When residual strabismus remains after non-surgical treatments (refractive correction, amblyopia training, prism therapy, orthoptic training), surgical correction of eye position is performed. The surgical plan (eye to be operated on, procedure, and amount) is determined by the type of strabismus and ocular motility abnormality, and weakening/strengthening procedures or muscle transposition are performed on the extraocular muscles.
Procedures are broadly classified into three types.
Procedure
Purpose
Typical Use
Recession
Weakening of the muscle
Medial rectus recession for esotropia, lateral rectus recession for exotropia
Resection
Strengthening of the muscle
Medial rectus resection for exotropia, lateral rectus resection for esotropia
Transposition
Changing the direction of muscle action
Paralytic strabismus, special type strabismus, after muscle loss
The overall success rate of adult strabismus surgery is about 80% after a single surgery, and over 95% when including a second surgery 1). Persistent postoperative diplopia (intractable in primary gaze) occurs in less than 1% of cases 1). Surgical goals include improving eye alignment, restoring binocular vision, reducing diplopia, eliminating compensatory head posture, and achieving psychosocial improvement 1).
Surgery is performed for residual strabismus that does not achieve sufficient improvement with non-invasive treatments such as glasses, prisms, or amblyopia training. The purpose of surgery is to correct eye alignment, restore and maintain binocular vision, and achieve cosmetic improvement. In adults, good alignment is achieved in about 80% after the first surgery and over 95% when including a second surgery 1).
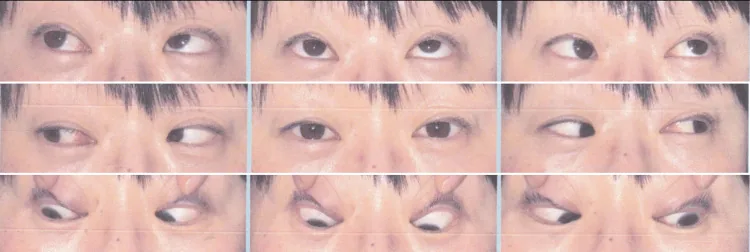
Simpao JL, et al. Surgical Approaches for Residual Secondary Gaze Diplopia After Strabismus Surgery: A Case Series. Cureus. 2025. Figure 5. PMCID: PMC12662713. License: CC BY.
Clinical photograph taken in nine gaze directions, showing limited elevation of the right eye and eye misalignment that varies with gaze direction. Ocular motor abnormalities of strabismus are demonstrated.
The prevalence of adult strabismus is 2.7% of ophthalmology outpatient visits according to IRIS Registry data, with an estimated incidence of about 4%1). The frequency of strabismus is 2–4% of the population (varies by race). Esotropia is more common in Western Caucasians, while exotropia is more common in Asians and Blacks. Incomitant strabismus accounts for about 5% of all strabismus. Infantile esotropia occurs at a frequency of 1–2%. The reoperation rate is generally 20–30%.
Forced duction test: Essential before surgery for incomitant strabismus. In children, it is performed under general anesthesia immediately before surgery.
Prism adaptation test: Performed in older children. It allows sensory evaluation and improves accuracy of surgical technique and amount.
Imaging tests: For vertical strabismus and special types, orbital MRI/CT is used to detect congenital extraocular muscle abnormalities.
Eye position tests: Measure the strabismus angle at distance (5 m) and near (30 cm) in 9 gaze positions. In patients with fusion, perform a 30-45 minute occlusion test to reveal the full deviation before measurement 1).
The Lancaster red-green test and Hess screen test are efficient 1). For quantifying diplopia, use Goldmann perimetry plotting, cervical range of motion measurement, and the Diplopia Questionnaire 1).
Scleral perforation: Confirm with dilated fundus examination
Lost muscle: Identify muscle location with saccadic velocity, forced duction test, and CT/MRI
Anterior segment ischemia: Diagnose based on findings of corneal edema, Descemet membrane folds, and moderate mydriasis
QWhat tests are needed before strabismus surgery?
A
Quantify the strabismus angle with 9-gaze position testing (distance and near), and evaluate suppression, stereopsis, and retinal correspondence with binocular vision tests. For incomitant strabismus, a forced duction test is essential; in children, it is performed just before surgery under general anesthesia. In older children, perform a prism adaptation test to improve surgical accuracy. For vertical strabismus and special types, use orbital MRI/CT to detect extraocular muscle abnormalities.
In intermittent exotropia, binocular vision is maintained, so early surgery is unnecessary. Observe with refractive correction and amblyopia training, and perform surgery when it progresses to constant exotropia. If the deviation angle is less than 20Δ, surgery is not indicated; try optical treatment or orthoptic training. If the deviation angle is large and frequent, or if it is a cosmetic concern, plan surgical treatment before school age.
In strabismus where binocular vision is maintained with an abnormal head posture, early surgery is unnecessary if the deviation angle is small. Observe with refractive correction and prism therapy, and plan surgical treatment by school age at the latest.
If there is visual impairment due to organic disease, achieving binocular vision through eye alignment correction is difficult, but if it is a cosmetic concern, plan surgical treatment around age 6. Generally, a deviation angle exceeding 15Δ affects cosmesis, but consider surgery if the deviation is 20Δ or more and the patient/family desires it. Since childhood esotropia tends to shift to exotropia postoperatively, perform undercorrection surgery.
Move the insertion of the extraocular muscle posteriorly to increase its effective length and weaken it. Typical indications include medial rectus recession for esotropia and lateral rectus recession for exotropia. Maximum correction effect is obtained in the direction of action of the recessed muscle.
Resect a portion of the extraocular muscle to shorten and strengthen it. Typical indications include medial rectus resection for exotropia and lateral rectus resection for esotropia.
The extraocular muscle attachment is moved to a different position to change the direction of action. Used for paralytic strabismus and special types of strabismus. Also selected when the muscle is lost and cannot be retrieved.
A technique that allows postoperative readjustment of the extraocular muscle position to modify the surgical effect. Based on the hang-back recession, the muscle tendon is detached from its insertion and a suture is passed through the sclera at the original insertion. A sliding knot is created with another suture (6/0 Vicryl), and postoperatively, under topical anesthesia, the knot position is adjusted while performing an alternate cover test to fine-tune the eye alignment. Once the desired correction is achieved, the hang-back suture is tied and the excess suture is trimmed.
This technique is particularly useful in reoperations and cases where postoperative alignment is difficult to predict, such as restrictive or paralytic strabismus1).
Bow-tie method
Origin: The first adjustable suture technique devised by Jampolsky (1975).
Technique: A knot is created to fix the muscle to the sclera at the insertion and set the hang-back amount, and a bow-tie knot is placed on top of it.
Adjustment: The bow-tie knot is untied to change the surgical amount.
Sliding noose method
Principle: A method in which the muscle is held by a separate knot from the muscle suture.
Adjustment: Advancing the noose toward the muscle decreases the recession amount, and moving it away increases it.
Features: Fine adjustment of the surgical amount is possible through sliding manipulation.
Short-tag noose method
Advantage: Since the conjunctiva completely covers the surgical site, no additional manipulation is needed if adjustment is not required.
Application in children: Delayed adjustment is also possible. It is easier to avoid a second general anesthesia.
Feature: It has been reported that adjustment is possible with only topical anesthesia in 89% of children.
Removable Noose Technique
Devised by: Guyton. Combines a clove hitch with three slip knots.
Advantage: The noose suture material can be completely removed after adjustment, leaving no foreign material under the conjunctiva.
In addition to rectus recession, it is also applied to special procedures such as rectus transposition, Harada-Ito procedure, and superior oblique tendon surgery 1). In inferior rectus recession, a semi-adjustable suture technique may reduce muscle drift. Since overcorrection in downgaze is poorly tolerated, it is recommended to aim for slight undercorrection and use adjustable sutures 1).
The timing of adjustment is immediately to several hours after surgery. By the next day, the tendon adheres to the sclera, making adjustment difficult. In thyroid eye disease, some surgeons claim better results, but there are concerns about late overcorrection and muscle slippage 1).
Botulinum toxin injection into extraocular muscles is used alone or in combination with surgery 1). It is used to enhance the effect of surgery for new or large deviations, for residual postoperative deviations, and for small-angle deviations 1). It is also useful for preventing contracture of the antagonist muscle while waiting for spontaneous recovery in paralytic strabismus1).
Even small deviations of ≤8Δ horizontally and <3Δ vertically can cause diplopia and asthenopia 1). They can be managed with tenotomy (partial central tenotomy) or single rectus recession 1).
The estimated incidence of serious complications (scleral perforation, severe infection, muscle slippage/loss, scleritis) is 1/400, of which poor prognosis is reported in 1/2,400 2). Many complications are minor and resolve spontaneously or improve with topical medications 9).
Intraoperative Complications
Scleral perforation: Incidence 0.08–5.1%. Most cases have no sequelae 2)5)
Oculocardiac reflex: Incidence 67.9%. Sinus bradycardia is most common. Cardiac arrest 0.11% 6)7)
Scleral perforation: Dilated fundus examination → laser photocoagulation for retinal tears. In children, often no treatment is needed. For thin sclera, choose the hang-loose technique.
Oculocardiac reflex: Usually resolves with cessation of manipulation. If frequent, administer intravenous atropine sulfate.
Lost muscle: Attempt immediate retrieval during the same surgery. The lateral rectus and inferior rectus can be found via connective tissue attachments to adjacent muscles. The medial rectus has no such attachments and is difficult to secure. If retrieval fails, perform muscle transposition.
Slipped muscle: Trace the fascia posteriorly to locate the muscle and reattach it.
Even if strabismus in children is successfully treated, it may change due to growth, aging, and environmental factors. Long-term management of eye alignment and binocular vision is important. It takes 3 to 4 months for the muscle suture site to stabilize. Choosing an initial surgical technique that allows easy reoperation is also important.
QIs reoperation sometimes necessary after strabismus surgery?
A
The reoperation rate varies by disease but is generally 20-30%. Childhood esotropia tends to shift to exotropia postoperatively, so undercorrection is often performed, and the initial surgery is chosen to facilitate reoperation. In adults, good alignment is achieved in about 80% after the first surgery and over 95% including a second surgery 1).
QIs adjustable suture necessary for all strabismus surgeries?
A
Adjustable sutures are particularly useful in cases where postoperative alignment is difficult to predict, such as reoperations, restrictive strabismus, and paralytic strabismus1). In simple concomitant strabismus, non-adjustable sutures often yield good results.
When strabismus occurs in infancy, it leads to suppression, amblyopia, and abnormal correspondence in the deviating eye, preventing normal binocular vision development.
Sensitive period for stereopsis development: 2 months to 2 years of age, peak at 3-4 months of age
Peripheral fusion acquisition: Surgery required within 2 years of age
Gross stereopsis: Surgery required within 1 year of age
Fine stereopsis: Ultra-early surgery required within 6 months of age
Lost muscle: Muscle tendon slips off the suture/instrument and retracts posteriorly into the orbit. The medial rectus is difficult to retrieve due to lack of connections with other muscles.
Slipped muscle: Only the superficial fascia is fixated → muscle belly retracts during contraction → presents as clinical muscle weakening
Anterior segment ischemia: Anterior ciliary arteries run within the rectus muscles → simultaneous surgery on multiple rectus muscles causes blood flow impairment
Stretched scar: Suture site elongation → posterior displacement of muscle belly → reduced action
Iatrogenic Brown syndrome: Limitation of elevation in adduction occurs after superior oblique tuck procedure. It can be prevented by performing intraoperative superior oblique traction test to determine the amount of tuck.
Conjunctival inclusion cyst: Conjunctival epithelium becomes buried subconjunctivally during surgery and forms a cyst.
Corneal dellen: Postoperative ocular surface irregularity → abnormal tear film distribution → corneal thinning
It takes 3 to 4 months for the muscle suture site to stabilize. During this period, adhesion between the muscle and sclera progresses, and the final ocular alignment is determined. The immediate postoperative alignment does not always match the long-term alignment, and this unpredictability is the rationale for adjustable sutures. In children, Tenon’s capsule is thick and requires adequate management; since surgery is performed under general anesthesia, a second anesthesia exposure for adjustment can be a concern. The short-tag noose technique can avoid a second anesthesia when adjustment is not needed.
Current evidence on the effectiveness of adjustable sutures is not conclusive. In an RCT involving 40 adults with intermittent exotropia, the success rate was 90% in the adjustable group vs. 85% in the non-adjustable group, with no statistically significant difference (p=0.3). In a review of 11 studies, only 3 out of 7 studies showed a significant difference, and all 3 studies that showed significance were large-scale studies with n≥100. When reoperation rate was used as an indicator, 4 out of 5 studies showed a significant difference. An RCT of 60 children with horizontal strabismus found no significant difference in success rate at 6 months postoperatively (success defined as residual deviation ≤8Δ).
Discussion of adjustable sutures in thyroid eye disease
Some surgeons claim better outcomes, but others do not use them due to concerns about late overcorrection and muscle slippage 1). Alternative techniques such as polyester permanent sutures and relaxed muscle positioning technique are being investigated.
A 2025 retrospective study reported that postoperative antibiotic eye drops did not reduce infection rates. Further investigation is needed regarding the necessity of antibiotic eye drops for postoperative infection prevention.
Chemical denervation via botulinum toxin injection has been reported effective for strabismus correction in some cases. Research is progressing as an alternative to surgery. A Cochrane systematic review noted limited RCTs, making evaluation difficult1).
Using ketamine as the main anesthetic has been reported to reduce the oculocardiac reflex, postoperative nausea and vomiting, and postoperative agitation. Improved anesthesia management is expected to lower complication risks.
American Academy of Ophthalmology. Adult Strabismus Preferred Practice Pattern. San Francisco: AAO; 2023.
Bradbury JA, Taylor RH. Severe complications of strabismus surgery. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2013;17(1):59-63. doi:10.1016/j.jaapos.2012.10.016. PMID:23352718.
Tessler HH, Urist MJ. Corneal dellen in the limbal approach to rectus muscle surgery. The British journal of ophthalmology. 1975;59(7):377-9. doi:10.1136/bjo.59.7.377. PMID:1103964; PMCID:PMC1042643.
Fresina M, Campos EC. Corneal ‘dellen’ as a complication of strabismus surgery. Eye (London, England). 2009;23(1):161-3. doi:10.1038/sj.eye.6702944. PMID:17676020.
Simon JW, Lininger LL, Scheraga JL. Recognized scleral perforation during eye muscle surgery. J Pediatr Ophthalmol Strabismus. 1992;29:273-275.
Apt L, Isenberg S, Gaffney WL. The oculocardiac reflex in strabismus surgery. Am J Ophthalmol. 1973;76:533-536.
Min SW, Hwang JM. The incidence of asystole in patients undergoing strabismus surgery. Eye (London, England). 2009;23(4):864-6. doi:10.1038/eye.2008.127. PMID:18483497.
Shen E, Porco T, Rutar T. Errors in strabismus surgery. JAMA Ophthalmol. 2013;131:75-79.
Wan MJ, Hunter DG. Complications of strabismus surgery: incidence and risk factors. Seminars in ophthalmology. 2014;29(5-6):421-8. doi:10.3109/08820538.2014.959190. PMID:25325869.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.