Spherical OK Lens
Indications: Spherical myopia with corneal astigmatism less than 1.5 D
Characteristics: Standard 4-zone design. Easy to prescribe.
Prescription range: Up to approximately −4 D

Orthokeratology (OK) is a treatment that uses specially designed hard contact lenses worn on a planned schedule to reshape the cornea and correct refractive errors. With advances in lens materials, overnight wear (wearing lenses at bedtime and removing them upon waking) has become standard. A major feature is that patients can go without glasses or contact lenses during the day.
Originally developed for myopia correction, prescriptions for myopia control in schoolchildren have increased rapidly in recent years. Myopia prevalence is particularly high in Asian children, creating a strong demand for myopia control.
OK lenses consist of four concentric curves from the center to the periphery:
Wearing this lens causes thinning of the central corneal epithelium (about 5–10 μm) and thickening of the mid-peripheral cornea, resulting in reduced myopia and improved uncorrected visual acuity. The effect is noticeable the morning after the first wear and stabilizes with continued use.
In addition to central corneal flattening, mid-peripheral corneal thickening induces myopic defocus on the peripheral retina, suppressing axial elongation. This mechanism is shared with multifocal contact lenses and DIMS spectacles, based on the “peripheral retinal myopic defocus hypothesis.”
The base curve of the OK lens flattens the central cornea, reducing the excessive refractive power that causes myopia. Simultaneously, tears accumulate in the reverse curve area, and corneal epithelial cells redistribute from the center to the periphery, causing a shape change. This corneal deformation is reversible after discontinuation of lens wear, so it is not a permanent change independent of the lens.
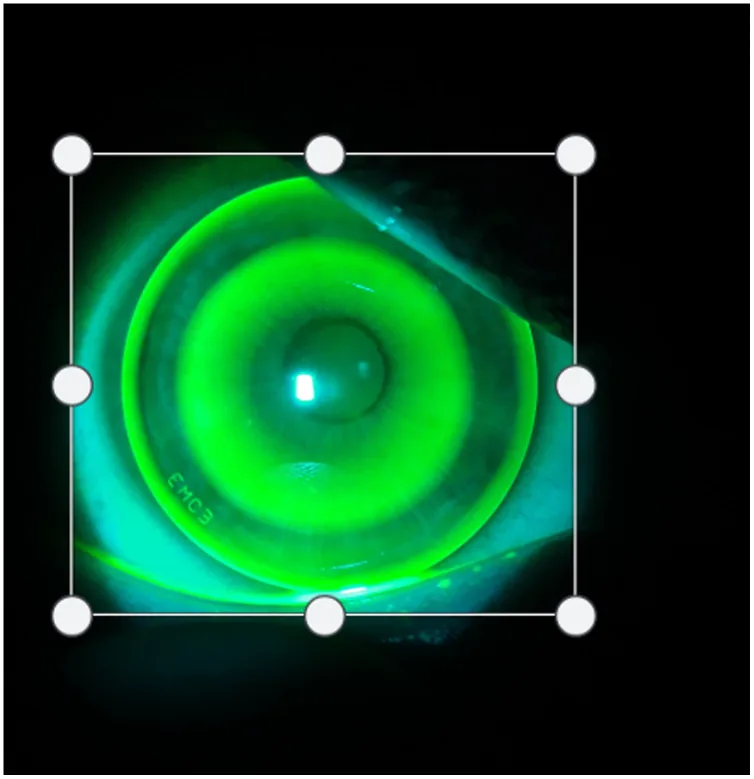
Fluorescein staining reveals a concentric pattern called a bull’s eye.
In an ideal bull’s eye pattern, the central dark zone is uniformly circular, adequately covers the pupillary area, and confirms good centration.
A good treatment response yields the following findings:
Improper fitting results in the following findings:
The main risk factors for myopia and its progression that are indications for orthokeratology are shown below.
Because OK lenses are worn overnight continuously, the risk of infectious keratitis is higher compared to regular rigid contact lenses. A survey by Watt and Swarbrick (2007) reported an increased incidence of microbial keratitis11), and the LOOK study by Rah et al. (2002) emphasized the importance of safety monitoring12). The risk increases particularly in the following situations.
According to the OK Guidelines (2nd edition), the following examinations are performed to confirm suitability.
| Examination Item | Purpose | Main Points to Check |
|---|---|---|
| Refraction and Visual Acuity Test | Confirm range of suitability | Spherical equivalent, corrected visual acuity |
| Corneal Topography | Calculate prescription parameters, rule out contraindications | Flat K value, corneal eccentricity (E value), rule out keratoconus |
| Corneal Thickness Measurement (Pachymetry) | Confirm contraindications | Rule out corneal thinning and dystrophy |
| Axial length measurement | Baseline setting | For myopia progression monitoring |
| Slit-lamp examination | Exclusion of anterior segment diseases | Check for active inflammation and corneal epithelial disorders |
| Tear film test | Assessment of contact lens suitability | Presence of dry eye |
Based on the results of refraction/visual acuity tests and corneal topography analysis, two factors are selected: the flat K (flat meridian) value and the target power (desired correction). Using the attached conversion table, the recommended base curve is determined from the intersection of the flat K value and the target power.
Indications (from OK Guidelines 2nd edition):
Contraindications:
The basic follow-up schedule after starting lens wear is as follows.
| Follow-up Timing | Main Items to Check |
|---|---|
| Next morning after wear (or within 1 week) | Correction effect, corneal epithelial status, fluorescein pattern |
| 1 month later | Confirm stability of visual acuity and refraction, check compliance |
| 3 months later | Axial length measurement (comparison with baseline), complication screening |
| Every 6 months thereafter | Axial length measurement, myopia progression monitoring, safety check |
At each follow-up, fluorescein pattern evaluation, corneal epithelial status check, visual acuity, refraction, and axial length measurement are performed. Regular axial length measurement is essential for monitoring the myopia control effect and serves as a criterion for continuing, intensifying, or changing treatment.
Corneal topography measures flat K value and corneal eccentricity to determine prescription parameters. It is important to rule out contraindicated conditions such as keratoconus. Axial length measurement must be recorded as a baseline for myopia progression monitoring. Corneal thickness, tear film, and slit-lamp examination are also mandatory pre-prescription tests.
The selected trial lens is placed on the patient and the fit is checked. Good centration and about 1 mm of movement with blinking are sufficient. The patient takes a nap or rests with eyes closed for 1–2 hours in the clinic, after which the effect is evaluated.
Key points for wear instruction:
Management of astigmatism: For corneal astigmatism of 1.5 D or more, toric OK lenses are recommended (Chen et al., TO-SEE study 2013)10). Because the alignment curve provides parallel fitting, centration and movement are improved.
Management of high myopia: Conventional OK lenses were limited to about −4 D, but with the development of double-zone designs and high-power lenses for high myopia, lenses that can handle cases of −6 D or more have become available. However, the effect is often more limited than in moderate myopia.
Spherical OK Lens
Indications: Spherical myopia with corneal astigmatism less than 1.5 D
Characteristics: Standard 4-zone design. Easy to prescribe.
Prescription range: Up to approximately −4 D
Toric OK Lens
Indications: Cases with corneal astigmatism of 1.5 D or more
Characteristics: Aspheric alignment curve design. Improved centration and stability.
Prescription range: Myopia with astigmatism
The OK Guidelines (2nd Edition)15), revised in December 2017, recommend the following measures against corneal infections:
| Complication | Frequency/Features | Management |
|---|---|---|
| Corneal epithelial damage (non-infectious) | Relatively common. Confirmed by fluorescein staining | Discontinue lens wear, artificial tears, fitting adjustment |
| Infectious keratitis (bacterial) | Increased risk with overnight wear | Immediate discontinuation, culture, antibiotic eye drops |
| Acanthamoeba keratitis | Severe. Mainly caused by tap water use | PHMB eye drops, chlorhexidine eye drops, long-term treatment required |
| Decentration | Irregular astigmatism, ghost images | Re-evaluate fitting, change base curve |
| Halos and glare | Especially at night | Consider switching to a lens with larger optical zone |
Multiple meta-analyses and RCTs have reported a 30–50% inhibition rate of axial elongation over 2 years1).
Key RCT evidence is shown below.
| Study | Subjects | Duration | Axial length suppression rate | Notes |
|---|---|---|---|---|
| LORIC (Cho 2005)13) | Hong Kong children | 2 years | Approximately 46% | Pilot study; first demonstration of OK myopia suppression |
| ROMIO (Cho 2012)3) | Hong Kong children aged 6–10 | 2 years | 43% | RCT design |
| MCOS (Santodomingo-Rubido 2012)9) | Spanish children | 2 years | Approximately 32% | Efficacy confirmed in Western children |
| TO-SEE (Chen 2013)10) | Myopia with astigmatism | 2 years | Significant suppression | Efficacy of toric OK lens confirmed |
| Lipson 20086) | Adults and children | Long-term | — | Long-term clinical outcomes reported |
| Walline 20047) | Pediatric RCT | 3 years | No difference in axial length | Confirmed limitations of RGP |
The effect persists during continued wear, and after discontinuation, the corneal shape returns to baseline within a few days to 2 weeks (reversible). However, the axial length elongation suppression effect obtained during the wearing period is partially maintained after discontinuation.
A 2-year combination RCT with low-concentration atropine 0.01% (Kinoshita 2020) showed significant suppression of axial elongation compared to orthokeratology alone2). This additive effect is thought to be based on complementary mechanisms: optical defocus correction (OK) and scleral remodeling suppression (atropine).
The value of “1 diopter” of myopia progression is significant; Bullimore and Brennan (2019) estimated that suppressing myopia by 1D can reduce the risk of myopic maculopathy by 40%4).
A meta-analysis by Haarman et al. (2020) showed that the risk of myopia complications (retinal detachment, glaucoma, macular degeneration, etc.) increases exponentially with increasing myopia5), highlighting the importance of delaying axial elongation even by one year.
In a 2-year RCT by Kinoshita 2020, the combination of orthokeratology + 0.01% atropine showed significant suppression of axial elongation compared to monotherapy2). Orthokeratology provides optical defocus correction, while atropine provides pharmacological suppression of scleral remodeling, and they are thought to brake myopia progression through complementary mechanisms. It is an effective option when monotherapy does not provide sufficient effect.
During OK lens wear, the tear film becomes thinner in the base curve area, and mechanical pressure is applied to the central corneal epithelium. Meanwhile, negative pressure occurs in the reverse curve area, causing tear accumulation. This pressure difference redistributes central corneal epithelial cells toward the periphery, thinning the central epithelium.
No significant changes occur in the corneal stroma; deformation is mainly limited to the corneal epithelium (reversible). After discontinuation, the shape almost returns to baseline within 3 to 14 days. Multiple studies have shown that even long-term wear returns to baseline corneal shape, indicating low concern for permanent corneal deformation3).
Thickening of the mid-peripheral cornea causes peripheral light rays to focus in front of the fovea (peripheral myopic defocus). This optical signal acts as a suppressive signal for axial elongation. It shares the same mechanism as multifocal contact lenses and DIMS spectacles, and is widely supported as the “peripheral retinal myopic defocus hypothesis” 3).
Acanthamoeba protozoa are widely present in tap water, pools, and rivers. Infected water adheres to the cornea via lenses or cases, and enters through minor epithelial abrasions. Overnight wear accumulates corneal microtrauma, increasing infection risk. Acanthamoeba phagocytizes corneal stromal keratocytes, causing severe stromal keratitis and ring infiltrates.
Treatment for Acanthamoeba keratitis involves long-term (usually 6 months or more) use of PHMB (polyhexamethylene biguanide) eye drops or chlorhexidine eye drops. If an accurate diagnosis is not made early, visual prognosis is poor. Therefore, if keratitis suspicious of Acanthamoeba occurs in an orthokeratology wearer, promptly refer to a specialist facility.
Watt and Swarbrick (2007) investigated the trend of orthokeratology-related microbial keratitis and reported that the risk is particularly high in Asian and younger populations 11). Since orthokeratology lenses are worn overnight, the infection risk is relatively higher than with regular contact lenses, and appropriate patient education is key to infection prevention.
In myopia management, orthokeratology is particularly suitable for the following patients:
In a long-term clinical outcome study by Lipson (2008), the long-term safety and efficacy of overnight corneal reshaping were confirmed in both adults and children 6), supporting long-term use under appropriate patient selection and management. Regarding the significance of axial length in myopia management, Bullimore and Brennan (2019) estimated that suppressing 1 D of myopia can reduce the risk of myopic maculopathy by 40% 4), indicating the importance of starting treatment one year earlier.
After discontinuation, the corneal shape returns to its pre-wear state within a few days to two weeks, so the myopia correction effect disappears. However, the effect of suppressing axial elongation (not shortening of axial length but suppression of elongation) obtained during the wearing period is irreversible and partially maintained even after discontinuation. If discontinued at an age when myopia progression continues, explain to the patient and parents that progression will continue along the normal course after discontinuation.
Multiple meta-analyses have confirmed the 2-year axial elongation suppression rate of orthokeratology 1), but long-term follow-up data of 5 years or more are limited. Further verification is also needed regarding the long-term stability of axial length after treatment discontinuation. In a randomized controlled trial by Walline et al. (2004), the rigid contact lens group showed less refractive progression, but there was no significant difference in axial length increase 7). Therefore, simple RGP wear is not justified for myopia progression control.
A Cochrane Database Syst Rev (Walline 2011) 14) systematic review evaluated the overall evidence for optical interventions to slow myopia progression, confirming the effectiveness of multiple interventions including OK.
Evidence for the combination of orthokeratology plus 0.01% atropine is accumulating 2), but standard protocols for optimal concentration (comparison of 0.01%, 0.025%, 0.05%) and optimal start/discontinuation timing have not yet been established. From a new perspective by Kang and Swarbrick (2016), optimization of prescription parameters to maximize OK peripheral defocus is also being studied 8).
After wearing OK lenses, corneal asphericity changes, and higher-order aberrations (especially coma and spherical aberrations) may increase. Research is ongoing on the trade-off between the optimal defocus profile for myopia progression control and visual quality 3).
Quantifying the risk of Acanthamoeba keratitis and bacterial keratitis and optimizing prevention protocols are challenges. A survey by Watt and Swarbrick (2007) reported that OK lens-related microbial keratitis tends to occur more frequently in young Asian individuals 11), and individualized guidance based on understanding risk factors is important.
As of April 2025, orthokeratology is not approved in Japan for the indication of myopia progression control. Proper use according to the OK guidelines of the Japan Contact Lens Society (2nd edition, 2017) 15) is required, and future approval trends are of interest.