Bacterial keratitis is a purulent inflammation caused by bacteria invading and proliferating in the corneal stroma. It is also known as bacterial corneal ulcer, and particularly when caused by Streptococcus pneumoniae, it is called serpiginous corneal ulcer. It is the most common type of infectious keratitis and can lead to severe visual impairment if initial diagnosis and treatment are incorrect1).
In Japan, the age distribution of patients with infectious keratitis shows a bimodal pattern with peaks in the 20s and 60s1). The peak in younger individuals is mostly due to infections associated with contact lens (CL) use. There is no clear sex difference in incidence, but trauma-related infections are more common in men, while CL-related infections are more common in women1).
According to large cohort studies, the annual incidence in developed countries ranges from a few to several dozen per 100,000 population, while in developing countries it can reach several hundred per 100,0001). Bacteria are the most common causative microorganisms of infectious keratitis, followed by viruses, fungi, and Acanthamoeba1). In the United States, an estimated 71,000 cases of microbial keratitis (including bacterial, fungal, and Acanthamoeba) occur annually, with an increasing trend in recent years7). Regarding visual prognosis, some cases do not recover vision due to irregular astigmatism or corneal scarring even after healing, and central ulcers are particularly likely to result in visual impairment1).
In Japan, the most common trigger is CL use, similar to other developed countries1). Severe CL-related keratitis is often associated with users of 2-week frequent replacement soft CL (FRSCL) or conventional SCL, and poor lens care is an important risk factor1). It should also be noted that CL-related infectious keratitis is frequently bilateral. In the United States, CL use is the main trigger, while in developing countries, trauma is the most common cause7).
The four major causative bacteria of bacterial keratitis are Staphylococcus aureus, Streptococcus pneumoniae, Pseudomonas aeruginosa, and Moraxella. Among them, Staphylococcus species are the most frequent, and Pseudomonas aeruginosa is the main causative agent in CL-related keratitis1). Moraxella has been increasingly reported both in Japan and abroad, with ocular surface diseases, history of ocular surgery, and diabetes as triggers1). Corynebacterium, a normal flora of the ocular surface, is also a relatively common causative bacterium1).
Mixed infections are also not negligible; the AAO PPP reports that about 43% of culture-positive cases yield two or more bacterial species7). The most common trigger for mixed infections is trauma, with the combination of Staphylococcus epidermidis and Fusarium species being frequent7). Ung et al. describe infectious keratitis as a “persistent clinical challenge” and emphasize the importance of rapid microbiological testing, new antimicrobial agents, and monitoring regional differences in resistant strains11).
The term “serpiginous corneal ulcer” has been used since the 19th century, named for the characteristic creeping movement of the lesion across the corneal surface. In Japan, the clinical practice guidelines for infectious keratitis were first published in the Journal of the Japanese Ophthalmological Society in 2007, followed by revisions in 2013 (2nd edition)12) and 2023 (3rd edition), promoting evidence-based standardization of care1).
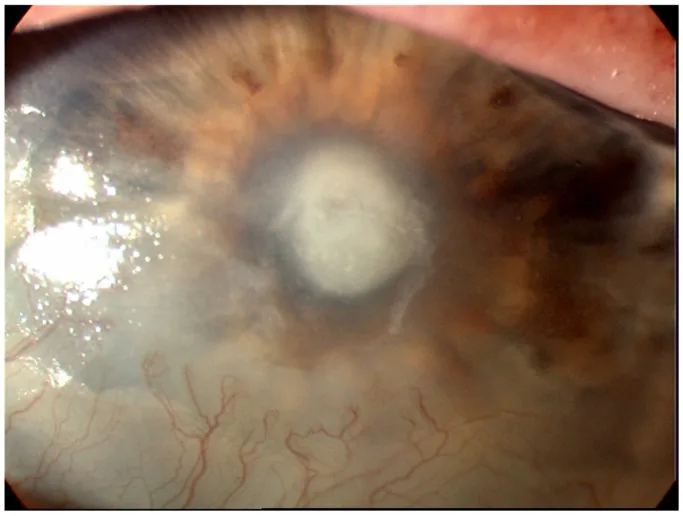
Cabrera-Aguas M, Watson SL. Updates in Diagnostic Imaging for Infectious Keratitis: A Review. Diagnostics (Basel). 2023 Oct 31;13(21):3358. Figure 1. PMCID: PMC10647798. License: CC BY.
A clinical photograph of bacterial keratitis showing a white infiltrate in the central cornea with an overlying epithelial defect. The ulcer base and surrounding opacity appear continuous.
Acute onset of eye pain is characteristic. In mild cases, patients complain of a foreign body sensation, while in severe cases, intense eye pain is reported1). In addition to pain, symptoms include redness, visual impairment, tearing, mucopurulent discharge, and photophobia1). The speed of progression correlates with the virulence of the causative bacteria; for example, Pseudomonas aeruginosa can worsen rapidly within 24 hours of onset7).
The initial lesions of bacterial keratitis are infiltration, epithelial defect, appearance of inflammatory cells in the anterior chamber, and ciliary injection. However, true initial lesions are rarely observed; patients usually present with a round corneal abscess. Corneal findings differ significantly between Gram-positive cocci and Gram-negative rods, providing important clues for inferring the causative organism based on clinical appearance 1).
In severe cases, hypopyon and fibrin exudation are observed, with a high likelihood of posterior synechiae. Keratic precipitates (KP) appear on the posterior surface corresponding to the corneal infiltration, abscess, or ulcer 1).
Slit-lamp examination is useful: use diffuse illumination to assess overall opacity, retroillumination to evaluate cellular infiltration and anterior chamber inflammation (especially KP), a broad slit beam to examine the corneal surface, a narrow slit beam to assess lesion depth and anterior chamber inflammation, and fluorescein staining to delineate epithelial defects.
Gram-positive cocci
Staphylococci: Typically present as small, round, relatively well-demarcated gray-white localized abscesses 1). Progression is slow, but MRSA tends to be more severe and is often associated with epithelial defects larger than the infectious focus 1). In patients with atopic dermatitis, MRSA is detected at a high rate.
Streptococcus pneumoniae: Shows characteristic findings known as serpiginous corneal ulcer. One edge of the lesion heals while the other progresses, giving the appearance of creeping movement 1). The capsule resists phagocytosis by neutrophils, allowing deep extension and potential corneal perforation 1).
Gram-negative rods
Pseudomonas aeruginosa: Presents with ring-shaped abscess and ground-glass opacity of the surrounding cornea1). Protease-induced corneal melting leads to rapid progression and perforation. Often associated with contact lens use; cases of ring ulcer have been reported with long-term combined use of orthokeratology and contact lenses 3).
Moraxella: Forms a localized, well-demarcated ulcer in the central cornea1). Risk factors include contact lens wear and underlying diseases such as diabetes 1). Progression is relatively slow, and it is susceptible to many antibiotics.
Serratia: Presents with a variety of findings from mild superficial ulcers to extensive abscesses; the amount of protease production correlates with severity 1).
Special causative organisms
Neisseria gonorrhoeae: Can penetrate intact corneal epithelium. Secondary to conjunctivitis, it can rapidly lead to corneal perforation 1). Fluoroquinolone resistance is increasing.
Corynebacterium: A normal inhabitant of the ocular surface, but can become pathogenic with contact lens use or immunosuppression 1). Attention is needed for fluoroquinolone-resistant strains. Rare cases of severe corneal perforation caused by C. bovis have been reported 4).
Nontuberculous mycobacteria and Nocardia: Occur after trauma, contact lens use, or anterior segment surgery such as LASIK. Present as faint, poorly demarcated infiltrates 1).
QHow do corneal findings differ between Gram-positive cocci and Gram-negative rods?
A
Gram-positive cocci (staphylococci, pneumococci) present as small round to oval, well-marginated localized abscesses. In contrast, Gram-negative rods (Pseudomonas, Moraxella, Serratia) are associated with ground-glass opacity and marked edema of the surrounding stroma, and in severe cases, ring-shaped abscess due to corneal stromal melting. The Infectious Keratitis Clinical Practice Guideline, 2nd edition, includes a keratitis diagnostic flowchart that suggests inferring Gram-positive cocci from localized abscess and Gram-negative rods from ring-shaped abscess 1).
The normal cornea is protected from infection by the stratified squamous epithelium and defensive substances in tears (lysozyme, lactoferrin, IgA). Therefore, bacterial keratitis occurs when these defense mechanisms are compromised by trauma, contact lens use, surgery, ocular surface disease, or systemic disease 1). The AAO PPP identifies contact lens use as the greatest risk factor in the United States, while trauma is the main cause in many parts of the world 7).
Contact lens-related
Overnight wear: Significantly increases the risk of infection compared to daily wear. Nighttime wear, including orthokeratology, is a particularly important risk factor 7).
Inappropriate care: Refilling cleaning solution, contaminating the case, and storing or rinsing with tap water are typical triggers1)7).
Lens type: Two-week frequent replacement soft contact lenses (FRSCL) and conventional soft contact lenses (SCL) are associated with a higher incidence of gram-negative bacterial infections such as Pseudomonas aeruginosa, Moraxella, and Serratia1).
Decorative contact lenses: Lenses purchased online or in stores without a doctor’s prescription carry a high risk of infection7).
Trauma and Surgery-Related
Trauma: Penetrating eye injuries, foreign bodies, chemical burns, and thermal burns can be triggers. In non-contact lens-related trauma, gram-positive bacteria are more common1).
Refractive surgery: Bacterial keratitis can occur after LASIK and SMILE. In SMILE cases, onset occurs 1–3 days postoperatively, and a technique of converting the cap to a flap for treatment has been reported5).
Other surgeries: It can also occur after cataract surgery, corneal transplantation, and glaucoma surgery. Loose sutures can become a nidus for infection1).
Ocular Surface and Systemic Factors
Ocular surface diseases: Dry eye, herpes keratitis, bullous keratopathy, Stevens-Johnson syndrome, and neurotrophic keratopathy are predisposing factors1). There have been cases where extensively drug-resistant Pseudomonas aeruginosa was detected in contaminated artificial tears2).
Systemic factors: Diabetes, immunosuppression, atopic dermatitis, and collagen diseases are listed1)7).
Medication-related: Long-term use of steroid eye drops, contaminated eye drops, and NSAID eye drops are risk factors. Under long-term use of fluoroquinolone antibiotics, the detection rate of MRSA increases1).
In non-contact lens-related cases, MRSA after corneal transplantation, ocular surface diseases, and long-term use of fluoroquinolone antibiotics are important issues1). In patients on long-term steroids or immunosuppressants, differentiation from fungal infections (especially yeast-like fungi) and herpes virus is necessary1). In elderly, bedridden patients with refractory keratitis, the possibility of Pseudomonas aeruginosa, MRSA, and fungi should be considered1).
QWhat is the most important thing for contact lens wearers to do to prevent bacterial keratitis?
A
Avoiding overnight wear and proper lens care are most important. The AAO’s Bacterial Keratitis PPP also lists overnight wear, including orthokeratology, as a major risk factor7). Replacing the lens case every 3 months, daily cleaning and drying, and avoiding contact with tap water are essential7). Decorative lenses and lenses purchased online are also prone to infection, so a doctor’s prescription and regular follow-up are recommended.
Diagnosis is made by combining history, clinical findings, and tests1). The Infectious Keratitis Clinical Practice Guidelines (3rd edition) Clinical Question 1 (CQ-1) strongly recommends smear microscopy and culture for the diagnosis of bacterial keratitis (evidence level C)1).
Record the location, size, and depth of corneal infiltration, and evaluate epithelial defects with fluorescein staining. Assess anterior chamber inflammation (cells, flare, fibrin, hypopyon), corneal endothelial deposits, corneal sensation, lagophthalmos, and lacrimal drainage system 1). If the posterior pole is difficult to observe, add ultrasound B-mode examination.
Anterior segment optical coherence tomography (AS-OCT) objectively visualizes the depth of corneal lesions, increased corneal thickness, thinning, anterior chamber inflammatory cells, fibrin, keratic precipitates (KP), and endothelial plaque 1). It can evaluate treatment effects by comparing before and after treatment. However, it is not covered by insurance for infectious keratitis 1).
In vivo confocal microscopy (IVCM) non-invasively observes corneal cells, nerve fibers, fungi, and Acanthamoeba trophozoites and cysts 1).
For definitive diagnosis, perform smear microscopy and culture testing by scraping the corneal lesion 1). It is extremely important to collect specimens before administering antimicrobial agents; according to CQ-1 of the Infectious Keratitis GL 3rd edition, the culture positivity rate is 77.3% in cases not treated with antimicrobials before testing, and 37.8% after treatment 1).
Under topical anesthesia, scrape the ulcer including the margin with a sterile spatula. If there is a risk of perforation, use a sterile cotton swab, and fix with flame or alcohol 1). In a study of specimen collection methods, the culture positivity rate was 50% with swab scraping and 35% with a 23G needle; swab scraping is simple and recommended 1). Direct inoculation onto solid media has a positivity rate of 61%, while indirect inoculation via transport medium is 44%; direct inoculation onto solid media is preferable when possible 1).
According to the Infectious Keratitis GL 3rd edition, culture positivity rates are 37.6–74.3%, smear microscopy positivity rates are 58.1–73.7%, and the detection rate of causative bacteria by smear microscopy is 60–75% 1). The culture positivity rate in smear-positive cases is high at 57.1–82.4%, and combined use of both methods is desirable 1).
The main staining methods are shown below.
Staining Method
Target
Time Required
Gram stain (Faber G)
Bacteria, fungi, amoebae
3 minutes
Giemsa stain (Diff-Quik)
Bacteria, fungi, Chlamydia
15 seconds
Fungiflora Y
Fungi and amoeba cysts
Fluorescence microscope
Gram staining is performed when bacterial, fungal, or Acanthamoeba infection is suspected 1). Diff-Quik, a rapid staining kit, provides images equivalent to Giemsa staining in a short time 1). Fungiflora Y staining specifically stains chitin and cellulose, which are β-structure polysaccharides, and sensitively detects fungi and amoeba cysts 1).
For culture, blood agar, chocolate agar, Sabouraud agar, liquid media (thioglycollate broth), and transport media (Seed Swab®, Transwab®) are used 1). Blood agar allows assessment of hemolysis, and chocolate agar contains factors V and X, making it suitable for growth of Haemophilus species and gonococci 1). Culture results require 48 hours, and susceptibility results take 3–4 days 1).
Note that since the ocular surface harbors normal flora, bacteria isolated in culture are not necessarily the causative pathogen; comprehensive judgment is made based on consistency with smear results, ocular findings, drug susceptibility, and treatment response 1). McLeod et al. reported that while many community-acquired infections resolve with empirical treatment alone, smear and culture are strongly recommended for large central lesions, stromal melting, hypopyon, history of corneal surgery, and atypical cases 10). The AAO PPP explicitly recommends smear and culture in the following situations 7):
Central corneal infiltrate within 3 mm of the center and ≥2 mm in size
Two or more adjacent lesions
Large lesion with stromal melting
Anterior chamber inflammatory cells ≥1+
Post-corneal surgery
Atypical findings suspicious for fungi, amoeba, or nontuberculous mycobacteria
PCR is a rapid test that amplifies microbial DNA, but the Japanese Infectious Keratitis GL 3rd edition does not recommend diagnosing bacterial keratitis by PCR alone from corneal scrapings1). PCR may detect normal ocular surface flora and is positioned as an adjunct to smear microscopy and culture 1).
It is important to differentiate from catarrhal corneal infiltrate (type III allergy to staphylococcal exotoxin), fungal keratitis (feathery infiltrates, satellite lesions, endothelial plaque), Acanthamoeba keratitis (radial keratoneuritis, ring infiltrate, pseudodendritic lesions), and herpetic keratitis (dendritic lesion with terminal bulbs) 1). Corneal biopsy is considered when culture is negative but infection is strongly suspected 7).
QWhat should be done if no organism is detected on corneal scraping culture?
A
First, if the patient is on antibiotics, consider temporarily discontinuing them and repeating culture. The Infectious Keratitis GL 3rd edition reports that the culture positivity rate before antibiotic administration is 77.3%, which drops to 37.8% after administration 1). If still negative, consider corneal biopsy and reassess for special pathogens such as nontuberculous mycobacteria, Nocardia, Acanthamoeba, and fungi 1). Concurrently, continue empirical treatment with broad-spectrum antibiotics and evaluate treatment response every 48 hours 7).
The Infectious Keratitis Clinical Practice Guidelines (3rd edition) state that treatment of bacterial keratitis requires selection of antimicrobial agents effective against the causative bacteria, and prompt and reliable identification of the causative organism 1). The treatment flowchart (Figure 10) in the guidelines shows the following policy 1).
Estimate the causative organism from patient background, predisposing factors, and corneal findings.
Smear microscopy is useful for rapid diagnosis. Perform culture tests as well.
Use one agent for mild cases and two agents with different mechanisms of action for severe cases.
For extremely severe cases with intense anterior chamber inflammation, combine intravenous antimicrobial therapy.
Examples of initial treatment drugs from the Infectious Keratitis GL 3rd edition are as follows 1).
Suspected causative organism
First choice (two-drug combination)
Gram-negative bacilli
Fluoroquinolone + Aminoglycoside
Gram-positive cocci
Fluoroquinolone + Cephem
If the causative organism cannot be estimated, combine a new quinolone and a beta-lactam agent 1). Once the causative organism is identified, reassess treatment based on smear results, culture results, and drug sensitivity 1).
Commercially available antibacterial eye drops in Japan include fluoroquinolones (third-generation: ofloxacin [OFLX], levofloxacin [LVFX], tosufloxacin [TFLX]; fourth-generation: gatifloxacin [GFLX], moxifloxacin [MFLX]), cephems (cefmenoxime hydrochloride), aminoglycosides (tobramycin, gentamicin, dibekacin, framycetin), macrolides (erythromycin), and chloramphenicol. The glycopeptide vancomycin is used as an extemporaneous eye drop.
Third- and fourth-generation fluoroquinolones have improved tissue penetration and stronger efficacy against streptococci. High-concentration levofloxacin hydrate eye drops have improved therapeutic effect against gram-negative bacteria 1). Meanwhile, cefmenoxime hydrochloride eye drops are effective against streptococci but have poor activity against Pseudomonas aeruginosa, and aminoglycosides are effective against Pseudomonas aeruginosa but ineffective against streptococci 1). Note that fourth-generation fluoroquinolones have weaker activity against Pseudomonas aeruginosa.
The general correspondence between major causative bacterial groups and drug class sensitivity is shown below.
Instill 1 to 2 drops per dose, considering the severity and the post-antibiotic effect (PAE) of the drug 1). In severe cases or when reflex tearing is significant, frequent instillation every 30 minutes to 1 hour may be performed 1). PAE is observed with aminoglycosides and fluoroquinolones, but is short for cefmenoxime and chloramphenicol, requiring more frequent dosing 1).
The American Academy of Ophthalmology (AAO) Bacterial Keratitis PPP (2023) recommends the use of fortified antibiotics for vision-threatening cases with large central lesions or hypopyon7). Specific preparation methods are as follows 7).
Cefazolin 50 mg/mL: Add 9.2 mL of artificial tears to a 1 g vial, then dilute 5 mL of this solution with 5 mL of artificial tears.
Tobramycin 14 mg/mL: Add 2 mL of 40 mg/mL injectable tobramycin to 5 mL of tobramycin eye drops.
Vancomycin 25 mg/mL: Add 20 mL of 0.9% NaCl to a 500 mg vial.
In severe cases, cefazolin 50 mg/mL plus tobramycin 14 mg/mL is used; if MRSA is suspected, vancomycin 25–50 mg/mL is added 7). Fortified antibiotics are used as extemporaneous preparations, and the Japanese Infectious Keratitis Guideline 3rd edition warns against their indiscriminate use due to safety and stability concerns 1).
Extemporaneous Preparations and Resistant Bacteria
If commercial eye drops are not effective, consider diluting injectable drugs with saline to prepare extemporaneous eye drops 1). For MRSA and MR-CNS, the usefulness of chloramphenicol eye drops and extemporaneous arbekacin eye drops (off-label) has been reported 1). For extensively drug-resistant (XDR) Pseudomonas aeruginosa, systemic administration of novel antibiotics such as cefiderocol has been reported 2).
In recent years, decreased susceptibility to fluoroquinolones, which are widely used in ophthalmology, has become a problem, and the detection of multidrug-resistant bacteria such as MRSA, MRSE, and penicillin-resistant Streptococcus pneumoniae is increasing 1). Since the drug concentration in eye drops is high, even if susceptibility testing indicates resistance, it may be acceptable to continue treatment if clinical efficacy is observed 1).
The Infectious Keratitis Clinical Practice Guideline (3rd edition) CQ-5 concludes: “Weakly recommend against the concomitant use of corticosteroid eye drops in the treatment of bacterial keratitis.”1) This is based on the rationale that many cases lack identification of the causative organism, and given the increase in resistant bacteria, cautious use of steroids is warranted 1).
The main Steroids for Corneal Ulcer Trial (SCUT) found no significant difference in visual outcomes with prednisolone phosphate 1% plus broad-spectrum antibiotics, but subgroup analysis suggested visual improvement with early steroid use in Pseudomonas and severe cases 9). Based on these results, the AAO Bacterial Keratitis PPP 2023 states that “steroids may be considered after identification of the causative organism and confirmation of response to antibiotics (usually after 48 hours)” 7). However, steroids are contraindicated in Acanthamoeba, Nocardia, and fungal infections 7).
When deciding treatment, refer to the recommendations of the Infectious Keratitis Clinical Practice Guideline 3rd edition, and for severe cases, make decisions based on individual patient conditions.
Cycloplegics: In cases with significant anterior chamber inflammation, use atropine sulfate hydrate eye drops or mydriatics for pupil management and to prevent posterior synechiae 1).
Intraocular pressure-lowering agents: Used when secondary glaucoma is present.
Systemic administration: In severe cases with suspected spread to the sclera or intraocular structures, intravenous antibiotics may be added 1). Systemic administration is adjunctive in bacterial keratitis; indiscriminate use of broad-spectrum agents should be avoided 1).
The AAO PPP recommends reassessing the treatment regimen if no improvement is observed within 48 hours of starting treatment 7). The Infectious Keratitis GL 3rd edition also requires reviewing the patient’s background and treatment course if no improvement is seen, and checking for the possibility of mixed infection (bacteria + fungi, rarely bacteria + herpes) and the patient’s adherence to eye drops 1).
Surgical intervention is performed in cases unresponsive to drug therapy or with corneal perforation. The Infectious Keratitis GL 3rd edition states that therapeutic corneal transplantation should be performed when unavoidable, such as when anterior chamber loss persists, but elective corneal transplantation after infection control is preferable if possible 1). Full-thickness penetrating keratoplasty (PKP) or deep anterior lamellar keratoplasty (DALK) is selected, and good visual recovery after DALK for severe Pseudomonas aeruginosa keratitis has been reported 6). For small perforations (<2 mm), cyanoacrylate corneal adhesive and therapeutic contact lenses are used. For severe infection after SMILE, a technique of converting the cap to a flap, removing necrotic tissue, and irrigating with antibiotics has been reported 5). In a case of perforation due to C. bovis, a Gundersen conjunctival flap surgery was performed 4).
QWhen can steroid eye drops be started?
A
The Infectious Keratitis Clinical Practice Guidelines (3rd edition) CQ-5 clearly states: “We weakly recommend against the concomitant use of corticosteroid eye drops in the treatment of bacterial keratitis” 1). This is a safety-focused recommendation considering that the causative organism is often not identified and the increase in resistant bacteria 1). Subgroup analyses of the SCUT trial and the AAO PPP suggest cautious concomitant use only after identification of the causative organism and confirmation of response to antibiotics (usually after 48 hours), but it is contraindicated in Acanthamoeba, Nocardia, and fungal infections 7).
The normal cornea has a barrier composed of stratified squamous epithelium and Bowman’s membrane, and defense substances in tears such as lysozyme, lactoferrin, and IgA prevent microbial invasion 1). When this defense mechanism is disrupted by trauma, contact lens wear, steroid eye drops, or ocular surface diseases, bacteria can invade the corneal stroma.
When bacteria proliferate in the cornea, inflammatory cells, mainly neutrophils, infiltrate and form purulent lesions (infiltrates, abscesses, ulcers) 1). Proteolytic enzymes and reactive oxygen species released by infiltrating neutrophils cause progressive destruction of the corneal stroma, leaving tissue thinning after healing 1). If infection becomes prolonged or severe, a marked decrease in corneal endothelial cell count may lead to bullous keratopathy1).
Pseudomonas aeruginosa: Produces large amounts of proteases such as elastase, causing rapid corneal stromal melting and perforation 1). Protease activity is also considered the cause of the characteristic ground-glass opacity in the surrounding corneal stroma.
Streptococcus pneumoniae: Has a capsule that resists neutrophil phagocytosis, tends to spread deep into the stroma, and has a high risk of corneal perforation 1).
Staphylococcus aureus: Produces multiple exotoxins such as alpha-toxin, and may be associated with localized peripheral abscesses and adjacent type III allergic reactions (catarrhal corneal infiltrates) 1).
Moraxella lacunata: A large Gram-negative diplobacillus that causes severe keratitis in contact lens wearers and diabetic patients 1). It presents a variety of findings from small round lesions to ring infiltrates and irregularly shaped infiltrates 1).
Serratia: Due to differences in protease production, it can form from mild shallow ulcers to extensive abscesses 1). An association with contact lens wear has been noted 1).
Corynebacterium: A normal flora of the ocular surface, but can become pathogenic with contact lens use or immunosuppression 1). Fluoroquinolone-resistant strains exist and require caution in treatment 1).
Neisseria gonorrhoeae: Gram-negative diplococcus, known as the causative agent of gonococcal conjunctivitis characterized by creamy discharge 1). It can penetrate intact corneal epithelium and rapidly lead to corneal perforation following conjunctivitis1).
In recent years, decreased susceptibility to fluoroquinolones in ophthalmology has become a concern, with an increase in multidrug-resistant organisms such as MRSA, MRSE, and penicillin-resistant Streptococcus pneumoniae 1). From 2005 to 2015, fluoroquinolone resistance in MRSA and Pseudomonas aeruginosa has been reported to progress 7). Contributing factors include excessive antibiotic use, contaminated contact lens case environments, and horizontal gene transfer. Austin et al.’s review also emphasizes the importance of empirical treatment based on local epidemiological data and rapid susceptibility testing for resistant organisms 13).
Pseudomonas aeruginosa adheres to cell surface glycolipids such as asialoganglioside on corneal epithelial cells and injects effector molecules into host cells via the type III secretion system. This induces apoptosis of corneal epithelial cells and neutrophil recruitment. Subsequently, proteases released by the bacteria, including elastase, alkaline protease, and protease IV, degrade collagen and proteoglycans in the corneal stroma, causing rapid tissue destruction 1)11). Meanwhile, host-derived matrix metalloproteinases (MMP-2, MMP-9) from neutrophils also contribute to corneal damage and are the main cause of scar formation even after infection control. This cascade of infection establishment and tissue destruction highlights the therapeutic challenge of not only eliminating the pathogen with antibiotics but also controlling excessive host inflammation 11).
The AAO PPP classifies the stages of bacterial keratitis into four phases: progressive infiltration, active ulceration, regression, and healing 7). Even with appropriate treatment, visual impairment may persist due to corneal scarring or irregular astigmatism, and early diagnosis and prompt antibiotic administration are the most critical factors affecting prognosis 1). In untreated or severe cases, corneal perforation can occur within 24 hours, leading to endophthalmitis and loss of the eye 7).
Morelli MK et al. reported a case of corneal ulcer caused by extensively drug-resistant (XDR) Pseudomonas aeruginosa isolated from a commercial artificial tear product (EzriCare), successfully treated with systemic cefiderocol (a siderophore cephalosporin) combined with topical imipenem and polymyxin B. Whole-genome analysis identified blaVIM-80 and blaGES-9 2).
Kikuchi et al. reported a case of Pseudomonas aeruginosa keratitis in a 63-year-old man who had used orthokeratology and soft contact lenses for 10 years. He presented with diffuse corneal infiltration and ring ulcer, treated with levofloxacin, cefmenoxime, and gentamicin eye drops plus intravenous imipenem, resulting in healing but residual corneal opacity 3).
Elsheikh M et al. reported a case of severe corneal infection leading to perforation caused by Corynebacterium bovis in an 89-year-old woman with a history of herpes zoster keratitis. Contact with cattle in the vicinity was suspected as the route of infection. She was managed with vancomycin and ciprofloxacin combination and Gundersen conjunctival flap surgery 4).
Li J et al. reported 5 cases (7 eyes) of bacterial keratitis after SMILE. Onset occurred 1–3 days postoperatively, with Staphylococcus epidermidis and Streptococcus pneumoniae cultured. In severe cases, the cap was converted to a flap for necrotic tissue removal and antibiotic irrigation. All eyes achieved final corrected visual acuity of 20/32 or better 5).
Arun K and Georgoudis reported a case of a 32-year-old male contact lens wearer with Pseudomonas aeruginosa keratitis who underwent DALK after acute-phase antibiotic treatment and achieved good visual recovery 6).
Photoactivated Chromophore for Keratitis-Corneal Cross-linking (PACK-CXL)
As a response to the problem of antibiotic resistance, photoactivated chromophore for keratitis-corneal cross-linking (PACK-CXL) is attracting attention. In 2008, the Dresden protocol for keratoconus treatment (0.1% riboflavin eye drops for 30 minutes + UVA 3 mW/cm² irradiation for 30 minutes, total energy 5.4 J/cm²) was applied to the treatment of infectious keratitis 8). The name PACK-CXL was officially adopted at an international conference in 2013 8).
A scoping review by Kowalska et al. analyzed 233 preclinical studies and summarized that PACK-CXL increases the resistance of the corneal stroma to enzymatic degradation and kills pathogens including bacteria, fungi, and amoebae 8). Good results have been reported for bacterial corneal ulcers up to moderate severity, but the Dresden protocol is considered insufficiently effective, and a shift toward accelerated, high-fluence protocols is observed 8). This is an FDA-unapproved indication and is still at the research stage in Japan 7).
The increase in drug-resistant bacteria is a global challenge, and new treatment strategies for MRSA keratitis and fluoroquinolone-resistant bacteria are needed 7). In the future, establishment of a standard protocol for PACK-CXL, novel preparation methods for existing antibiotics, and development of species-specific rapid diagnostics are expected.
QHow do you manage bacterial keratitis caused by drug-resistant bacteria?
A
For MRSA, vancomycin eye drops (25–50 mg/mL) or in-house arbekacin eye drops are options 1)7). For fluoroquinolone-resistant strains, consider switching to aminoglycosides or cephems, or chloramphenicol eye drops 1). Systemic administration of novel antibiotics such as cefiderocol has been reported for extensively drug-resistant (XDR) Pseudomonas aeruginosa 2). In all cases, selection of therapeutic agents based on susceptibility testing is essential, and the importance of smear and culture tests is re-emphasized 1). PACK-CXL is being studied as an alternative for resistant bacteria but is not standard treatment 8).
Morelli MK, Kloosterboer A, Fulton SA, et al. Investigating and Treating a Corneal Ulcer Due to Extensively Drug-Resistant Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2023;67(7):e0045023.
Kikuchi Y, Toshida H, Ono J. A Case of Bacterial Keratitis in a Patient Using Orthokeratology and Soft Contact Lenses. Cureus. 2024;16(9):e68717. doi:10.7759/cureus.68717.
Elsheikh M, Elsayed A, Bennett N, Connor M. Corynebacterium Bovis: A Rare Case of Persistent Bacterial Keratitis and Corneal Perforation. Cureus. 2021;13(8):e16913. doi:10.7759/cureus.16913. PMID:34513486; PMCID:PMC8412843.
Li J, Ren SW, Dai LJ, Zhang B, Gu YW, Pang CJ, et al. Bacterial Keratitis Following Small Incision Lenticule Extraction. Infection and drug resistance. 2022;15:4585-4593. doi:10.2147/IDR.S367328. PMID:35999830; PMCID:PMC9393015.
American Academy of Ophthalmology Cornea/External Disease Preferred Practice Pattern Panel. Bacterial Keratitis Preferred Practice Pattern®. San Francisco: American Academy of Ophthalmology; 2023.
Kowalska ME, Pot SA, Hartnack S. Photoactivated Chromophore for Keratitis-Corneal Cross-linking (PACK-CXL)-A Scoping Review Based on Preclinical Studies. Translational vision science & technology. 2024;13(7):14. doi:10.1167/tvst.13.7.14. PMID:39023444; PMCID:PMC11262473.
Srinivasan M, Mascarenhas J, Rajaraman R, Ravindran M, Lalitha P, Glidden DV, et al. Corticosteroids for bacterial keratitis: the Steroids for Corneal Ulcers Trial (SCUT). Archives of ophthalmology (Chicago, Ill. : 1960). 2012;130(2):143-50. doi:10.1001/archophthalmol.2011.315. PMID:21987582; PMCID:PMC3830549.
McLeod SD, Kolahdouz-Isfahani A, Rostamian K, Flowers CW, Lee PP, McDonnell PJ. The role of smears, cultures, and antibiotic sensitivity testing in the management of suspected infectious keratitis. Ophthalmology. 1996;103(1):23-8. doi:10.1016/s0161-6420(96)30738-0. PMID:8628555.
Ung L, Bispo PJM, Shanbhag SS, Gilmore MS, Chodosh J. The persistent dilemma of microbial keratitis: Global burden, diagnosis, and antimicrobial resistance. Survey of ophthalmology. 2019;64(3):255-271. doi:10.1016/j.survophthal.2018.12.003. PMID:30590103; PMCID:PMC7021355.
Austin A, Lietman T, Rose-Nussbaumer J. Update on the Management of Infectious Keratitis. Ophthalmology. 2017;124(11):1678-1689. doi:10.1016/j.ophtha.2017.05.012. PMID:28942073; PMCID:PMC5710829.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.