“Smartphone presbyopia” is a common term for reduced accommodative function or accommodative spasm caused by prolonged near-distance use of digital devices such as smartphones. It is not a formal medical term but is classified as part of technostress eye syndrome, IT eye syndrome, and VDT syndrome.
Prolonged use of smartphones, computer displays, and video games under poor conditions can lead to various physical and mental symptoms centered on the visual system (eyes), known as VDT syndrome. With recent advances in IT, it has increased rapidly and is also called technostress eye syndrome or IT eye syndrome. Due to the global spread of smartphones and the advent of 3D televisions, it is increasing across a wide age range.
TFOS (Tear Film & Ocular Surface Society) defines digital eye strain (DES) as “the development or exacerbation of recurrent ocular symptoms and signs specifically related to viewing digital device screens” 1). This concept encompasses all digital devices including smartphones, tablets, computers, and VR headsets.
The global prevalence of DES is approximately 66% (95% CI: 59–74%) 8), and due to the surge in remote work and online learning during the COVID-19 pandemic, it has risen to 74% (95% CI: 66–81%) 7). Particularly in young people (10s–30s), decreased accommodative function is a problem, and smartphones are considered to have the highest CVS severity among devices 4).
QWhat is the difference between smartphone presbyopia and true presbyopia?
A
True presbyopia is caused by age-related hardening of the lens, resulting in irreversible loss of accommodative ability. In contrast, smartphone presbyopia is primarily due to excessive tension of the ciliary muscle (accommodative spasm) from prolonged near-distance device use, and is essentially a temporary functional decline. It differs from true presbyopia in that it can be reversed through environmental improvements, rest, and medication. However, if it becomes chronic and severe, accommodative ability may persistently decrease, potentially leading to a condition similar to true presbyopia.
Sheppard AL, Wolffsohn JS. Digital eye strain: prevalence, measurement and amelioration. BMJ Open Ophthalmol. 2018 Apr 16;3(1):e000146. Figure 1. PMCID: PMC6165611. DOI: 10.1155/2018/4107590. License: CC BY.
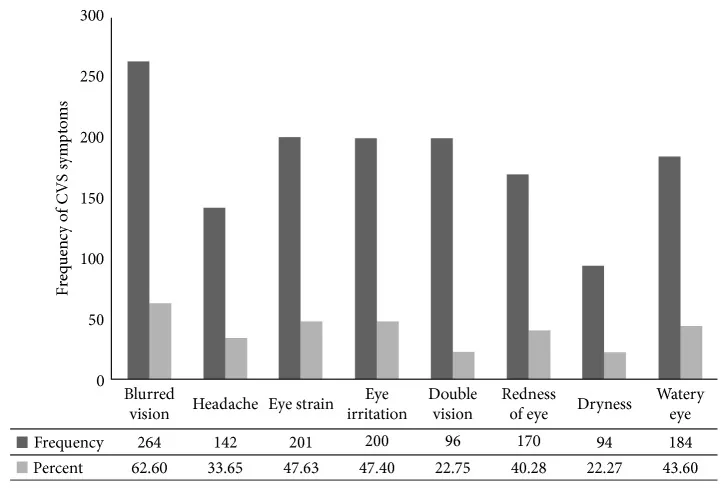
A survey of 422 computer users at a government agency in Ethiopia shows the frequency of each symptom of computer vision syndrome (CVS) in a bar graph and table. Blurred vision (62.6%) is the most common, followed by eye strain (47.6%), eye irritation (47.4%), redness (40.3%), tearing (43.6%), dry eye (22.3%), headache (33.7%), and double vision (22.8%). This corresponds to the subjective symptom profile of accommodative fatigue and ocular surface disorders due to smartphone near work discussed in the section “Main Symptoms and Clinical Findings.”
The subjective symptoms of technostress eye syndrome and smartphone presbyopia include not only eye fatigue, pain, dryness, and blurred vision, but also a variety of symptoms such as neck, shoulder, and arm stiffness, lower back pain, lethargy, numbness in limbs, menstrual irregularities, and even mental symptoms like insomnia and depression.
The main ocular symptoms are shown below.
Symptom
Mechanism
Blurred vision (most common) / Out-of-focus
Accommodative spasm / Disruption of near response synergy
Eye fatigue / Heavy feeling
Sustained tension of ciliary muscle
Dryness and foreign body sensation in the eyes
Increased tear evaporation due to reduced blinking
Changes in blinking: During VDT work, blinking frequency clearly decreases, and combined with office dryness, leads to functional dry eye. After work, blinking increases compensatorily.
Alteration of the near response: The near response (accommodation, miosis, convergence) is normally triggered simultaneously during near vision, but after VDT work, this synergy is disrupted, causing inconsistency in the simultaneous activation of the three components.
Tear film abnormalities: Shortened tear breakup time (TBUT) is observed, indicating evaporative dry eye4). Smartphone use has a particularly large impact on the tear film. Binocular vision abnormalities (convergence insufficiency, increased accommodative lag, fixation disparity) are also important clinical findings of DES5).
Changes in accommodation and convergence function: After prolonged use, decreased accommodative amplitude and recession of the near point of convergence are observed4). In children, acute acquired comitant esotropia (AACE) has been reported.
QWhy does distance vision become blurry after using a smartphone?
A
This is because prolonged near-distance viewing causes the ciliary muscle to become over-tense (accommodative spasm). The ciliary muscle adjusts the thickness of the lens to focus, and contracts when looking at near objects. When it remains in a sustained contracted state, it becomes temporarily difficult to adjust focus for distance. Usually, it recovers with adequate rest, but if it becomes chronic, symptoms may persist.
The development of smartphone-related presbyopia involves a combination of three factors: accommodative mechanisms, ocular surface mechanisms, and environmental factors.
Accommodative Tension Type
Ciliary muscle over-tension: Continuous near work prevents the ciliary muscle from relaxing.
Transient myopia: Distance vision decreases after smartphone use.
Common in young people: Particularly problematic in those aged 10–30 who have high accommodative ability.
Discrepancy in 3D viewing: Accommodation (screen position) and convergence (stereoscopic image) diverge, affecting the autonomic nervous system.
Dry Eye Complicated Type
Decreased blinking: Blink rate significantly decreases while gazing at a screen.
Ocular surface damage: Epithelial damage and inflammation occur, causing foreign body sensation and dryness.
Compensatory increased blinking: Excessive blinking may occur after work.
Environmental Factor Type
Short viewing distance: Smartphones are often used at close distances (30–40 cm) (OR 4.24)6)
Inappropriate ergonomics: Improper screen position and posture (OR 3.87) 6)
Environmental dryness: Humidity below 40% and direct exposure to air conditioning promote tear evaporation 1)
Inappropriate lighting: Glare and luminance contrast worsen visual fatigue
Odds ratios of risk factors quantified by systematic review and meta-analysis are shown 6).
Risk factor
Odds ratio
Short viewing distance
4.24
Inappropriate ergonomics
3.87
Inappropriate posture
2.65
No breaks
2.24
Long duration of use
2.02
Female
1.74
Smartphones have small screens and are used at close distances, so they have the highest CVS severity among all digital devices 4). Furthermore, due to the global increase in smartphone use and the spread of 3D televisions, this condition tends to increase further across a wide age range.
The diagnosis of smartphone presbyopia and technostress eye syndrome is mainly based on the evaluation of clinical symptoms. The following examinations are combined.
In the interview, the work environment, computer work hours, mental state other than eye symptoms (such as insomnia), and medication status including psychotropic drugs and antiallergic drugs are also checked in detail.
Key points of the interview:
Type of digital device (smartphone, PC, tablet, etc.) and daily usage time
Main usage scenarios (work, hobbies, games) and posture/distance
Timing of symptom onset (during use, after use, upon waking up)
Presence of vision fluctuation (whether distance vision becomes blurry after prolonged use)
Symptoms other than eyes (headache, stiff shoulders, sleep disturbance)
Prescription history of glasses or contact lenses and the last update date
Medications taken (check for drugs affecting accommodation function)
Examinations based on VDT work guidelines:
The Ministry of Health, Labour and Welfare’s “Guidelines for Occupational Health Management in VDT Work” recommends the following ophthalmologic examinations for VDT workers:
Visual acuity test (5 m distance and near vision)
Refraction test (confirmation of appropriate correction at 50 cm viewing distance)
Eye position test (presence and degree of heterophoria)
Accommodation function test
A particularly noteworthy point is that distance correction glasses are not optimized for the 30–50 cm distance of VDT work, so the use of progressive addition lenses designed for the VDT work environment is considered effective in preventing the onset of technostress eye syndrome. It is important to explain to patients that VDT work may not be comfortable even with glasses that provide good corrected vision at 30 cm.
A list of main examination methods is shown below.
Examination method
Purpose
Key points
Refraction test
Quantification of accommodative spasm
Comparison with cycloplegic refraction is important
Accommodation function test
Measurement of accommodative amplitude and near point
Near point ruler, repeated measurement, accommodation function analyzer
Visual acuity test
Distance, near, and intermediate
Comparison before and after smartphone use is also useful
Objective fatigue indicators: Visual fatigue can be quantified using critical flicker fusion frequency (CFF), blink analysis (blink rate, proportion of incomplete blinks), pupillary response, etc.1)
Differential diagnosis: Differentiate from dry eye, asthenopia, refractive errors (myopia, hyperopia, astigmatism), accommodative dysfunction, strabismus/heterophoria, and ocular misalignment. Also rule out drug-induced accommodative disorders caused by antiallergic drugs, psychotropic drugs, etc.
Treatment consists of three pillars: environmental/behavioral improvement, pharmacotherapy, and refractive correction.
Environmental/behavioral improvement
Take a 10–15 minute break every hour: Look into the distance to relax the ciliary muscle
Maintain appropriate distance: Keep a distance of 40–70 cm from smartphones and computers
20-20-20 rule: Every 20 minutes, look at something 20 feet (about 6 m) away for 20 seconds8)
Adjust lighting environment: Avoid direct sunlight and ensure adequate indoor lighting. Avoid direct airflow from air conditioning or heating.
Pharmacotherapy
Artificial tears: Soft Santear ophthalmic solution, 2–3 drops per dose, 5–6 times daily
Moisturizing eye drops: Hyalein ophthalmic solution 0.1%, 1 drop per dose, 5–6 times daily, plus Mucosta ophthalmic solution UD 2% or Diquas ophthalmic solution 3%, 1 drop per dose, 5–6 times daily
Treatment for accommodative spasm: Mydrin M ophthalmic solution 0.4%, once daily at bedtime (to relax the ciliary muscle)
Treatment for asthenopia: Sancoba ophthalmic solution 0.02%, 3–5 times daily
Refractive Correction
Appropriate prescription glasses/contact lenses: It is important to avoid under-correction or over-correction.
Intermediate distance glasses: After age 40, glasses for intermediate distance (e.g., computer use) may be needed.
Prism glasses: Indicated when eye misalignment is present.
Blinking exercises: Repeat a set of closing eyes for 2 seconds × 2 times + forceful eyelid closure for 2 seconds4).
Nutritional intervention: According to a systematic review by TFOS, oral omega-3 fatty acid supplementation has high-quality evidence for efficacy in managing DES2). It improves dry eye symptoms on the ocular surface through antioxidant and anti-inflammatory effects.
QHow can I prevent smartphone presbyopia?
A
The most important preventive measures are practicing the 20-20-20 rule (every 20 minutes, look at something 6 meters away for 20 seconds) and maintaining an appropriate distance from the device (40–70 cm). Additionally, consciously increasing blinking, optimizing the work environment (lighting, screen position, humidity), and correcting refractive errors as needed are effective. If symptoms persist or if young individuals experience presbyopia-like symptoms, it is recommended to see an ophthalmologist for accommodation function tests and dry eye tests.
Three main mechanisms are involved in the development of smartphone presbyopia and technostress eye syndrome1).
Overview of the condition:
Smartphone presbyopia should be understood not as a single disease but as a spectrum disorder involving multiple conditions. The three components—accommodative spasm (functional abnormality), dry eye (ocular surface disorder), and convergence insufficiency (binocular vision dysfunction)—mutually exacerbate each other, leading to chronicity and severity. Evaluating each component and addressing them comprehensively is important for long-term improvement.
Prolonged near work causes the ciliary muscle to become over-contracted, fixing the lens in a thick state (for near vision). This makes it difficult to adjust focus for distance, resulting in transient myopia. In young people, the ciliary muscle has higher contractile strength, making them more prone to accommodative spasm. Smartphones are particularly used at close distances and small screens, imposing the highest accommodative load among devices.
2. Decreased Blinking and Worsening of Dry Eye
During VDT work, blinking frequency clearly decreases, and combined with dry office environments, functional dry eye occurs. Normal blink rate is 15–20 times per minute, but it significantly decreases while gazing at a screen. Increased incomplete blinking also promotes tear evaporation, leading to shortened tear break-up time (TBUT) and ocular surface damage. After work, blinking increases compensatorily.
3. Disruption of the Near Triad Coordination
The near triad (accommodation, miosis, convergence) is normally triggered simultaneously during near vision, but after VDT work, this coordination breaks down, causing a mismatch in the simultaneous activation of the three components. This leads to increased exophoria, convergence insufficiency, and fixation disparity, resulting in blurred vision, diplopia, and eye strain. Binocular vision abnormalities (convergence insufficiency, increased accommodative lag) are important pathologies of digital eye strain (DES), especially manifesting after prolonged device use5). In children, it has been reported to manifest as acute acquired comitant esotropia (AACE).
Issues with 3D TV and VR Viewing
When viewing 3D TV, accommodation (physical screen position) and convergence (apparent depth of stereoscopic images) diverge. This divergence can affect the autonomic nervous system, potentially causing eye strain, headache, and nausea.
It has been suggested that increased long-term screen time may contribute to true myopia progression. Particularly in childhood, prolonged near work is known as a risk factor for axial elongation, and smartphone use can be one of the causes. However, the effect on myopia progression is due to a mechanism (axial elongation) that is essentially different from accommodative spasm (pseudomyopia), and the two must be considered separately.
Smartphone use and axial length:
The protective effect of outdoor activity against myopia progression is thought to be mainly due to sunlight promoting retinal dopamine secretion (suppressing axial elongation). Meanwhile, smartphone use is considered to contribute to myopia progression by increasing indoor time as a substitute for near work and reducing outdoor activity time. In other words, in addition to the optical issues of smartphones themselves, lifestyle changes (decreased outdoor activity) are important mediating factors.
Digital devices and sleep:
Smartphone use before bedtime leads to disruption of circadian rhythm (suppression of melatonin secretion) due to blue light, mental hyperactivity, and decreased sleep quality. Sleep deprivation creates a vicious cycle that worsens eye fatigue and accommodative dysfunction the next morning. In the management of smartphone-induced presbyopia, limiting device use before bedtime is an important instruction.
Smartphone-induced presbyopia and correction options:
In patients with smartphone-induced presbyopia, the following correction considerations apply:
Avoid overcorrection: Excessive distance correction increases accommodative effort during near work, worsening smartphone-induced presbyopia
Usefulness of intermediate-distance glasses: After age 40, progressive addition lenses for intermediate distance (50–70 cm) are effective for VDT work
Use of cycloplegic agents: One drop of Mydrin M (0.4% tropicamide) before bedtime can relieve ciliary muscle hypertonicity
Concurrent treatment of dry eye: Dry eye frequently coexists with smartphone-induced presbyopia, so a combination of artificial tears, hyaluronic acid eye drops, and Sancoba eye drops is standard
Prolonged use of digital devices leads to sustained activation of the sympathetic nervous system, resulting in a relative decrease in parasympathetic control (accommodation, blinking, tear secretion). This has recently gained attention as a common underlying mechanism for accommodative spasm, dry eye, and reduced blinking. In addition, autonomic imbalance (insomnia, palpitations, fatigue) after VDT work is understood as part of the systemic symptoms of technostress eye syndrome.
Normal blink rate and incomplete blinking:
Blink rate changes significantly during quiet eye closure, conversation, reading, and VDT work.
Condition
Blink rate (blinks/min)
After quiet eye closure
15–20
During conversation
18–26
During reading
4–8
During VDT work
3–7
During simple calculation
3–5
An increase in incomplete blinks (shallow blinking) is characteristic of VDT work, and because the tear film is not fully reset, ocular surface dryness accelerates. Blinking exercises are an effective training method to correct this incomplete blinking4).
Global trends in prevalence: According to meta-analyses, the pooled prevalence of DES is 66% (95% CI: 59–74%), making it a highly common condition affecting 2 out of 3 people 8). During the COVID-19 pandemic, due to the surge in remote work and online learning, the prevalence rose to 74% (95% CI: 66–81%) 7). Prevalence rates of 82% in non-student populations and 70% in student populations have been reported. Overall, the global prevalence of eye strain is 51% (95% CI: 50–52%), reaching up to 90% among digital device users 11).
Impact on children: DES has been called a “shadow pandemic” in children 9). A study in India found that average screen time doubled from 1.9 hours before COVID to 3.9 hours, and the prevalence of DES in children reached 50.2%. Age ≥14 years, male sex, and device use >5 hours per day were identified as risk factors. Limiting screen time and ensuring outdoor activity time in children are considered important for preventing myopia progression and eye strain.
Eye strain after COVID-19: Cases of hyperopic shift and eye strain symptoms after COVID-19 infection have been reported, suggesting a decline in the ciliary muscle’s ability to maintain accommodation 12). Smartphone-induced presbyopia and accommodation dysfunction as a post-COVID-19 sequelae may share similar mechanisms.
Objective assessment of tear film stability: Development of methods to objectively assess tear film stability is progressing 13). If this technology is clinically applied, it will enable objective diagnosis and monitoring of the dry eye component associated with smartphone-induced presbyopia. Objective assessment of the tear film will become increasingly important in the management of DES.
Advances in nutritional intervention: Supplementation with macular carotenoids (lutein, zeaxanthin, and meso-zeaxanthin) has shown improvements in visual performance and cognitive function, and is expected as an adjunctive approach for DES 10). Omega-3 fatty acid supplementation is positioned as the management method with the highest level of evidence in the TFOS systematic review 2). DHA (docosahexaenoic acid) constitutes approximately 50% of the phospholipids in retinal photoreceptors, and supplementation with omega-3 polyunsaturated fatty acids (PUFAs) has been suggested to be effective in reducing oxidative stress on the ocular surface 14).
Standardized diagnostic tools: Standardized questionnaires are important for evaluating asthenopia and DES15), and the CVS-Q (score ≥6 indicating DES) is widely used. They are useful for capturing a wide range of symptoms, from ocular symptoms (eye fatigue, blurred vision, dry eye) to musculoskeletal symptoms (neck and shoulder pain)16). VDT usage time, work environment, and spectacle correction status have been identified as major determinants of prevalence17), reaffirming the importance of screen time management and work environment optimization.
Response to new technologies: VR (virtual reality) head-mounted displays impose near-distance visual loads different from conventional screens, raising concerns about new effects on accommodation and vergence functions. Development of DES monitoring and prevention systems using AI and wearable devices is also underway. In VR devices, the accommodation distance (focus at a few cm to tens of cm from the eyes) and vergence distance (apparent depth of objects in virtual space) diverge (vergence-accommodation conflict), making eye strain, headache, and nausea particularly problematic with prolonged use. Establishing ophthalmic guidelines for the upcoming XR (extended reality) era remains a challenge.
Wolffsohn JS, Lingham G, Downie LE, et al. TFOS Lifestyle: Impact of the digital environment on the ocular surface. Ocul Surf. 2023 Apr;28:213-252. doi:10.1016/j.jtos.2023.04.004. PMID:37062428.
Wolffsohn JS, Lingham G, Downie LE, et al. TFOS Lifestyle: Impact of the digital environment on the ocular surface. Ocul Surf. 2023 Apr;28:213-252. doi:10.1016/j.jtos.2023.04.004. PMID:37062428.
Pucker AD, et al. Digital Eye Strain: Updated Perspectives. Clin Optom. 2024;16:249-261. doi:10.2147/opto.s412382.
Pavel IA, Bogdanici CM, Donica VC, Anton N, Savu B, Chiriac CP, et al. Computer Vision Syndrome: An Ophthalmic Pathology of the Modern Era. Medicina (Kaunas, Lithuania). 2023;59(2). doi:10.3390/medicina59020412. PMID:36837613; PMCID:PMC9961559.
Barata MJ, et al. A Review of Digital Eye Strain: Binocular Vision Anomalies, Ocular Surface Changes. J Eye Mov Res. 2025. doi:10.3390/jemr18050039. PMID:40989226; PMCID:PMC12452390.
Kirandeep Kaur, Bharat Gurnani, Swatishree Nayak, Nilutparna Deori, Savleen Kaur, Jitendra Jethani, et al. Digital Eye Strain- A Comprehensive Review. Ophthalmol Ther. 2022;11(5):1655-1680. doi:10.1007/s40123-022-00540-9.
León-Figueroa DA, et al. Prevalence of computer vision syndrome during the COVID-19 pandemic. BMC Public Health. 2024;24:640. doi:10.1186/s12889-024-17636-5. PMID:38424562; PMCID:PMC10902934.
Bhattacharya S, et al. Let There Be Light-Digital Eye Strain (DES) in Children as a Shadow Pandemic. Front Public Health. 2022;10:945082. doi:10.3389/fpubh.2022.945082. PMID:36033797; PMCID:PMC9403324.
Lem DW, et al. Can Nutrition Play a Role in Ameliorating Digital Eye Strain? Nutrients. 2022;14(19):4005. doi:10.3390/nu14194005. PMID:36235656; PMCID:PMC9570730.
Song F, Liu Y, Zhao Z, Shang X, Wang Y, Lai M, et al. Clinical manifestations, prevalence, and risk factors of asthenopia: a systematic review and meta-analysis. Journal of global health. 2026;16:04053. doi:10.7189/jogh.16.04053. PMID:41648943; PMCID:PMC12879263.
Thakur M, Panicker T, Satgunam P. Refractive error changes and associated asthenopia observed after COVID-19 infection: Case reports from two continents. Indian journal of ophthalmology. 2023;71(6):2592-2594. doi:10.4103/IJO.IJO_2581_22. PMID:37322686; PMCID:PMC10418019.
Watanabe M, Hirota M, Takigawa R, Kato K, Ikeda Y. Objective Evaluation of Relationship Between Tear Film Stability and Visual Fatigue. Clinical optometry. 2025;17:175-183. doi:10.2147/OPTO.S522320. PMID:40620484; PMCID:PMC12228515.
Hao Duan, Wei Song, Jian Zhao, Wenjie Yan. Polyunsaturated Fatty Acids (PUFAs): Sources, Digestion, Absorption, Application and Their Potential Adjunctive Effects on Visual Fatigue. Nutrients. 2023;15(11):2633. doi:10.3390/nu15112633.
Mylona I, et al. Spotlight on Digital Eye Strain. Clin Optom. 2023;15:29-36. doi:10.2147/opto.s389114.
Kahal F, Al Darra A, Torbey A. Computer vision syndrome: a comprehensive literature review. Future science OA. 2025;11(1):2476923. doi:10.1080/20565623.2025.2476923. PMID:40055942; PMCID:PMC11901492.
Lema AK, Anbesu EW. Computer vision syndrome and its determinants: A systematic review and meta-analysis. SAGE open medicine. 2022;10:20503121221142402. doi:10.1177/20503121221142402. PMID:36518554; PMCID:PMC9743027.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.