Vertical strabismus is a general term for vertical misalignment of the eyes, where one eye deviates upward or downward compared to the other. It is classified based on whether the deviation is constant or intermittent, and congenital or acquired. Most vertical strabismus is comitant, but incomitant types due to myogenic or neurogenic causes are also important.
Congenital superior oblique palsy (SOP) is the most common cause of vertical strabismus in children. The superior oblique muscle originates deep in the orbit, changes its course by approximately 180° at the trochlea, and attaches broadly to the sclera on the temporal side of the superior rectus muscle. The posterior fibers act to depress the eye in adduction and abduct, while the anterior fibers produce intorsion. In superior oblique palsy, the affected eye shows elevation, inward deviation, and extorsion, and the patient compensates by tilting the head to the healthy side.
The annual incidence of superior oblique palsy is 6.3 per 100,000 population, with a male predominance1). Head trauma (including concussion) is the most common identifiable cause2), followed by cerebrovascular disorders, tumors, and idiopathic causes. In a study of 1,000 cases of cranial nerve palsy, trauma, congenital, vascular disorders, and tumors were the main causes of fourth nerve palsy4).
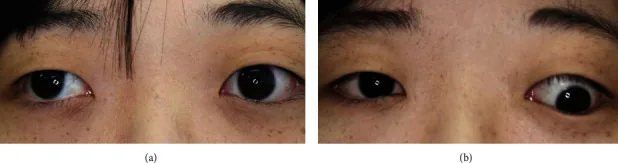
Aomatsu K, et al. Isolated Superior Oblique Muscle Swelling Causing Acute Vertical Strabismus in Graves’ Disease. Case Rep Ophthalmol Med. 2020. Figure 4. PMCID: PMC7652624. License: CC BY.
Two clinical photographs show the difference in eye position under different fixation conditions. In the right image, the vertical deviation is clearly visible, demonstrating the eye position findings of vertical strabismus.
Chief complaint: In children, head tilt (ocular torticollis) is often the first symptom. Diplopia is rare, but may appear for the first time in adulthood as decompensation.
Features: Low frequency of amblyopia and poor binocular vision (compensated by abnormal head posture to maintain single vision). Long-term untreated abnormal head posture may lead to facial asymmetry (difference in maxillary length) and risk of scoliosis4).
Brown Syndrome
Chief complaint: Limited elevation in adduction. Patients prefer chin-up head posture and turning the face toward the healthy side.
Features: Orthophoria or hypotropia in primary position. Some patients feel a click near the trochlea during elevation. A V-pattern with exotropia in upgaze is characteristic and useful for differentiation from inferior oblique palsy.
A-V Pattern Strabismus (Pattern Strabismus)
Features: Horizontal strabismus where the deviation angle differs significantly between upgaze and downgaze. Types A and V are most common. V-pattern exotropia has a larger angle in upgaze and smaller in downgaze. V-pattern esotropia has a smaller angle in upgaze and larger in downgaze. Infantile esotropia often coexists with overelevation in adduction and V-pattern strabismus.
Other Disease Types
Double elevator palsy (monocular elevation deficiency): Congenital. Ptosis is associated in 50% of cases. Bell’s phenomenon is preserved (differentiating from inferior rectus fibrosis).
Acquired superior oblique palsy: Head trauma or cerebrovascular disorder. Diplopia is the main complaint. No facial asymmetry.
Congenital fibrosis of the extraocular muscles (CFEOM): Type 1 (autosomal dominant, bilateral ptosis and fixed infraduction of the eyes), Type 2 (autosomal recessive, large-angle exotropia), Type 3 (autosomal dominant, variable restriction of eye movements).
Ocular torticollis consists of face turn, chin up/down, head tilt, or a combination of these. If the abnormal head posture disappears when one eye is covered, it can be identified as ocular torticollis compensating for diplopia. In trochlear nerve palsy, a characteristic abnormal head posture is seen: face turned toward the healthy side, chin down, and head tilted toward the healthy side.
QCan a child's head tilt be a sign of strabismus?
A
Head tilt (torticollis) in children is a typical initial symptom of congenital superior oblique palsy. If the head tilt disappears when one eye is covered, ocular torticollis is suspected. Differentiation from congenital muscular torticollis (mass or shortening of the sternocleidomastoid muscle) is important, and ocular alignment examination is key to diagnosis.
Congenital SOP: Congenital hypoplasia or abnormal insertion of the superior oblique tendon. In over 70% of cases, MRI confirms absence of the trochlear nerve. Hereditary cases are rare.
Acquired SOP: Head trauma (most common), cerebrovascular disease, tumor, idiopathic.
Brown syndrome: Congenital (congenital tendon sheath stenosis), inflammatory (including autoimmune diseases such as thyroid eye disease), traumatic (impact to the trochlea from frontal blow), iatrogenic (excessive superior oblique tuck surgery).
A-V pattern strabismus: Inferior oblique overaction (main cause of V pattern), superior oblique overaction (main cause of A pattern), orbital morphological abnormalities (craniosynostosis, Crouzon disease), superior oblique tendon anomalies.
This is a systematic diagnostic method to identify the causative muscle of hypertropia.
Step 1: Determine which eye is hypertropic (right or left hypertropia).
Step 2: Determine whether the hypertropia worsens on adduction or abduction (differentiating IOOA vs SOP).
Step 3: Bielschowsky head tilt test: if the hypertropia increases when the head is tilted toward the affected side, it indicates superior oblique palsy (SOP).
Quantification of cyclotorsion: Use Double Maddox Rod, Lancaster red-green test, or synoptophore (with fusion slides)4). Since the superior oblique muscle has an intorsion action, SOP causes excyclotorsion. Subjective cyclotorsion is smaller than objective cyclotorsion in long-standing SOP (due to adaptation)2)
Imaging (MRI): In congenital SOP, evaluate hypoplasia of the superior oblique tendon, abnormal insertion, and trochlear nerve deficiency. In A-V pattern strabismus, assessment of extraocular muscle position and shape is important.
Definitive diagnosis of Brown syndrome: Positive superior oblique traction test under general anesthesia. The degree of resistance varies by case.
“Masquerading SOP”: Cases with positive three-step test but no superior oblique atrophy on MRI. Inferior rectus enlargement in thyroid eye disease can mimic SOP 3).
Intraoperative testing: Intraoperative exaggerated forced duction test confirms superior oblique tendon laxity (congenital SOP) 4). Quantitative intraoperative rotational traction test is also useful.
QWhat is A-V pattern strabismus?
A
Horizontal strabismus in which the strabismus angle differs significantly between upgaze and downgaze. In V-pattern, exodeviation increases in upgaze (V shape); in A-pattern, esodeviation increases in upgaze (A shape). Inferior oblique overaction (main cause of V-pattern) or superior oblique overaction (main cause of A-pattern) are responsible, and oblique muscle surgery or vertical transposition of horizontal recti is performed.
After head trauma, observe for 6 months; if no spontaneous recovery, consider surgery 2)
Prism glasses: effective for small angles (less than 10 PD) and comitant deviations. Difficult to apply if there is variable outward or oblique deviation 2)
Congenital: tends to resolve spontaneously. Observation is the mainstay. Surgical indications: (1) hypotropia in primary position, (2) significant abnormal head posture, (3) cosmetic issue with depression on adduction
Inflammatory: improves with local injection of corticosteroids (at the trochlea)
Surgery: superior oblique tendon lengthening (tenotomy, silicone band lengthening, nonabsorbable suture lengthening). Beware of iatrogenic SOP (inverted Brown pattern) in long-term prognosis
When accompanied by oblique muscle overaction: combine oblique muscle surgery with horizontal strabismus surgery
V-pattern esotropia and V-pattern exotropia: bilateral inferior oblique weakening + horizontal muscle surgery (if alternating hypertropia is present, anterior transposition of inferior oblique)
A-pattern esotropia: superior oblique weakening + horizontal muscle surgery (if binocular vision is present in downgaze, beware of torsional diplopia)
When not accompanied by oblique muscle overaction: Trick method (vertical transposition of horizontal rectus insertions)
In V-pattern, move the medial rectus downward and the lateral rectus upward by half to one muscle belly width
QDoes congenital superior oblique palsy resolve on its own?
A
Congenital superior oblique palsy does not resolve spontaneously. Although amblyopia is infrequent due to compensatory abnormal head posture, long-term neglect carries risks of facial asymmetry and scoliosis. Surgery is recommended once the diagnosis is confirmed. Visual and binocular outcomes are generally good, but multiple surgeries may be required if anatomical abnormalities of the superior oblique are severe.
QIs surgery necessary for Brown syndrome?
A
Congenital Brown syndrome tends to resolve spontaneously, so observation is the basic approach. Surgical indications include: (1) hypotropia in primary position, (2) significant abnormal head posture, and (3) cosmetic issues with depression in adduction. Inflammatory cases may improve with local steroid injection.
The superior oblique muscle originates in the superonasal aspect of the deep orbit, runs forward, and then changes direction by approximately 180° at the cartilaginous trochlea on the medial orbital roof. After passing through the trochlea, it runs lateral to the superior rectus and attaches broadly in a fan shape to the sclera. The posterior fibers are responsible for depression and abduction in adduction, while the anterior fibers produce intorsion. Paralysis of the superior oblique results in elevation, inward deviation, and extorsion of the affected eye.
Most cases of congenital SOP show hypoplasia or abnormal insertion of the superior oblique tendon on MRI, and trochlear nerve absence is confirmed in over 70%. Dysfunction of the superior oblique leads to secondary overaction of the inferior oblique. In acquired SOP, the trochlear nerve is the only cranial nerve emerging from the dorsal brainstem and has the longest intracranial course, making it vulnerable to head trauma.
The essence is a mechanical problem preventing smooth passage of the superior oblique tendon through the trochlea. Congenital cases are caused by congenital stenosis of the tendon sheath, while inflammatory cases result from inflammatory thickening around the trochlea. It can also occur due to trauma to the trochlear region from frontal impact, excessive superior oblique tuck surgery (iatrogenic), or autoimmune diseases including thyroid eye disease.
The main cause of V-pattern strabismus is inferior oblique overaction (common in infantile esotropia), while A-pattern is often due to superior oblique overaction. Orbital morphological abnormalities (e.g., craniosynostosis, Crouzon disease) also contribute. Imaging evaluation of extraocular muscle position and shape is important for determining treatment strategy.
Congenital neurodevelopmental abnormalities cause the extraocular muscles to be replaced by fibrous tissue. Genetic abnormalities such as the KIF21A gene (type 1) and PHOX2A gene (type 2) have been identified.
Demer & Clark (2022) reported the concept of “Masquerading SOP,” where the Parks 3-step test is positive despite no superior oblique atrophy on MRI 3). It was shown that enlargement of the inferior rectus muscle in thyroid eye disease can mimic SOP, highlighting the importance of detailed orbital MRI evaluation.
Bata et al. (2017) reported that bilateral SO tendon advancement (using adjustable sutures) significantly improved both vertical and torsional deviations in patients with large-angle bilateral SOP 4).
Measurement methods for torsional deviation (Double Maddox Rod, Lancaster red-green, synoptophore) were compared, examining the agreement between methods and the characteristics of each 4). Standardization of measurement methods was shown to be important for clinical decision-making.
Congenital SOP ocular torticollis, if left untreated for a long time, has been reported to cause facial developmental asymmetry (difference in maxillary length) 4), and early surgical intervention may contribute to improvement in facial symmetry. With the spread of adjustable suture techniques, the success rate of primary surgery for acquired SOP and adult cases has improved 2), and accumulation of evidence through future multicenter studies is expected.
QIs there a risk of overcorrection in surgery for superior oblique palsy?
A
Overcorrection in downgaze is extremely poorly tolerated because it causes significant difficulty in reading and stair walking. The surgical goal is set at slight undercorrection (no diplopia in downgaze). It is recommended to use adjustable sutures and fix the suture after confirming the eye position postoperatively 2). For small angles (1-6 PD), partial tendon recession (pole recession) can reduce the risk of overcorrection 4).
Dosunmu EO, Hatt SR, Leske DA, et al. Incidence and etiology of presumed fourth cranial nerve palsy: A population-based study. Am J Ophthalmol. 2018;185:110-114.
American Academy of Ophthalmology Pediatric Ophthalmology/Strabismus Panel. Adult Strabismus Preferred Practice Pattern®. San Francisco: AAO; 2023.
Demer JL, Clark RA. Masquerading superior oblique palsy. Am J Ophthalmol. 2022;242:197-208.
Bata BM, Leske DA, Holmes JM. Adjustable bilateral superior oblique tendon advancement for bilateral fourth nerve palsy. Am J Ophthalmol. 2017;178:115-121.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.