Accommodative spasm (tonic accommodation) is a condition in which abnormal tension (abnormal tonus) beyond the physiological range of the ciliary muscle causes pseudomyopia. It consists of two types: physiological tonus (the minimal necessary tension of the ciliary muscle) and abnormal tonus.
Spasm of accommodation is a state of excessive accommodation, which is divided into functional and organic types based on its cause. Functional spasm of accommodation is a symptom due to overwork of the ciliary muscle, where increased tension of the ciliary muscle is observed during fixation. Organic spasm of accommodation occurs in a state of parasympathetic stimulation and refers to involuntary, non-purposeful contraction of the ciliary muscle.
Convergence spasm is a condition in which both eyes adduct paroxysmally and persist. It is also called spasm of the near reflex because it is accompanied by accommodation spasm and miosis. 1)
Pseudomyopia is a concept that pseudomyopia occurs due to prolonged near work and transitions to true myopia. It is classified into the following four types based on etiology.
Inertia of accommodation: The time required to shift focus from far to near is prolonged.
Accommodative palsy: Acute onset of near vision difficulty with marked recession of the near point.
Accommodative constriction: Consists of physiological and abnormal tonus (causing pseudomyopia).
Spasm of accommodation: A state of excessive accommodation (functional or organic).
This condition is common in school-age children and is increasing with the rise in near work and VDT tasks. Organic accommodative spasm is rare; most cases are psychogenic.
Accommodative spasm does not resolve easily, and when it persists for a long time, it has been called pseudomyopia to distinguish it from true myopia.
In the spectrum of accommodative disorders, “spasm” represents an extreme of excessive accommodation, while “ill-sustained accommodation” manifests as difficulty maintaining accommodative power. Fatigue symptoms after VDT work can be understood as a continuous spectrum from ill-sustained accommodation to accommodative constriction and then to spasm.
High-frequency component (HFC) analysis using an accommodative function analyzer (e.g., Speedy-K) is useful for understanding the pathophysiology and serves as an objective indicator of accommodative constriction and spasm. Daily eye fatigue often reflects this high HFC state.
QHow is pseudomyopia different from true myopia?
A
Pseudomyopia is a temporary myopic shift due to accommodative constriction, and refraction under cycloplegia (e.g., Mydrin P) returns to emmetropia or mild hyperopia. True myopia is an organic myopia due to axial elongation and remains myopic even under cycloplegia. Cycloplegic refraction is essential for differentiation.
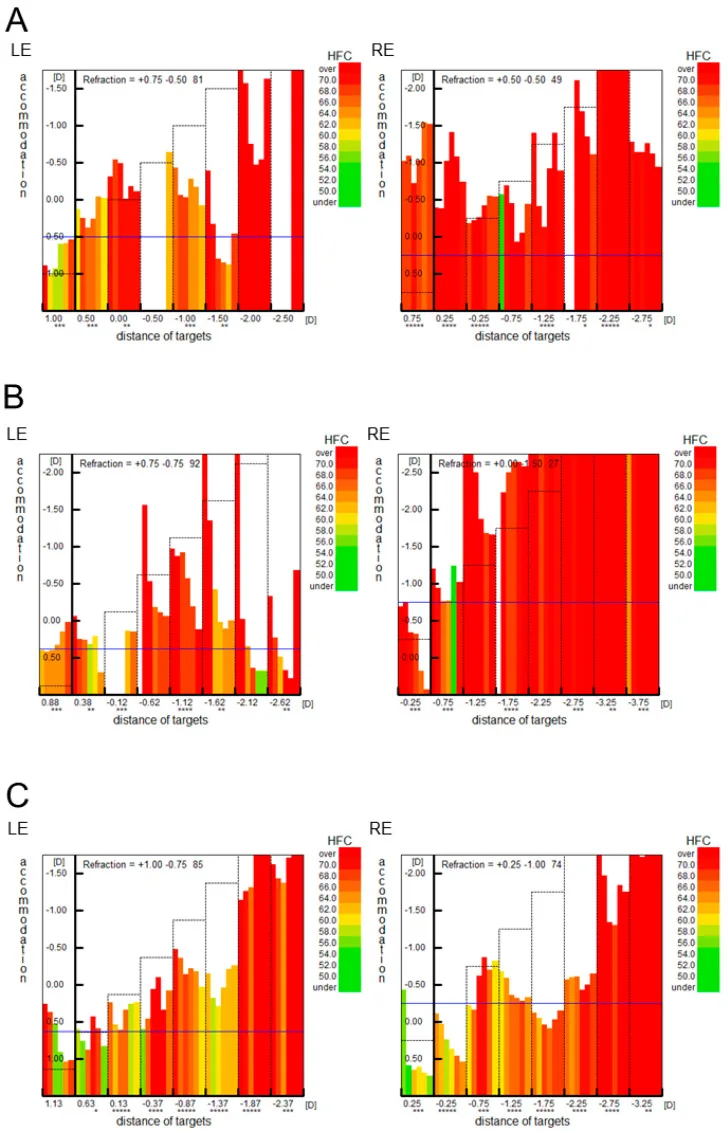
Accommodative microfluctuation analysis (Fk-map): In accommodative spasm, the Fk-map shows that the refractive value closely follows the accommodative stimulus target, but overall HFC (high-frequency component) values are high. This reflects the subjective symptom of daily eye fatigue.
Fk-map of accommodative spasm: When trying to view the presented target, accommodation overacts and increases the refractive value. HFC values remain high, indicating a state prone to eye fatigue.
Refractive fluctuation: A marked difference in refractive values is observed under cycloplegia versus non-cycloplegia. This difference corresponds to the pseudomyopic component.
QCan accommodative spasm occur in adults?
A
It also occurs in adult VDT workers. 2) Particularly in young adults who use smartphones or computers for long periods, it manifests as decreased distance vision after near work and eye strain. Organic convergence spasm is also more common in adults, and both psychogenic and functional types can occur at any age.
VDT work / prolonged near work: Increased tension due to fatigue of the ciliary muscle
Psychogenic (conversion disorder): Mental distress or anxiety as a trigger
Environmental factors: Inappropriate lighting, working distance, or posture
Decreased blink rate: Promotes the complication of dry eye
Organic (parasympathetic stimulation)
Head trauma: Stimulation of the convergence center
Multiple sclerosis3): Effect on the convergence center due to central nervous system demyelination
Metabolic encephalopathy / tumor: Organic lesions at the level of the dorsal midbrain
Arnold-Chiari malformation: Involvement due to congenital malformation of the posterior cranial fossa
Drug intoxication: Organophosphate pesticides and sarin poisoning cause pinpoint pupils (pin-hole pupil) and accommodative spasm.
Anticholinesterase eye drops for eyelid elevation: May cause miosis and accommodative spasm
In many cases of convergence spasm, no organic disease is found, and psychogenic factors such as conversion disorder (hysteria) are the main cause. It can also occur due to increased irritability of the convergence center at the midbrain dorsal level or organic lesions that stimulate the neural mechanism of convergence, but this is extremely rare.
In patients with conversion disorder or psychosomatic disorders, mental stress and anxiety can trigger accommodative spasm through mechanisms that induce the near response. Strong stress in the classroom environment (e.g., bullying, exams) is often associated with the onset of pseudomyopia in school-age children. After excluding organic diseases, if the cause is determined to be psychogenic, the cornerstone of treatment is to alleviate the patient’s anxiety and reduce life stress. Collaboration with psychiatry or psychosomatic medicine may be necessary.
Ueki S, et al. Spasm of Near Reflex in a Patient with Autism Spectrum Disorder: A Case Report. Reports (MDPI). 2023;6(3):38. Figure 1. PMCID: PMC12225246. DOI: 10.3390/reports6030038. License: CC BY 4.0.
Speedy K (Righton Co.) accommodative microfluctuation analysis shows that HFC (high-frequency components) are predominant (red bars) in both eyes across all areas, confirming a persistent accommodative spasm pattern over time. This corresponds to the objective examination findings of accommodative spasm discussed in the section “Diagnosis and Examination Methods.”
Diagnosis is primarily based on clinical findings and cycloplegic refraction.
① History and visual acuity testing: Obtain detailed information about near work and VDT time, work environment, and medication use (e.g., psychotropic drugs, antiallergic drugs). Measure distance and near visual acuity, and check for fluctuations depending on time of day or after rest.
② Non-cycloplegic refraction: Measure refractive error with accommodation active.
③ Cycloplegic refraction (essential for definitive diagnosis): Instill Mydrin P® (tropicamide 0.5% and phenylephrine 0.5% combination) and repeat refraction after 30–60 minutes. If the refraction returns to emmetropia or mild hyperopia under cycloplegia, pseudomyopia (accommodative spasm) is confirmed. If myopia persists under cycloplegia, it is true myopia. For severe symptoms, consider using Cyclogyl® (cyclopentolate 1%) for strong cycloplegia and precise refraction.
④ Accommodative function tests: Near point measurement (repeated near point measurement), HFC analysis using an accommodative function analyzer.
⑤ Ocular alignment and convergence tests: In convergence spasm, paroxysmal high-angle esotropia is observed. Performing monocular duction movements is important.
⑥ Pathophysiological analysis (if needed): Simultaneous measurement of accommodation, miosis, and convergence using a binocular wavefront sensor helps understand the condition.
QHow is it distinguished from abducens nerve palsy?
A
Abducens nerve palsy does not involve miosis or accommodative disturbances, and the abduction limitation is unilateral and non-fluctuating. In accommodative spasm/convergence spasm, the monocular duction test resolves the abduction limitation and miosis. Also, a highly variable convergence angle is characteristic. For details, see the section “Diagnosis and Examination Methods”.
Treatment of Functional Accommodative Spasm (Pseudomyopia)
Environmental Improvement (First Choice): Identifying and eliminating the cause is the highest priority. VDT work should be limited to a maximum of 1 continuous hour, followed by a 10-15 minute break.
Prescription of Near-Vision Glasses: Prescribe near-vision glasses tailored to the working distance. Intermediate-near progressive addition lenses are appropriate. Distance-near progressive lenses are unsuitable because the near portion is too small. Progressive power lenses designed for VDT work environments are considered effective in preventing technostress eye syndrome.
Mydrin M Eye Drops (0.4% Tropicamide): Instill one drop before bedtime to relax the ciliary muscle. Cycloplegic agents (parasympatholytics) relax the ciliary muscle and relieve tension. Bedtime instillation avoids the impact of pupillary dilation on daytime visual function.
Oral Vitamin B Preparations: Used to maintain and improve nerve function.
Management of Dry Eye Complication: Use artificial tears or hyaluronic acid-containing eye drops for dry eye associated with decreased blinking.
Treatment of Organic Accommodative Spasm (Convergence Spasm)
Prioritize Treatment of the Underlying Disease: If an organic disease is the cause, treatment of the primary disease takes precedence. If neurological or systemic findings are present, actively perform imaging studies.
Psychological Support: In psychogenic (non-organic) cases, strive to alleviate the patient’s anxiety.
Monocular Occlusion: May be effective in relieving convergence spasm.
Cycloplegic Eye Drops: Used when spasm persists (e.g., atropine).
Spontaneous remission: Most cases resolve spontaneously.
Key points for environmental and behavioral guidance
Guidance for patients with functional accommodative spasm or pseudomyopia due to VDT work:
Improvement of VDT work environment:
Maintain a working distance of 30–40 cm (especially avoid holding smartphones too close)
Limit continuous work to 1 hour maximum, and take a 10–15 minute break without fail
During breaks, look into the distance to relax the ciliary muscle
Set the monitor height slightly below eye level
Ensure adequate lighting and prevent glare
Avoid direct air conditioning or heating airflow to the face and eyes
Screen usage rules:
Follow the “20-20-20 rule” (every 20 minutes, look at something 20 feet away for 20 seconds)
Avoid using smartphones while lying down, and keep the screen at least 40 cm away
Avoid using smartphones before bedtime
Be aware of recording and managing total daily screen time
Special considerations for children:
In school-age accommodative spasm (pseudomyopia), accurate refraction under cycloplegia is essential to differentiate from true myopia. Limiting smartphone/tablet use and ensuring outdoor activities (recommended at least 2 hours per day) are important for preventing accommodative spasm and suppressing myopia progression.
Changes in subjective symptoms: Confirm improvement in distance vision loss and eye fatigue symptoms
Improvement in visual acuity: Compare distance corrected visual acuity before and after treatment
Re-evaluation of accommodative function: Re-measure refraction under cycloplegia 2–4 weeks after treatment
Fk-map changes: Confirm normalization of HFC values (objective indicator of treatment effect)
Check VDT work environment: Confirm whether the guidance is being followed
Continuation of environmental improvements is essential to prevent recurrence. Even after patients feel they have improved, if VDT work habits are not corrected, recurrence is likely. Especially in school-age children and adolescents, if smartphone or game addiction is the root cause, cooperation with parents and schools is necessary.
Course of organic convergence spasm:
In organic convergence spasm, treatment and follow-up of the underlying disease take priority. Most psychogenic cases resolve spontaneously, but psychological support and regular follow-up are important. Since true neurological diseases (e.g., multiple sclerosis) may develop over the long term, detailed neurological examination and, if necessary, imaging (MRI) should not be neglected in the initial evaluation.
A clinically important point is the existence of a mixed type where “pseudomyopic component” and “true myopic component” coexist. This corresponds to cases where the amount of myopia decreases under cycloplegic refraction but does not return to complete emmetropia. In this mixed type:
The refractive value under cycloplegia is used as the standard for prescription as the “true myopia component”.
The difference before and after cycloplegia (pseudomyopia component) is quantified and set as a treatment target.
Regularly reassess whether the pseudomyopia component has improved.
Especially in school-age children, mixed types are common at the first visit. Improvement of the pseudomyopia component through environmental improvements and cycloplegic treatment may lead to a reduction in prescription power. However, to prevent the progression of true myopia, separate consideration of myopia progression control treatments such as low-concentration atropine eye drops or orthokeratology is necessary.
In many cases, improvement occurs within 2 to 4 weeks with appropriate environmental improvements and treatment.
Continuous improvement of lifestyle habits is essential to prevent recurrence.
If true myopia is latent, appropriate myopia-correcting glasses prescription is necessary after pseudomyopia treatment.
Since pseudomyopia in school-age children may be a precursor to the progression of true myopia, regular follow-up is performed.
Prognosis of organic convergence spasm:
Depends on the treatment course of the underlying disease.
In psychogenic cases, a good prognosis can be expected.
If due to neurological disease, it depends on the progression of the underlying disease.
QWill it heal naturally without treatment?
A
In psychogenic cases, most cases resolve spontaneously. In functional cases (VDT overwork), improvement is often seen with improvements in the VDT environment, use of appropriate glasses, and instillation of artificial tears. However, in organic cases, treatment of the underlying disease is necessary, and if left untreated, improvement may not occur.
The near reflex is a physiological response in which convergence, accommodation, and miosis occur simultaneously as a supranuclear binocular associated movement when viewing near objects. These cannot be consciously separated.
The supranuclear fibers to the Edinger-Westphal nucleus (EW nucleus) for the near reflex run ventral to the midbrain pretectal area and posterior commissure through which the afferent fibers of the pupillary light reflex pass. The ratio of neurons involved in the light reflex and accommodation in the ciliary ganglion is 3:97, with accommodation-related cells overwhelmingly predominant.
Details of innervation:
Neural pathway of accommodation:
Parieto-occipital cortex (visual association area) → midbrain accommodation and convergence center
Depending on which part of this pathway is abnormal causing accommodative spasm, it is classified as functional (overwork, psychogenic) or organic (neurological disorder).
Dissociation from the pupillary light reflex:
The near reflex (miosis, accommodation, convergence) is controlled by a pathway anatomically different from that of the pupillary light reflex. The afferent pathway of the light reflex passes through the midbrain pretectal area, while the afferent pathway of the near reflex runs more ventrally. Therefore, in Argyll Robertson pupils (due to midbrain lesions from syphilis, diabetes, etc.), the near reflex (miosis) is preserved even when the light reflex is lost, resulting in “light-near dissociation.” This dissociation is an important concept in understanding the neuroanatomy of convergence spasm.
Interrelationship of accommodation, convergence, and miosis:
The three components of the near reflex do not occur independently but normally function in coordination. These relationships can be summarized as follows:
Accommodative convergence (AC/A ratio): The ratio of how many prism diopters (Δ) of convergence occur per 1 D of accommodative change.
Convergence accommodation (CA/C ratio): The accommodative change that occurs in response to a change in convergence.
Linkage between miosis and accommodation: Miosis during accommodation increases depth of focus, improving near visual acuity.
In accommodative spasm, excessive accommodation is accompanied by increased convergence and miosis. Conversely, in accommodative insufficiency, accommodative failure may lead to convergence insufficiency and relative mydriasis. Understanding these interrelationships clarifies the usefulness of tests that measure all three elements simultaneously (wavefront sensors, near response measurement devices).
Pathophysiology of accommodative spasm and accommodative spasm
Functional accommodative spasm: Prolonged VDT work or near tasks cause the ciliary muscle to become fatigued, leading to insufficient relaxation. This results in persistent myopia and asthenopia. In the Fk-map of accommodative spasm, the refractive value follows the target well, but the HFC value is generally high, reflecting eye fatigue.
Accommodative spasm: In the Fk-map, when trying to see the presented target, accommodation works excessively, increasing the refractive value. The HFC value also remains high. Cases that do not improve easily and persist for a long time are called pseudomyopia.
Abnormal tonus in accommodative spasm: Caused by persistent insufficient relaxation of the ciliary muscle. This maintains the lens in a constantly bulging state (myopia), leading to decreased distance vision and asthenopia.
Convergence spasm is caused by increased irritability of the convergence center at the midbrain dorsal level, or by organic lesions that stimulate the neural mechanism of convergence. In conversion disorder (psychogenic), mental stress may induce the near response, leading to persistent involuntary convergence contraction.
Pseudo sixth nerve palsy:
Convergence spasm is sometimes misdiagnosed as abducens nerve palsy. This condition is called pseudo sixth nerve palsy. Monocular duction (pull test) is used for differentiation. In abducens nerve palsy, abduction limitation does not change with occlusion of one eye, but in convergence spasm, monocular duction eliminates adduction and miosis and normalizes abduction, which is a definitive differentiating finding.
With the widespread use of smartphones and game consoles, reports of accommodative spasm in young people are increasing. Prolonged near-distance screen use is thought to induce sustained tension in the ciliary muscle, and it is attracting attention as a factor in the increase of functional accommodative spasm.
After the COVID-19 pandemic, children’s screen time doubled (from 1.9 hours to 3.9 hours), and increases in accommodative spasm and pseudomyopia have been reported 7). Particularly, age 14 or older, male sex, and device use exceeding 5 hours per day have been identified as risk factors 9).
The prevalence of digital eye strain (DES) rose to 74% (95% CI: 66–81%) during the COVID-19 pandemic 8), and increased screen time has become an important trigger for accommodative spasm10). Ongoing research is being conducted on the relationship between pseudomyopia treatment with cycloplegic drugs and myopia progression control 12).
The Tear Film & Ocular Surface Society (TFOS) indicates that omega-3 fatty acid supplementation is the nutritional intervention with the highest level of evidence for managing digital eye strain13). Research is also progressing on the breakdown of the three components of the near response after VDT work 6).
An association between acute acquired comitant esotropia (AACE) in children and prolonged smartphone use has also been reported 11), drawing attention to effects on the convergence and accommodation systems. Evaluation of binocular vision is essential for managing accommodative spasm and convergence spasm 5), and a comprehensive approach is required as a digital device-related eye disease 14)15)16).
Goldstein JH, Schneekloth BB. Spasm of the near reflex: a spectrum of anomalies. Survey of ophthalmology. 1996;40(4):269-78. doi:10.1016/s0039-6257(96)82002-9. PMID:8658338.
Hussaindeen JR, Mani R, Agarkar S, Ramani KK, Surendran TS. Acute adult onset comitant esotropia associated with accommodative spasm. Optometry and vision science : official publication of the American Academy of Optometry. 2014;91(4 Suppl 1):S46-51. doi:10.1097/OPX.0000000000000182. PMID:24584303.
Rosenberg ML. Spasm of the near reflex mimicking myasthenia gravis. Journal of clinical neuro-ophthalmology. 1986;6(2):106-8. PMID:2942565.
Wolffsohn JS, Lingham G, Downie LE, et al. TFOS Lifestyle: Impact of the digital environment on the ocular surface. Ocul Surf. 2023 Apr;28:213-252. doi:10.1016/j.jtos.2023.04.004. PMID:37062428.
Pavel IA, Bogdanici CM, Donica VC, Anton N, Savu B, Chiriac CP, et al. Computer Vision Syndrome: An Ophthalmic Pathology of the Modern Era. Medicina (Kaunas, Lithuania). 2023;59(2). doi:10.3390/medicina59020412. PMID:36837613; PMCID:PMC9961559.
Bhattacharya S, et al. Let There Be Light-Digital Eye Strain (DES) in Children as a Shadow Pandemic. Front Public Health. 2022;10:945082. doi:10.3389/fpubh.2022.945082. PMID:36033797; PMCID:PMC9403324.
León-Figueroa DA, et al. Prevalence of computer vision syndrome during the COVID-19 pandemic. BMC Public Health. 2024;24:640. doi:10.1186/s12889-024-17636-5. PMID:38424562; PMCID:PMC10902934.
Song F, Liu Y, Zhao Z, Shang X, Wang Y, Lai M, et al. Clinical manifestations, prevalence, and risk factors of asthenopia: a systematic review and meta-analysis. Journal of global health. 2026;16:04053. doi:10.7189/jogh.16.04053. PMID:41648943; PMCID:PMC12879263.
Kirandeep Kaur, Bharat Gurnani, Swatishree Nayak, Nilutparna Deori, Savleen Kaur, Jitendra Jethani, et al. Digital Eye Strain- A Comprehensive Review. Ophthalmol Ther. 2022;11(5):1655-1680. doi:10.1007/s40123-022-00540-9.
Thakur M, Panicker T, Satgunam P. Refractive error changes and associated asthenopia observed after COVID-19 infection: Case reports from two continents. Indian journal of ophthalmology. 2023;71(6):2592-2594. doi:10.4103/IJO.IJO_2581_22. PMID:37322686; PMCID:PMC10418019.
Wolffsohn JS, Lingham G, Downie LE, et al. TFOS Lifestyle: Impact of the digital environment on the ocular surface. Ocul Surf. 2023 Apr;28:213-252. doi:10.1016/j.jtos.2023.04.004. PMID:37062428.
Barata MJ, et al. A Review of Digital Eye Strain: Binocular Vision Anomalies, Ocular Surface Changes. J Eye Mov Res. 2025. doi:10.3390/jemr18050039. PMID:40989226; PMCID:PMC12452390.
Lem DW, et al. Can Nutrition Play a Role in Ameliorating Digital Eye Strain? Nutrients. 2022;14(19):4005. doi:10.3390/nu14194005. PMID:36235656; PMCID:PMC9570730.
Ueki S, Hasegawa Y, Hatase T, Hanyu T, Egawa J, Miki A, Fukuchi T.. Spasm of Near Reflex in a Patient with Autism Spectrum Disorder: A Case Report. Reports (MDPI). 2023;6(3):38. doi:10.3390/reports6030038. PMID:40729206; PMCID:PMC12225246.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.