Esotropia is a condition in which one eye deviates inward (toward the nose) while the other eye fixates on a target. It is classified by onset age, presence of accommodation, variability of the deviation angle, and magnitude of the deviation.
Esotropia with onset within 6 months of age is classified as infantile esotropia (also called congenital esotropia). Among acquired esotropia after 6 months, accommodative esotropia involving accommodation is most common, followed by acute acquired comitant esotropia (AACE), intermittent myopic comitant esotropia (IMCE), cyclic esotropia, and secondary esotropia. It accounts for about one-third of all strabismus patients, with a prevalence estimated at 1–2% of the population.
Infantile esotropia: Onset within 6 months of age. Large-angle esotropia ≥30Δ. Reported in about 25 per 10,000 births, no gender difference.
Refractive accommodative esotropia: Orthotropic with full hyperopic correction. Normal AC/A ratio. Accounts for the majority of acquired esotropia.
Non-refractive accommodative esotropia: High AC/A ratio (≥6 PD/D). Difference in esotropia angle between near and distance ≥10 PD.
Partially accommodative esotropia: Residual deviation of 10 PD or more after full correction. Mixed accommodative and non-accommodative type. Poor binocular vision.
Acute acquired comitant esotropia (AACE): Older children and adults. Burian classification subdivides into 7 types2).
Intermittent myopic comitant esotropia (IMCE): Gradual onset with myopia. Characterized by shortened distance between medial rectus insertion and corneal limbus6).
Cyclic esotropia (alternate-day esotropia): Onset around 3–4 years of age. Alternating good and bad eye alignment in approximately 48-hour cycles.
Secondary esotropia: Consecutive esotropia after exotropia surgery (postoperative esotropia), sensory esotropia (visual acuity ≤0.2 with inability to fuse).
Infantile esotropia
Onset: Within the first 6 months of life. Large angle ≥30 PD.
Complications: DVD 46–90%, IOOA 33–78%, LN 30–50%.
Treatment: Surgery (bilateral medial rectus recession) is standard. Very early surgery (≤8 months) is most favorable for stereopsis.
Accommodative esotropia
Onset: Most common subtype of acquired esotropia. Often at 2–3 years of age. Main cause is hyperopia ≥+2 D.
3 types: Refractive (orthophoric with glasses), non-refractive (high AC/A ratio), partially accommodative (residual deviation with glasses).
Treatment: Full correction glasses are first-line. Only partially accommodative type is surgical indication.
QHow do you differentiate infantile esotropia from accommodative esotropia?
A
Infantile esotropia is characterized by onset within 6 months of age and large angle ≥30 PD. Accommodative esotropia is evaluated by wearing full hyperopic correction glasses for at least 3 months. In refractive accommodative esotropia, the deviation decreases by ≥10 PD and residual deviation is <10 PD. Even in infants under 1 year, if hyperopia >+2 D, trial of glasses can aid differentiation. Note that accommodative esotropia can also occur before 1 year of age, and cycloplegic refraction and glasses trial are essential for differentiation from infantile esotropia.
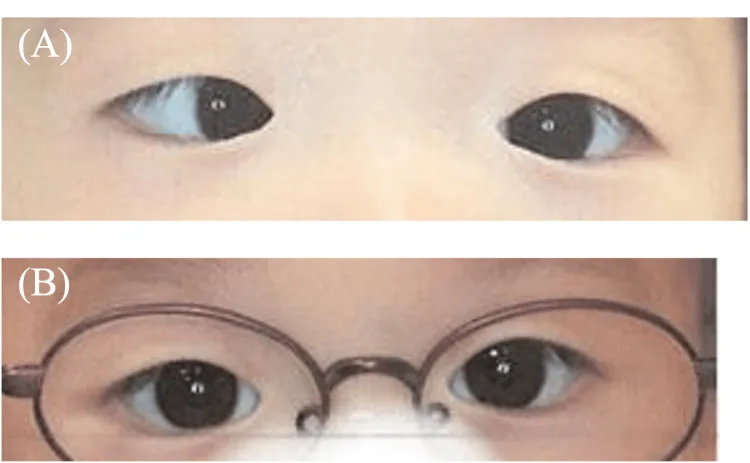
Fuseya K, et al. Esotropia Missed During Pre-health Checkup Screening With the Spot Vision Screener: A Case Series. Cureus. 2026. Figure 3. PMCID: PMC13045761. License: CC BY.
Binocular photographs of a child; in the upper row, one eye is deviated toward the nose, confirming esotropia. This image directly shows abnormal eye alignment and is suitable for illustrating key clinical findings.
Diplopia: Noticed in acute onset cases in adults and older children. Young children often do not complain of double vision because they learn suppression.
Suppression and Amblyopia Risk: Persistent suppression of one eye can lead to strabismic amblyopia.
Large-angle esotropia is the main finding, and several associated findings frequently coexist.
Main Findings in Infantile Esotropia
Large-Angle Deviation: Esotropia of 30 prism diopters or more. The angle of strabismus rarely fluctuates but may increase.
Cross Fixation: The right eye fixates in the left visual field and the left eye in the right visual field. This may appear as abduction limitation.
Amblyopia: Occurs in about 40–50% of cases. Determined by fixation preference. If there is no alternating fixation and a preference exists, the risk of amblyopia is high.
Associated Findings in Infantile Esotropia
Dissociated vertical deviation (DVD): Complicated in 46–90% of cases. The non-fixating eye elevates during occlusion. Usually appears after 1–2 years of age.
Inferior oblique overaction (IOOA): Complicated in 33–78% of cases. Observed as elevation during adduction.
Latent nystagmus (LN): Complicated in 30–50% of cases. Horizontal jerk nystagmus induced by monocular occlusion. The fast phase beats toward the non-occluded eye.
OKN asymmetry: Asymmetry where pursuit in the ear-to-nose direction is sustained and dominant.
Refractive: Esotropia angle decreases by ≥10 PD with full hyperopic correction, residual <10 PD. Esotropia angle 20–40 PD. AC/A ratio normal.
Non-refractive (high AC/A ratio): Near esotropia angle > distance by ≥10 PD. Near esotropia improves with +3 D lens loading. Gradient AC/A ratio exceeds normal 4±2 PD/D (≥6 PD/D).
Partially accommodative: Residual esotropia ≥10 PD even with full hyperopic correction. Binocular visual function generally poor.
AACE cases are characterized by acute-onset diplopia and esotropia, and up to 10% have underlying intracranial disease 2). In IMCE cases, shortening of the distance between the medial rectus insertion and the corneal limbus (5.2–5.3 mm) has been confirmed 6).
Risk factors for infantile esotropia: Prematurity, hydrocephalus, cerebral palsy, epilepsy, developmental delay, family history of strabismus, low birth weight. Cause unknown.
High AC/A ratio (cause of non-refractive type): Convergence response per unit of accommodation is excessive. Marked inward deviation at near.
AACE triggers: Monocular occlusion, trauma, fever, psychological stress. Induction of AACE by excessive near work during the COVID-19 pandemic has also been reported 2).
Excessive use of digital devices: Use of smartphones for 6 hours or more per day has been associated with IMCE6)
Causes of sensory esotropia: When visual acuity is 0.2 or less, fusion becomes difficult and inward deviation occurs
QCan using a smartphone cause esotropia?
A
Excessive near work using a smartphone for 6 hours or more per day has been reported to be associated with IMCE (Intermittent Myopic Consecutive Esotropia) and AACE (Acute Acquired Comitant Esotropia)2, 6). It has been hypothesized that excessive near fixation causes shortening of the medial rectus muscle and anterior displacement of its insertion.
For esotropia, cycloplegia with atropine sulfate eye drops is the first choice (0.5% 2-3 times daily for 5-7 days). It is excellent for detecting the maximum hyperopic refractive error. A mixture of cyclopentolate 1% and phenylephrine 2.5% may be used as an alternative. After full correction under cycloplegia, the eye position is measured to determine the amount of surgery.
Spectacle correction: If hyperopia of +2 D or more is present, the accommodative component should be evaluated with full correction spectacles. For hyperopia of +3 D or more, measure the ocular deviation after full correction under cycloplegia to determine the surgical dose. Since accommodative esotropia develops postoperatively in about 60% of cases, ongoing refractive management is necessary.
Surgical treatment:
The basic surgical procedure is bilateral medial rectus muscle recession. For large angles, lateral rectus muscle resection is added (three-muscle surgery) 1). Esotropia of 40 PD or more does not resolve spontaneously, so surgical indication should be determined promptly. In the PEDIG study, among infants confirmed to have 40 PD or more at 2–4 months of age, spontaneous resolution occurred in 0/45 cases and 0/21 cases 1).
Guidelines for surgical dosage (esotropia angle and recession amount):
Esotropia angle (Δ)
Recession amount from muscle insertion (mm)
Recession amount from limbus (mm)
15
3.0
—
25
4.0
8.5
35
5.0
9.5
45
6.0
10.5
55+
7.0
11.5
Maximum recession by age (from corneal limbus): <6 months → 10.0 mm, <1 year → 10.5 mm, <24 months → 11.0 mm.
p<0.001 (ultra-early vs late). Birch & Stager (2000) reported 100% stereopsis with surgery before 6 months, and 8% with surgery after 18 months.
Postoperative alignment goal: The minimum requirement for ARC to develop is to achieve microtropia within 8Δ or monofixation syndrome within 10Δ. Residual deviation ≥8Δ after surgery → use of membrane prism. Manifestation of DVD or oblique muscle dysfunction → appropriate reoperation. Reoperation rate is 15–30%1).
Ciancia syndrome: Characterized by large-angle esotropia >60°, abduction limitation, adduction fixation, and face turn. Set the recession amount larger than usual.
QWhen is the best time to perform surgery for infantile esotropia?
A
Ultra-early surgery before 8 months of age is considered most advantageous for achieving fusion (near fusion 93.8%) and stereopsis (75.0%). Early surgery by 2 years of age can also be expected to yield good results. Large-angle esotropia of 40Δ or more does not resolve spontaneously, so it is important to consult a pediatric ophthalmologist early to determine surgical indication1).
QIs reoperation sometimes necessary after surgery?
A
In infantile esotropia, the reoperation rate is reported to be 15–30%1). If DVD or oblique muscle dysfunction becomes manifest postoperatively, additional surgery is considered as appropriate. Residual esotropia (≥8Δ) is managed with membrane prism. Long-term management into adulthood is required; the success rate is about 80% after the first surgery and exceeds 95% including reoperations8).
Refractive accommodative esotropia: Full hyperopic correction with glasses is the first choice, and surgery is not required. Ocular alignment stabilizes within 3 months of wearing glasses. Only about 15% eventually become glasses-free. Since hyperopic power peaks around 6–7 years of age, regular cycloplegic refraction is necessary. Full-time wear is essential, and care must be taken to prevent the glasses frame from slipping down.
Non-refractive accommodative esotropia: Prescribe bifocal lenses with +2.5 to +3.0D addition or progressive addition lenses. Around 8–12 years of age, 37–62.5% can switch from bifocal to single vision lenses. Cholinesterase inhibitor distigmine bromide eye drops (Ubretid 1%) may be effective in reducing the AC/A ratio.
Partially accommodative esotropia: If 10PD or more remains under full correction with glasses, surgery is indicated. Surgery is performed only for the angle measured with glasses. About 30% require surgery. In children under 7 years, repeat cycloplegic refraction before surgery to confirm no undercorrection due to increased hyperopia. Surgical procedures include bilateral medial rectus recession, unilateral recession-resection, and posterior fixation suture (Faden procedure: effective for high AC/A ratio).
QCan accommodative esotropia be cured with glasses alone?
A
Refractive accommodative esotropia can achieve orthophoria with full hyperopic correction glasses alone. However, only about 15% eventually become glasses-free, and most require continued wear. In partially accommodative esotropia, glasses alone are insufficient, and surgery is needed for the residual deviation.
Acute esotropia: If the cause is unknown, observe for several months → reduce diplopia with membrane prism → surgery after stability for 6 months or more 2). Conservative treatment (glasses, prism, patch, botulinum) → surgery (unilateral recession-resection or bilateral medial rectus recession)
Cyclic esotropia: Medial rectus recession for the esotropic angle during the esotropic phase → good postoperative alignment maintained
Secondary esotropia: Postoperative esotropia (common after exotropia surgery), sensory esotropia (visual acuity ≤ 0.2), each managed accordingly
IMCE: Bilateral medial rectus recession of 5.5 mm (Parks method +0.5 mm augmentation) results in postoperative orthophoria and recovery of 40 seconds of stereopsis6)
In Japan, type A botulinum toxin (Botox®) was approved for strabismus treatment in 2015 (insurance coverage for ages 12 and older) 9). In the four years after approval, approximately 1,500 procedures were performed 9). Physician requirements: Board-certified ophthalmologist by the Japanese Ophthalmological Society + completion of training course + experience in 50 or more muscle surgeries 9).
Injection into the medial rectus for acute sixth nerve palsy in children (recommended dose 2.5–5 units per muscle) has been reported to improve from 50 PD to 20 PD in one week and to orthophoria in eight weeks 7). In infantile esotropia, it is more effective for deviation angles less than 30–35Δ 1). Safety has not been established for strabismus over 50 PD, restrictive strabismus, or Duane syndrome with lateral rectus weakness.
Hyperopia (+2D or more) requires accommodation to focus a clear image on the fovea, and increased accommodation leads to increased accommodative convergence. Normally, fusional divergence compensates for this convergence, but when it exceeds the compensatory ability, esotropia becomes manifest. In refractive type, the AC/A ratio is normal (4±2PD/D) but the amount of accommodation is excessive. In non-refractive type (high AC/A ratio), the AC/A ratio reaches ≥6PD/D, and convergence associated with accommodation at near becomes excessive, resulting in marked esotropia at near.
Age-related changes in hyperopia are also important. Newborns have about +2D of hyperopia, and hyperopia tends to increase until around 7–8 years of age. This increase and decrease affect the onset and course of accommodative esotropia.
Worth theory (congenital visual system defect → failure of binocular vision)
Chavasse theory (primary ocular motor abnormality precedes → rationale for very early surgery)
Guyton theory (convergence inhibition of fusion maldevelopment nystagmus → medial rectus shortening)
Brodsky theory (decompensation of subcortical motor pathways)
Richards (2007) reported that when esotropia persists for more than 6 months, monocular connections increase threefold compared to binocular connections 1). In primate models, early eye alignment restored normal eye movements and binocular vision, while delayed correction resulted in residual esotropia, LN, DVD, and OKN asymmetry 1).
Infantile nystagmus suppressed by convergence → excessive convergence → esotropia. ENG shows decelerating slow-phase waveform
IMCE
Sustained near gaze → shortening of medial rectus, anterior displacement of insertion. Pathological reports of lateral rectus atrophy exist 6)
AACE type V
Posterior fossa lesion → compression of cranial nerve VI 2)
Mechanism of amblyopia: In constant esotropia, the image from the deviated eye is suppressed in the cerebral cortex. When fixation is consistently with one eye, sustained suppression of the non-dominant eye leads to strabismic amblyopia. If alternating fixation occurs, both eyes develop equally.
Surgery before 11 months → normal mVEP vs 11-18 months → abnormal mVEP persists
Drover 20081)
Postoperative improvement in sensorimotor and gross motor development confirmed
Ghobrial & Kuwera (2023) reported improvement after asymmetric recession-shortening surgery in a case of bilateral horizontal gaze palsy and esotropia following neurocysticercosis3). When preoperative differentiation between gaze palsy and abducens nerve palsy is difficult, recess-resect surgery is recommended.
Negishi et al. (2024) reported esotropia surgery in nanophthalmos (axial length 15.5 mm)5). With a 6 mm medial rectus recession, the expected correction of 25 PD was only 12 PD, suggesting the influence of biomechanical peculiarities and pulley effects in small eyes.
The increase in AACE and IMCE due to excessive digital device use has recently gained attention, and the public health significance of limiting near work is being discussed2, 6). New approaches to improve binocular vision (binocular treatment: dichoptic stimulation to draw attention to the amblyopic eye) are being developed for strabismic amblyopia4). In adults with accommodative esotropia, LASIK/PRK to correct hyperopia and eliminate glasses has been attempted, but its application in children is not established. The success rate of surgery in adults is about 80% for the first surgery and over 95% including reoperations8).
Manjushree Bhate, Maree Flaherty, Frank J Martin. Timing of surgery in essential infantile esotropia – What more do we know since the turn of the century?. Indian Journal of Ophthalmology. 2022;70(2):386-395. doi:10.4103/ijo.ijo_1129_21.
Dragomir MS, Merticariu M, Merticariu CI. Management of acute acquired comitant esotropia in children. Romanian journal of ophthalmology. 2023;67(1):87-91. doi:10.22336/rjo.2023.16. PMID:37089805; PMCID:PMC10117196.
Ghobrial M, Kuwera E. A case of bilateral horizontal gaze palsy and concurrent esotropia. American journal of ophthalmology case reports. 2023;32:101947. doi:10.1016/j.ajoc.2023.101947. PMID:37954058; PMCID:PMC10637873.
Meier K, Tarczy-Hornoch K. Amblyopia and strabismus. Annu Rev Vis Sci. 2024;10:325-348.
Negishi T, Nakao S.. Surgery for Esotropia in a Case of Nanophthalmos. Cureus. 2024;16(7):e63728. doi:10.7759/cureus.63728. PMID:39099983; PMCID:PMC11295114.
Tangtammaruk P, Hieda O.. Insidious Myopic Comitant Esotropia in a Teenager. Int Med Case Rep J. 2024;17:945-948. doi:10.2147/imcrj.s488472. PMID:39554901; PMCID:PMC11566586.
Merticariu CI, Merticariu M, Dragomir MS.. Botulinum Toxin Injection in Acute Sixth Nerve Palsy in a 1-Year-Old Child: Case Report, Management Strategy, and Review of Literature. Rom J Ophthalmol. 2025;69(1):22-27. doi:10.22336/rjo.2025.05. PMID:40330958; PMCID:PMC12049660.