteria are sufficiently eliminated.
Treatment based on the MRKC concept involves controlling ocular surface inflammation and treating meibomianitis in parallel 1,3).
Initial: Administer oral cephem antibiotics (e.g., cefcapene) with bactericidal action to rapidly reduce bacterial load in the meibomian glands.
Maintenance: Switch to macrolide antibiotics (clarithromycin, azithromycin) with bacteriostatic action, continue for several weeks to months depending on meibomianitis activity, and normalize the bacterial flora of the meibomian glands.
Eyelid hygiene: Continue warm compresses and eyelid cleansing to reduce the amount of antigenic bacteria.
For refractory or steroid-dependent cases, cyclosporine A eye drops are an effective option. They have the advantage of avoiding the risks of cataracts and secondary glaucoma associated with long-term steroid use.
When considering oral doxycycline in children, erythromycin or clarithromycin is recommended for those under 8 years of age due to the risk of tooth discoloration.
Tuberculosis-related PKC requires systemic administration of antituberculosis drugs 2). In a case of PKC with sinus tuberculosis in a 7-year-old boy reported by Wiriyachai et al., standard multidrug antituberculosis therapy improved the ocular lesions 2).
For HSV-associated PKC, consider systemic antiviral therapy 4). In a case report by Khan et al., improvement was reported after adding antivirals for conjunctival phlyctenules and nodular scleritis suspected to be associated with HSV-2 exposure 4). Since steroid monotherapy may worsen HSV-related lesions, it is important to investigate infectious causes in atypical cases.
QHow long does treatment take?
A
Conjunctival phlyctenules may resolve spontaneously within 1–2 weeks, but improve within days to 1 week with topical steroids. Corneal phlyctenules often require longer treatment. In recurrent cases associated with meibomianitis, eyelid hygiene and oral antibiotics should be continued for several weeks to months. For tuberculosis-associated PKC, antitubercular drugs are needed for a duration according to systemic tuberculosis treatment 2). For refractory HSV-related cases, consider continuing antiviral therapy 4).
QWhy is treatment of meibomianitis important?
A
Many of the causative antigens in phlyctenular keratoconjunctivitis originate from bacteria such as C. acnes and Staphylococcus aureus that colonize the meibomian glands. Studies on MRKC in Japan and abroad have shown a correlation between the severity of meibomianitis and ocular surface inflammation 1,3). Even if inflammation is suppressed with topical steroids alone without controlling meibomianitis, recurrence will persist as long as antigen exposure continues. Physical reduction of bacterial load through warm compresses and eyelid hygiene, along with normalization of the meibomian gland microbiota using oral cephalosporins and macrolides, is important as a curative treatment strategy 1,3).
The essence of PKC is inflammatory cell infiltration due to a delayed-type (type IV) allergic reaction to local bacterial proteins. Antigen-presenting cells (Langerhans cells) take up microbial antigens and present them to sensitized helper T cells via major histocompatibility complex class II (HLA-DR). Activated T cells release cytokines such as interferon-γ and IL-2, recruiting monocytes and macrophages to the lesion, forming granulomatous nodular lesions.
Histologically, scrapings from the infiltrated area show helper T cells, suppressor/cytotoxic T lymphocytes, monocytes, and Langerhans cells, with most cells being HLA-DR positive, supporting the involvement of cell-mediated immune reactions.
Since the concept of MRKC was proposed, it is thought that persistent exposure of the ocular surface to lipases and bacterial proteins produced by bacteria colonizing the meibomian glands (especially C. acnes and staphylococci) triggers phlycten formation 1,3). In a multicenter cross-sectional study of patients with phlyctenular MRKC, Suzuki et al. reported that morphological changes such as dropout and loss of meibomian glands were frequently observed, indicating that meibomian gland pathology itself is associated with phlycten formation 3).
Chalazion is a phenotype of focal meibomian gland obstruction plus inflammation (focal obstructive MGD) and is considered an important accompanying finding of MRKC 1,3).
The corneal limbus is a special area where the vascular, immune, and nervous systems are densely packed, and it is rich in Langerhans cells and lymphoid tissue. This accumulation of immune system components is thought to be the reason why phlyctens preferentially occur at the limbus. In corneal phlycten, superficial blood vessels invade in a bundle toward the nodular infiltration, presenting the typical findings of fascicular keratitis.
In patients sensitized to tuberculin protein of Mycobacterium tuberculosis, local type IV reactions are triggered by minimal antigen exposure on the ocular surface. PKC does not necessarily correlate with tuberculosis activity; the presence of hypersensitivity to tuberculin protein is a prerequisite for onset. In children living in tuberculosis-endemic areas or with a history of tuberculosis exposure, PKC should be considered a clinical warning sign of tuberculosis 2).
Azithromycin eye drops and oral administration: The efficacy of oral azithromycin (pulse therapy) for MRKC and ocular rosacea-associated PKC has been increasingly reported.
In vivo imaging of meibomian glands: Morphological evaluation of meibomian glands using IVCM (in vivo confocal microscopy) and meibography is developing as a tool for diagnosis and treatment effect assessment of MRKC 3).
Microbiome research of meibomian glands: Analysis of the meibomian gland bacterial flora using next-generation sequencing is investigating the relationship between the balance of C. acnes and S. aureus and MRKC disease type.
Suzuki T, Mitsuishi Y, Sano Y, Yokoi N, Kinoshita S. Phlyctenular keratitis associated with meibomitis in young patients. Am J Ophthalmol. 2005;140(1):77-82. doi:10.1016/j.ajo.2005.02.039. PMID:15953578.
Wiriyachai T, Boonsathorn S, Apiwattanakul N, Assawawiroonhakarn S. A rare case of primary sinonasal tuberculosis presented with phlyctenular keratoconjunctivitis in a pediatric patient: a case report and literature review. Medicine (Baltimore). 2021;100(7):e24787. PMID:33607832.
Suzuki T, Morishige N, Arita R, Koh S, Sakimoto T, Shirakawa R, et al. Morphological changes in the meibomian glands of patients with phlyctenular keratitis: a multicenter cross-sectional study. BMC Ophthalmol. 2016;16:178. doi:10.1186/s12886-016-0347-5. PMID:27724848.
Khan S, Saigal K, Maleki A. Conjunctival Phlyctenule and Nodular Scleritis in a Patient with Previous Herpes Simplex Virus-2 Exposure: Causative Agent or Innocent Bystander? Case Rep Ophthalmol. 2024;15(1):777-783. doi:10.1159/000542076. PMID:39544433; PMCID:PMC11563655.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.