Contact lens intolerance is a general term for a condition in which ocular surface disorders and subjective symptoms caused by or triggered by CL wear persist or recur chronically, making continued CL wear difficult. The severity ranges from mild asymptomatic cases to severe cases leading to corneal ulcers.
Contact lens wear is the greatest risk factor for infectious keratitis1), and it is estimated that approximately 71,000 cases of microbial keratitis occur annually in the United States1). Among all contact lens wearers, the annual incidence of contact lens-related corneal infiltrative events (CIE) is reported to be about 3 to 6 per 100 person-years5).
The main mechanisms by which contact lenses induce ocular disorders can be broadly classified into the following five categories.
Mechanism
Representative Condition
Main Cause
Mechanical disturbance
3 and 9 o’clock staining, SEAL
Friction during blinking with HCL, stiffness of SiHy
With the widespread use of silicone hydrogel (SiHy) lenses, hypoxia-related complications have decreased, but intolerance due to lipid deposits is increasing 6). Contact lens wear is one of the greatest risk factors for Acanthamoeba keratitis (AK), and it has been reported that over 88% of AK patients were contact lens wearers 3). Daily disposable (DD) lenses significantly reduce the risk of AK compared to DW reusable lenses (OR 0.26; approximately 3.84-fold difference), and switching to DD is estimated to prevent 30–62% of AK cases 3).
QAre daily disposable lenses less likely to cause intolerance?
A
Daily disposable lenses require no lens care, eliminating the risk of case contamination and minimizing protein deposit buildup. They are less likely to cause giant papillary conjunctivitis or care solution-related complications, and significantly reduce the risk of Acanthamoeba keratitis. However, dry eye-related epithelial damage and complications from overnight wear can still occur with daily disposable lenses, so proper wearing time management and regular check-ups remain important.
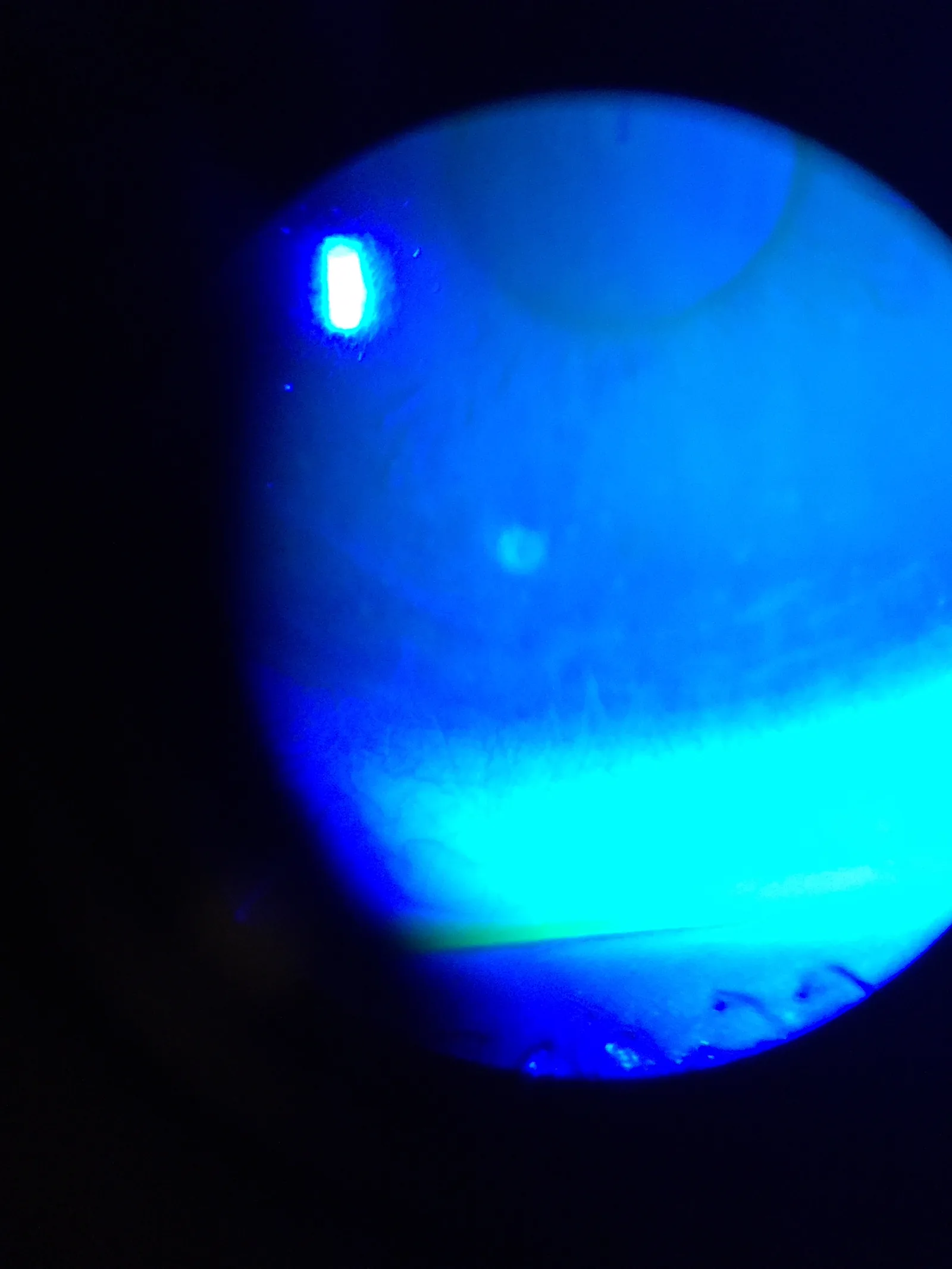
Iceclanl. Contact Lens Related Small Corneal Ulcer with Sodium Fluorescein Staining. Wikimedia Commons. 2015. Figure 1. Source ID: commons:File:Contact_Lens_Related_Small_Corneal_Ulcer_with_Sodium_Fluorescein_Staining_1.jpg. License: CC BY-SA 4.0.
Slit-lamp micrograph showing a small corneal ulcer associated with contact lens wear, stained with fluorescein sodium; the yellow-green fluorescent epithelial defect is clearly visible on the corneal surface. This corresponds to the visualization of corneal epithelial damage patterns by fluorescein staining discussed in the section “2. Main Symptoms and Clinical Findings.”
Mild to moderate. Severe pain suggests infectious cause
Blurred vision / visual loss
Light scattering due to epithelial damage
Reduced wearing time
Feeling the need to remove CL earlier than before
If hyperemia, discharge, and pain all occur together, infectious corneal ulcer is possible and requires special attention. All CLs reduce corneal sensation (hypoesthesia). Due to reduced sensation, CL wearers may not notice early symptoms of corneal damage 1).
Location: Limited to the 3 and 9 o’clock positions of the corneal limbus
Cause: During blinking, the HCL moves approximately 2 mm vertically, causing local dryness when tears are drawn in from the 3 and 9 o’clock directions. It also occurs with steep fitting.
Course: Mild cases heal in 3–5 days. If it progresses to erosion, it takes about 1 week and may leave corneal opacity.
Smile Mark Superficial Punctate Keratitis (SCL)
Location: Inferior pupillary area (corresponding to the shape of a smiling mouth)
Cause: Occurs in patients with pre-existing dry eye due to decreased tear fluid under the lens. A pattern specific to dry eye in SCL wearers.
Course: Managed with dry eye eye drops. Advise early removal after evening.
Diffuse Superficial Punctate Keratitis (HCL/SCL)
Location: Almost uniform across the entire cornea
Cause: Oxygen deficiency due to CL wear. Lens deposits add mechanical irritation and worsen the condition.
Course: Heals in 4–5 days with CL discontinuation and eye drop treatment.
The following are important as diffuse and linear lesions.
SEAL (Superior Epithelial Arcuate Lesion): When wearing rigid SiHy material SCL, an arcuate corneal epithelial lesion parallel to the limbus occurs in the superior peripheral cornea. It is caused by mechanical damage from the upper eyelid pressing on the relatively rigid SiHy lens.
Corneal infiltrates (CLPU / CLARE): Non-infectious immune-mediated infiltrates due to immune reaction to bacterial products 6). Single, small, peripheral lesions are characteristic of CLPU. Multiple lesions are characteristic of CLARE.
Infectious corneal ulcer: Characterized by the triad of hyperemia, discharge, and pain 1). Emergency management is required.
QWhat should be done if pain occurs while wearing contact lenses?
A
First, remove the contact lens immediately. If pain is mild and there is no vision loss, you may stop wearing the lens until the next day and observe the condition. However, if there is redness, discharge, or severe pain, it may be infectious keratitis, so promptly see an ophthalmologist. Do not discard the removed lens; bring it to your appointment for investigation of the cause.
The characteristics and precautions of major CL care solutions are shown below.
Type
Characteristics
Precautions
MPS/MPDS
Single solution for cleaning, disinfection, and storage
Weak disinfection effect against fungi and viruses
Hydrogen peroxide preparations
Higher disinfection efficacy than MPS
Risk of corneal and conjunctival damage if neutralization is inadequate
Povidone-iodine preparations
Highest disinfection efficacy
Cannot be used in patients with iodine allergy
No matter how high the disinfection efficacy, neglecting basic care such as rubbing, rinsing, and cleaning and drying the lens case can lead to serious eye disorders such as corneal ulcers 7).
Diagnosis of CL intolerance requires a detailed interview about CL type, lens care methods, and wearing time. Slit-lamp microscopy is essential for diagnosing corneal damage caused by CLs, and fluorescein staining is useful for determining the pattern of epithelial defects. For HCL-wearing eyes, it is important to observe lens surface deposits and wettability before fluorescein staining.
In differentiating infectious from non-infectious causes, the triad of hyperemia, discharge, and pain, as well as the presence of anterior chamber inflammation, are important. CLPU may occur without epithelial defect, so caution is needed in differentiating it from infectious keratitis 6).
The prognosis of CL intolerance varies depending on the cause and severity. In mild superficial punctate keratopathy (SPK), the epithelium recovers within 3–5 days after discontinuation of CL, and complete healing can be expected with additional eye drops. For SEALs or erosions with 3 and 9 o’clock staining, healing takes about 7–10 days and may leave opacity.
Severe infectious keratitis may require antibiotic treatment and hospitalization, and corneal scarring or irregular astigmatism may remain after healing. Acanthamoeba keratitis may take more than a year to treat, and some severe cases require corneal transplantation.
The prognosis of non-infectious corneal infiltrates (CLPU, CLARE) is generally good, and with appropriate management, they usually heal within 1–2 weeks9). However, if recurrence occurs repeatedly, the CL wearing regimen must be fundamentally reviewed. In cases with frequent recurrence, a comprehensive approach combining a change to DD lenses, modification of wearing schedule, enhanced dry eye treatment, and MGD management is required.
The prognosis of giant papillary conjunctivitis (GPC) is good with appropriate treatment and elimination of the cause (protein deposits, CL material), but recurrence is likely if the CL type is not changed. Improvement of GPC may take several weeks to months. In refractory cases with repeated GPC flares, complete transition to glasses or refractive surgery such as ICL, LASIK, or SMILE may be considered as long-term options.
The basic principle is discontinuation of CL wear and elimination of the cause. Based on corneal findings, the cause is inferred, and the healing period, presence of sequelae, and need for CL change are explained individually.
After healing, CL change is performed according to the cause. For 3 and 9 o’clock staining, a change to SCL is effective; for SEALs, selection of a safe SCL; for smile-mark superficial punctate keratopathy, a change to a silicone hydrogel lens with high water retention is effective.
Eye drop treatment:
For dry eye-related cases: 3% diquafosol sodium eye drops 6 times daily or 2% rebamipide eye drops UD 4 times daily
Epithelial repair support: 0.1% or 0.3% sodium hyaluronate eye drops 4–6 times daily
When inflammation is severe (after excluding infection): 0.1% fluorometholone eye drops 4 times daily
Treatment involves discontinuation of CL wear and use of antibiotics plus low-concentration steroids (0.1% fluorometholone) eye drops. Steroid use is desirable because infiltrative lesions may remain as opacity, but use when infection cannot be completely ruled out should be carefully judged. The Infectious Keratitis Clinical Practice Guidelines (3rd edition) weakly recommends against concomitant steroid use for bacterial keratitis8), and indiscriminate use before identification of the causative organism should be avoided.
Indications: Small non-central ulcer with infiltration ≤2 mm and ≥3 mm from the visual axis
Treatment: Empirical therapy with fluoroquinolone eye drops, e.g., 0.5% levofloxacin or 0.5% moxifloxacin, 4–6 times daily
Threat to vision
Indications: Infiltration >2 mm, <3 mm from visual axis, or worsening after 48 hours of treatment
Treatment: Perform corneal culture and Gram stain; start vancomycin (25–50 mg/mL) plus fortified tobramycin (14 mg/mL) eye drops every hour. Adjust medication based on culture results1)
Immediate discontinuation of CL is mandatory. For Acanthamoeba keratitis, combination therapy with polyhexamethylene biguanide (PHMB) and propamidine isethionate, among others, is used.
The basic approach is to discontinue CL wear or switch to daily disposable lenses. Use 0.1% fluorometholone 4 times daily for 1–2 weeks. Even after symptom improvement, returning to the original lens often leads to recurrence, so changing the lens type is desirable.
Precautions for Using Bandage Contact Lenses (BCL)
When using BCL for pain relief in microcystic and bullous corneal epitheliopathy, thin lenses with high water content and high Dk value are considered safe 2). Prophylactic broad-spectrum antibiotics are recommended to prevent secondary infection during use 2). BCL does not provide a long-term solution for corneal edema2).
QAre silicone hydrogel lenses safe?
A
Silicone hydrogel lenses have dramatically improved oxygen permeability compared to conventional HEMA lenses, significantly reducing hypoxia-related complications. However, due to the hydrophobic nature of the material, they are prone to lipid deposits, making proper selection of care solutions important. The stiffness of the material can cause SEALs, and incompatibility with some care solutions has been reported to cause ring-shaped staining. Regardless of the lens type, proper care and regular check-ups are essential.
Contact lenses limit the supply of atmospheric oxygen to the cornea. Lenses with low oxygen permeability (Dk/t) increase anaerobic metabolism in the corneal epithelium, leading to osmotic pressure rise due to lactate accumulation and subsequent epithelial edema. Until around 1990, conventional HEMA SCLs frequently caused acute epithelial edema due to oxygen deficiency, but now SiHy lenses are mainstream and hypoxic damage has decreased. Chronic hypoxia induces corneal neovascularization, and long-term wearers may have potential limbal stem cell deficiency.
Friction between the contact lens and the ocular surface during blinking causes epithelial damage. With HCL, the lens moves about 2 mm vertically with each blink, and when tear fluid is drawn in from the 3 and 9 o’clock positions, local drying and punctate keratopathy occur. With SCL, SEALs occur at the site where the upper eyelid presses the lens, especially when the corneal side surface of the lens is irregular.
SiHy lenses are hydrophobic, so their surfaces are modified with plasma treatment or other methods to improve hydrophilicity. Unlike conventional hydrogel lenses, they are more prone to lipid deposits, and the cleaning agents in MPS must be effective against lipid deposits. Accumulation of lipid deposits can trigger immune reactions, causing GPC and corneal infiltration 6).
Chronic mechanical stimulation and bacterial endotoxins from CL wear can trigger an immune response, leading to sterile infiltration 9). This is often caused by inadequately disinfected SCLs or biofilms in the lens case 10). Biofilm formation in the lens case is a significant risk factor for infectious keratitis, and bacteria within biofilms are highly resistant to disinfectants 10). In GPC, a type I allergic reaction to proteins deposited on the CL surface is involved.
AK is a severe protozoal keratitis specific to CL wearers. Acanthamoeba is widely present in tap water, pools, soil, etc., and invades the cornea of CL wearers. Microtrauma to the corneal epithelium caused by CLs serves as the portal of entry for AK. Pain is severe (especially worsening at night), and radial keratoneuritis along the corneal nerves is an early sign of AK. Treatment requires multidrug therapy including PHMB and propamidine isethionate, and some severe cases require long-term treatment (over 1 year).
Multifocal soft CLs are sometimes used to control myopia progression. Multiple RCTs with Level I evidence have shown significant suppression of myopia progression compared to single-vision lenses or spectacles, with SE changes reported as -0.22 to -0.81 D in the multifocal CL group and -0.50 to -1.45 D in the control group 4). No serious adverse events have been reported, but long-term effects, optimal treatment duration, and rebound effects after discontinuation are not yet established 4). In children with CL intolerance, the balance between managing CL intolerance and the myopia control effect must be carefully evaluated.
Public Health Strategies for Preventing Acanthamoeba Keratitis
Switching to DD lenses to reduce AK risk has significant public health implications. It is estimated that transitioning from DW reusable lenses to DD lenses could prevent 30-62% of AK cases 3), and a review of prescribing practices along with patient education is warranted.
The TFOS CLEAR (Contact Lens Evidence-Based Academic Reports) published in 2021 systematized the classification, epidemiology, risk factors, and prevention of CL complications 6), and has become an international standard reference for inflammatory complications including CL intolerance. The importance of risk stratification and individualized management based on lens material, wearing schedule, and care product combinations is emphasized 6).
Staphylococcus aureus easily colonizes the CL surface and lens case, and is one of the main causative bacteria of CLPU and CLARE. Jalbert et al. showed that S. aureus is isolated from the CL surface during CLPU, and bacterial components (peptidoglycan, lipoteichoic acid) trigger an immune response via Toll-like receptors on the corneal epithelium11). With continuous wear of SiHy lenses (30 days), the annual incidence of non-infectious corneal infiltrates reaches about 20 per 100 person-years; although hypoxia-related complications have decreased, the CIE risk remains high 12).
According to a recent review by Steele et al., the epidemiology of CL-related infiltrative events varies greatly depending on material, wearing schedule, and care 13). DD lenses significantly reduce CIE risk and are an important preventive strategy in CL intolerance management.
Relationship between Dry Eye Treatment and CL Intolerance
Stepwise dry eye treatment based on TFOS DEWS III corrects the underlying dry eye in CL-related ocular surface disorders including CLIDE, thereby improving the overall prognosis of CL intolerance 14). Artificial tears and tear secretion stimulants such as diquafosol and rebamipide may improve CLIDE symptoms and increase the rate of continued CL wear.
The number of CL wearers worldwide has reached approximately 300 million, and prevention of CL-related complications is an important public health issue 15). Through prevention and management of CL intolerance, it is the ophthalmologist’s key role to maintain the QOL and ocular health of CL wearers over the long term.
Regular Lens Case Replacement and Biofilm Prevention
Reports indicate that 30–80% of lens cases in use show bacterial contamination 10), making rubbing cleaning, regular case replacement, and drying essential. Regular cleaning with sodium hypochlorite preparations (e.g., Progent) about once every two weeks has been reported effective for biofilm removal and is recommended in orthokeratology guidelines.
American Academy of Ophthalmology. Bacterial Keratitis Preferred Practice Pattern. Ophthalmology. 2024;131(2):P265-P330.
American Academy of Ophthalmology. Corneal Edema and Opacification Preferred Practice Pattern. Ophthalmology. 2024.
Carnt N, Minassian DC, Dart JKG. Acanthamoeba Keratitis Risk Factors for Daily Wear Contact Lens Users: A Case-Control Study. Ophthalmology. 2023;130(1):48-55. doi:10.1016/j.ophtha.2022.08.002. PMID:35952937.
Cavuoto KM, Trivedi RH, Prakalapakorn SG, Oatts JT, Nallasamy S, Morrison DG, Pineles SL, Chang MY. Multifocal Soft Contact Lenses for the Treatment of Myopia Progression in Children: A Report by the American Academy of Ophthalmology. Ophthalmology. 2025;132(4):495-503. doi:10.1016/j.ophtha.2024.09.031. PMID:39503665; PMCID:PMC11930616.
Stapleton F, Keay L, Edwards K, Naduvilath T, Dart JK, Brian G, et al. The incidence of contact lens-related microbial keratitis in Australia. Ophthalmology. 2008;115(10):1655-62. doi:10.1016/j.ophtha.2008.04.002. PMID:18538404.
Stapleton F, Bakkar M, Carnt N, Chalmers R, Vijay AK, Marasini S, et al. CLEAR - Contact lens complications. Contact lens & anterior eye : the journal of the British Contact Lens Association. 2021;44(2):330-367. doi:10.1016/j.clae.2021.02.010. PMID:33775382.
Sweeney DF, Jalbert I, Covey M, Sankaridurg PR, Vajdic C, Holden BA, et al. Clinical characterization of corneal infiltrative events observed with soft contact lens wear. Cornea. 2003;22(5):435-42. doi:10.1097/00003226-200307000-00009. PMID:12827049.
Wu YT, Willcox M, Zhu H, Stapleton F. Contact lens hygiene compliance and lens case contamination: A review. Contact lens & anterior eye : the journal of the British Contact Lens Association. 2015;38(5):307-16. doi:10.1016/j.clae.2015.04.007. PMID:25980811.
Jalbert I, Willcox MD, Sweeney DF. Isolation of Staphylococcus aureus from a contact lens at the time of a contact lens-induced peripheral ulcer: case report. Cornea. 2000;19(1):116-20. doi:10.1097/00003226-200001000-00023. PMID:10632021.
Loretta Szczotka‐Flynn, Mireya Diaz. Risk of Corneal Inflammatory Events with Silicone Hydrogel and Low Dk Hydrogel Extended Contact Lens Wear: A Meta‐Analysis. OVS. 2007;84(4):247-256. doi:10.1097/opx.0b013e3180421c47.
Steele KR, Szczotka-Flynn L. Epidemiology of contact lens-induced infiltrates: an updated review. Clinical & experimental optometry. 2017;100(5):473-481. doi:10.1111/cxo.12598. PMID:28868803.
Jones L, Craig JP, Markoulli M, Karpecki P, Akpek EK, Basu S, et al. TFOS DEWS III: Management and Therapy. American journal of ophthalmology. 2025;279:289-386. doi:10.1016/j.ajo.2025.05.039. PMID:40467022.
Craig JP, Alves M, Wolffsohn JS, Downie LE, Efron N, Galor A, et al. TFOS Lifestyle Report Executive Summary: A Lifestyle Epidemic - Ocular Surface Disease. The ocular surface. 2023;30:240-253. doi:10.1016/j.jtos.2023.08.009. PMID:37659474.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.