Abducens nerve palsy is an eye movement disorder caused by paralysis of the abducens nerve (sixth cranial nerve), which is the motor neuron of the lateral rectus muscle 1. When the abducens nerve is paralyzed, tension in the lateral rectus muscle decreases, resulting in poor abduction (outward movement) of the affected eye. This leads to paralytic (incomitant) esotropia. Due to this esotropia, the patient experiences ipsilateral diplopia (non-crossed diplopia), which worsens on lateral gaze toward the affected side, i.e., the direction of poor abduction.
The course of the abducens nerve begins at the nucleus in the pons, exits the brainstem ventrally, ascends along the clivus of the sphenoid bone, passes through the cavernous sinus, and reaches the lateral rectus muscle in the orbit via the superior orbital fissure. Damage can occur at any point along this course 1. The long intracranial course is an anatomical factor that makes the abducens nerve vulnerable to trauma.
Abducens nerve palsy is one of the representative ocular motor nerve palsies, along with oculomotor and trochlear nerve palsy. In an analysis of 807 cases, the most common cause was microcirculatory disorder (ischemic) at 36.7%, followed by idiopathic 17.7%, tumor 14.3%, vascular abnormality 10.2%, inflammatory 9.4%, and traumatic 4.3% 2. A notable feature compared to oculomotor and trochlear nerve palsy is the higher frequency of tumors, and tumor as a cause must always be considered in both adults and children. In children, particular attention should be paid to glioma3. Additionally, during increased intracranial pressure, bilateral mild abducens nerve palsy may occur, known as a false localizing sign, which does not indicate the location of the lesion 1.
An overview of the main causes is shown below.
Cause Category
Representative Diseases/Conditions
Remarks
Peripheral circulatory disorder (ischemic)
Diabetes, hypertension, arteriosclerosis
Most common in adults (approx. 37–44%). Often resolves spontaneously2,4
More frequent than other ocular motor nerve palsies (approx. 14%)2
Trauma
Head trauma
Long course makes it vulnerable
Increased intracranial pressure
Intracranial mass, hydrocephalus
Appears as bilateral false localizing sign
Inflammation/infection
Cavernous sinus thrombosis, meningitis
Often accompanied by other cranial nerve palsies
Congenital
Developmental anomaly
Important in differential diagnosis in children
QIs abducens nerve palsy a rare disease?
A
Among ocular motor nerve palsies, it is a common condition and is encountered in daily ophthalmology outpatient clinics. Cases due to peripheral circulatory disorders are the most common in adults (36–44%), and caution is needed in patients with underlying diabetes or hypertension 2,4. In children, however, the possibility of increased intracranial pressure or tumors is relatively high, requiring a different approach than in adults 3,6.
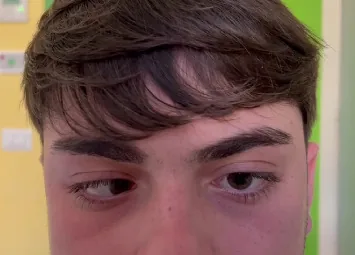
Paparella R, et al. Isolated Abducens Nerve Palsy in an Adolescent With Confounding Multisystem Serology: A Case Report and Diagnostic Review. Case Rep Pediatr. 2025. Figure 1. PMCID: PMC12488298. License: CC BY.
On left gaze, marked abduction limitation is observed in the left eye, consistent with left abducens nerve palsy. This corresponds to the abduction limitation discussed in the section “2. Main Symptoms and Clinical Findings.”
Diplopia (homonymous, non-crossed): In abducens nerve palsy, abduction of the affected eye is limited. Therefore, the separation of the two images is greatest on lateral gaze toward the affected side. In left abducens nerve palsy, diplopia is most severe when looking to the left. Diplopia is more noticeable at distance than at near.
Compensatory head posture (face turn): To avoid diplopia, the patient turns the face toward the side of the paralyzed eye. In left abducens nerve palsy, the face is turned to the left. This reduces the demand for gaze toward the abduction direction of the affected eye, eliminating diplopia.
Paralytic esotropia: Due to poor abduction of the affected eye, esotropia is observed in primary position (straight ahead). The strabismus angle increases as gaze is directed toward the affected side (incomitant).
Ocular movement limitation: Abduction of the affected eye is limited; in severe cases, the eye cannot cross the midline. In mild to moderate palsy, abduction is only weakened, and some eye movement in the abduction direction remains.
Mild to Moderate Palsy
Eye movement: Abduction is reduced, but abduction beyond the midline is possible.
Strabismus angle: Increases on lateral gaze to the affected side, but the deviation in primary position is relatively small.
Hess chart: The pattern is reduced in the abduction direction of the affected eye. The pattern is enlarged in the corresponding direction (adduction) of the healthy eye (overaction of the yoke muscle due to Hering’s law).
Severe palsy
Eye movement: The affected eye cannot cross the midline. Pursuit eye movements in the abduction direction are almost absent.
Strabismus angle: Marked esotropia even in primary position. Esotropia increases significantly when looking toward the affected side.
Hess chart: Marked pattern reduction in the abduction direction of the affected eye. Enlargement of the pattern in the healthy eye is also prominent.
Hess chart findings: The Hess chart is a useful test for quantifying eye movement disorders and monitoring their course. In abducens nerve palsy, the pattern is reduced in the outward direction (abduction) of the affected eye, and the pattern is enlarged in the corresponding direction (adduction) of the healthy eye. This is because, according to Hering’s law (equal innervation to yoke muscles), excessive neural firing to the abducens nucleus of the paralyzed eye is also transmitted to the medial rectus muscle of the contralateral eye.
QIn what situations is diplopia due to abducens nerve palsy most noticeable?
A
Diplopia becomes prominent during distance vision and lateral gaze to the affected side (gaze movement in the abduction direction). For example, in left abducens nerve palsy, two images appear when looking at a distant sign or when looking to the left. Conversely, diplopia disappears when the patient assumes a compensatory head posture (turning the face to the left). The strabismus angle tends to be smaller during near vision, making diplopia less noticeable.
Different causative diseases occur at various sites along the course of the abducens nerve. They are organized by the site of the lesion.
Nucleus / Brainstem (Pons)
Characteristics of pontine lesions: The abducens nucleus is located near the midline of the pons, adjacent to the paramedian pontine reticular formation (PPRF). Pontine lesions often cause ipsilateral horizontal gaze palsy in addition to abducens nerve palsy.
Foville syndrome: Lesion in the lower pons. Presents with ipsilateral abducens nerve palsy + horizontal gaze palsy + facial nerve palsy.
Raymond syndrome: Lower pontine lesion. Presents with ipsilateral abducens nerve palsy + contralateral hemiparesis (pyramidal tract disorder).
Subarachnoid space / Clivus
Trauma vulnerability: The intracranial course of the abducens nerve is the longest, making it susceptible to traction and compression from head trauma.
Increased intracranial pressure (false localizing sign): Because the nerve bends sharply at Dorello’s canal (bony canal on the sphenoid clivus), it is most vulnerable when intracranial pressure is elevated. It can occur bilaterally.
Tumors: Cerebellopontine angle tumors (acoustic neuroma, meningioma), skull base invasion of nasopharyngeal tumors.
Cavernous sinus
Combined cranial nerve palsy: Within the cavernous sinus, besides the abducens nerve (VI), the oculomotor nerve (III), trochlear nerve (IV), and trigeminal nerve branches V1 and V2 also run. Abducens nerve palsy can appear as part of a combined palsy (cavernous sinus syndrome).
Diseases requiring differentiation: Orbital wall fracture (entrapment of medial rectus), thyroid eye disease (restriction due to fibrosis of medial rectus), and external ophthalmoplegia can present with abduction limitation similar to abducens nerve palsy.
Differentiation method: Confirm mechanical cause of abduction limitation with forced duction test. Check for medial rectus hypertrophy or orbital fracture with CT/MRI.
Risk factors: Diabetes, hypertension, arteriosclerosis (main cause of ischemia), head trauma, increased intracranial pressure (hydrocephalus, tumor), tumors (glioma, cerebellopontine angle tumor) 2,4. In the microcirculatory disorder group, the mean age is 62.8 years, significantly higher than other cause groups (44.5 years), and the rate of diabetes comorbidity is also significantly higher 4.
It is possible. In increased intracranial pressure (due to intracranial tumor, hydrocephalus, pseudotumor cerebri, etc.), the abducens nerve may be stretched or compressed at the Dorello canal, causing bilateral abducens nerve palsy. In this case, abducens nerve palsy is a false localizing sign that occurs regardless of the lesion location, and it is important to investigate the underlying disease.
Cover test: Confirm esotropia in primary position. Confirm that the strabismus angle increases on lateral gaze to the affected side, and diagnose incomitant strabismus (paralytic strabismus). Quantify the strabismus angle with the prism alternate cover test.
Ocular motility evaluation: Evaluate eye movements in nine directions (horizontal, vertical, and oblique) to confirm the direction and degree of abduction limitation. Distinguish whether abduction limitation is within the midline (mild to moderate) or cannot cross the midline (severe).
Hess chart: Confirm pattern contraction in the abduction direction of the affected eye and pattern expansion in the corresponding direction of the healthy eye. It is also useful as an indicator for follow-up.
Imaging studies are essential for investigating the cause of abducens nerve palsy. Evaluate the presence of lesions in the brainstem, skull base, cavernous sinus, and orbital region. In a multicenter prospective study of acute isolated ocular motor nerve palsy in patients aged 50 years or older, other causes such as tumor, inflammation, and giant cell arteritis were identified in 10% of cases with only vascular risk factors, and brain MRI evaluation is recommended regardless of the presence of vascular risk factors5.
Examination Method
Features/Uses
MRI (including contrast)
Highest priority for detecting lesions in the brainstem, skull base, cavernous sinus, and orbit. Useful for evaluating tumors, inflammation, and infarction.
CT
Useful for evaluating orbital wall fractures and bone-destructive lesions.
MRA/CTA
Used to rule out vascular lesions (aneurysms, arteriovenous fistulas)
Orbital wall fractures, extraocular myositis, and thyroid eye disease (restriction of the medial rectus) can cause pseudo-abduction deficit, which mimics abducens nerve palsy; therefore, imaging evaluation of orbital lesions is also necessary.
A wide range of diseases that cause abduction limitation must be considered.
Thyroid eye disease (Graves disease): Fibrosis and hypertrophy of the medial rectus restrict abduction. CT/MRI shows medial rectus hypertrophy. Positive forced duction test (mechanical restriction of abduction). Thyroid function tests, proptosis, and lid retraction are also helpful.
Orbital blowout fracture (medial wall fracture): Entrapment of the medial rectus or orbital contents. Differentiated by trauma history, forced duction test, and CT.
Myasthenia gravis: Diurnal variation (worse in the evening), ice test (improvement of ≥2 mm after 2 minutes of ice pack application; sensitivity 80–92%), and anti-AChR antibody testing help differentiate.
Duane syndrome (Duane retraction syndrome): Congenital abduction limitation with globe retraction and palpebral fissure narrowing on adduction. Caused by congenital absence of the abducens nerve and aberrant innervation of the lateral rectus by the oculomotor nerve. Symptoms present since early childhood.
Internuclear ophthalmoplegia (INO): Primarily involves adduction limitation due to medial longitudinal fasciculus (MLF) lesion; usually does not cause abduction limitation, but may need to be differentiated from unilateral abduction deficit.
QAre there diseases that can be confused with abducens nerve palsy?
A
Thyroid eye disease and Duane syndrome are particularly confusing. Thyroid eye disease mechanically restricts abduction due to fibrosis of the medial rectus. It can be differentiated by a positive forced duction test, medial rectus hypertrophy on CT/MRI, proptosis, and lid retraction. Duane syndrome is characterized by congenital abduction limitation with globe retraction and palpebral fissure narrowing on adduction, with symptoms present since childhood. Both can be differentiated by a combination of ocular motility evaluation and imaging.
Treatment of the underlying cause is the highest priority. If tumor, inflammation, or vascular lesion is the cause, specific treatment for each should be initiated first.
Observation: Since spontaneous improvement is common, conservative observation is performed for about 6 months.
Medication: Vitamin preparations (e.g., vitamin B12) and circulation-improving drugs are administered to support nerve recovery.
Management of underlying diseases: Strict control of diabetes and hypertension is important for recovery.
Prism glasses
Indications: Prescribed for cases with mild strabismus to improve subjective symptoms of diplopia.
Timing of prescription: Prescribed when symptoms are stable. In the acute phase with large eye position fluctuations, the indication should be carefully considered.
Surgical treatment (no improvement after 6 months)
Surgery is considered when conservative treatment for more than 6 months does not improve eye position or diplopia. The surgical procedure is selected based on the degree of palsy.
Horizontal muscle transposition. The most standard procedure.
Severe (cannot abduct past midline)
Muscle transposition (full-width transposition of superior and inferior rectus muscles)
The full width of the superior and inferior rectus muscles is moved toward the insertion of the lateral rectus muscle. Includes Jensen procedure, Hummelsheim procedure, etc.
The goal of treatment is to improve eye alignment in primary position (straight ahead) and eliminate diplopia.
QWhen should surgery be considered?
A
Surgery is considered when conservative treatment for more than 6 months does not improve eye alignment or diplopia. The surgical procedure is selected based on the degree of palsy: for mild to moderate palsy where abduction past midline is possible, lateral rectus resection combined with medial rectus recession is performed; for severe palsy where abduction past midline is not possible, muscle transposition using the superior and inferior rectus muscles (full-width transposition) is selected. Preoperatively, adequate explanation about residual diplopia on lateral gaze is necessary.
6. Pathophysiology and detailed mechanism of onset
The abducens nucleus is located in the paramedian pons (just below the facial colliculus). The abducens nucleus has two important types of output.
Motor neurons to the ipsilateral lateral rectus muscle: Project peripherally as the abducens nerve, responsible for abduction of the ipsilateral eye.
Interneurons via the medial longitudinal fasciculus (MLF) to the contralateral oculomotor nucleus: Project to the contralateral medial rectus nucleus, coordinating conjugate horizontal eye movements.
The abducens nucleus is closely associated with the paramedian pontine reticular formation (PPRF: the horizontal gaze center). The PPRF issues commands for voluntary rapid horizontal eye movements (saccades) and forms direct synapses with the abducens nucleus.
In abducens nerve palsy, it is clinically important to distinguish whether the lesion is in the nucleus (pons) or in the peripheral nerve (distal to the pons).
Nuclear lesion: Destruction of the abducens nucleus often involves not only simple abducens nerve palsy but also the PPRF. As a result, in addition to abducens nerve palsy, horizontal gaze palsy to the ipsilateral side (inability to deviate the eye toward the affected side) occurs. The difference from peripheral lesions is that all eye movements toward the affected side (both abduction and adduction) are impaired.
Peripheral lesion: Causes only pure abduction limitation of the affected eye. It is not accompanied by internuclear ophthalmoplegia (INO) or other adduction deficits.
Increased intracranial pressure and false localizing sign
The abducens nerve runs with an acute bend in Dorello’s canal (a bony and dural canal formed between the posterior clinoid process of the sphenoid bone and the petrous apex). When intracranial pressure increases, the abducens nerve is easily stretched and compressed at this site. As a result, palsy occurs at a site not directly related to the intracranial lesion (pons or abducens nerve territory). This is called a false localizing sign, and when it appears as bilateral abducens nerve palsy, it is an important sign of increased intracranial pressure. It is necessary to investigate tumors, hydrocephalus, pseudotumor cerebri (idiopathic intracranial hypertension), etc.
Special features of pediatric abducens nerve palsy
Pediatric abducens nerve palsy has a different etiological distribution from that in adults. While peripheral circulatory disorders are common in adults, tumors (especially brainstem gliomas) account for a relatively high proportion in children, and infections (Gradenigo syndrome: triad of abducens nerve palsy, facial nerve palsy, and pain in the first branch of the trigeminal nerve due to petrous apicitis spreading from otitis media) are also seen. In pediatric abducens nerve palsy, urgent imaging diagnosis to investigate the cause is essential.
The prognosis of abducens nerve palsy varies greatly depending on the cause.
Peripheral circulatory disorder (ischemic): Spontaneous recovery is common, with improvement in an average of 2.5±1.3 months, and natural recovery can be expected around 6 months 4. The prognosis is relatively good, but continuous management of diabetes and hypertension is necessary.
Traumatic: Because it is caused by traction or rupture in the intracranial course, recovery may be difficult in some cases. Long-term follow-up is required, and if improvement is poor, surgery is considered after 6 months or more.
Neoplastic: Depends on the prognosis of the primary disease. The course of abducens nerve palsy is evaluated in parallel with the treatment effect of the tumor.
Children: Investigation of the cause is the highest priority. In pediatric cases, some reports indicate that tumors are the main cause, while others report that increased intracranial pressure and anti-GQ1b antibody syndrome are equally common, with distribution varying by facility and region 3,6. When caused by tumors such as glioma, treatment of the tumor determines the prognosis. When caused by infections (e.g., Gradenigo syndrome), improvement can be expected with treatment of the underlying infection. In a report by Merino et al., approximately one-third of cases resolved spontaneously, and botulinum toxin injection and surgical intervention were also effective 3.
Regardless of the cause, it is important to regularly evaluate eye position, diplopia, and Hess chart in parallel with treatment of the underlying disease, and to monitor the course of improvement.
Graham C, Gurnani B, Mohseni M. Abducens Nerve Palsy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Aug 24. PMID: 29489275. https://www.ncbi.nlm.nih.gov/books/NBK482177/
Kim HJ, Kim HJ, Choi JY, Yang HK, Hwang JM, Kim JS. Etiologic distribution of isolated abducens nerve palsy: Analysis of 807 patients and literature review. Eur J Neurol. 2023;30(8):2471-2480. PMID: 37154347. doi:10.1111/ene.15828
Merino P, Gómez de Liaño P, Caro Villalobo JM, Franco G, Gómez de Liaño R. Etiology and treatment of pediatric sixth nerve palsy. J AAPOS. 2010;14(6):502-505. PMID: 21168073. doi:10.1016/j.jaapos.2010.09.009
Erdal Y, Gunes T, Emre U. Isolated abducens nerve palsy: Comparison of microvascular and other causes. North Clin Istanb. 2022;9(4):353-357. PMID: 36276565.
Tamhankar MA, Biousse V, Ying GS, Prasad S, Subramanian PS, Lee MS, et al. Isolated third, fourth, and sixth cranial nerve palsies from presumed microvascular versus other causes: a prospective study. Ophthalmology. 2013;120(11):2264-2269. PMID: 23747163. doi:10.1016/j.ophtha.2013.04.009
Abu Hanna F, Jabaly-Habib H, Halachmi-Eyal O, Hujierat M, Sakran W, Spiegel R. Sixth Nerve Palsy in Children: Etiology, Long-Term Course, and a Diagnostic Algorithm. J Child Neurol. 2022;37(4):281-287. PMID: 34879720. doi:10.1177/08830738211035912
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.