Mild
Primary position: No vertical deviation
Adduction: No downshoot
Elevation: Limited only in adduction

Brown syndrome is a form of vertical strabismus in which elevation of the eye in adduction is limited or impossible due to an abnormality of the superior oblique tendon-trochlea complex. It is also called superior oblique tendon sheath syndrome. It was first reported in 1950 by Dr. Harold Whaley Brown 1).
The limitation of elevation in adduction is basically a mechanical problem caused by the superior oblique tendon not sliding smoothly through the trochlea, resulting in a condition where the tendon becomes stiff and cannot stretch like a tendon.
Epidemiology:
Genetics:
Autosomal recessive or autosomal dominant inheritance with reduced penetrance has been reported1).
Familial occurrence is relatively rare, affecting 1 in 20,000 births, and autosomal recessive or autosomal dominant inheritance with low penetrance has been reported1). Most cases are sporadic.
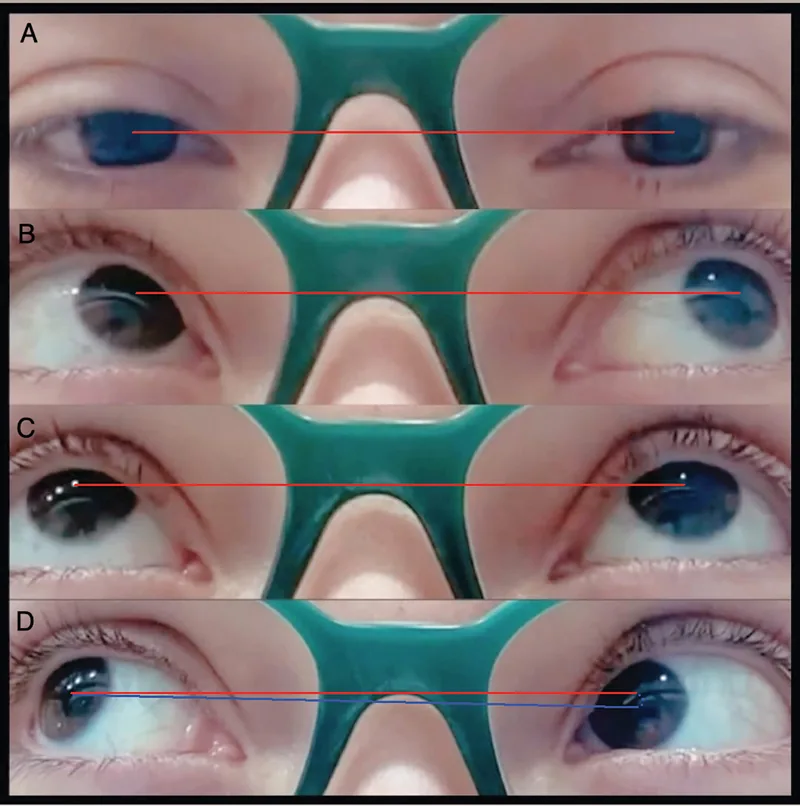
Limited elevation in adduction is the defining finding of Brown syndrome.
Mild
Primary position: No vertical deviation
Adduction: No downshoot
Elevation: Limited only in adduction
Moderate
Primary position: No vertical deviation
Adduction: Downshoot present
Elevation: Clearly limited in adduction
Severe
Primary position: Hypotropia present
Adduction: Downshoot present
Abnormal head posture: Marked head tilt and face turn
Other important clinical findings are shown below1).
Brown syndrome is broadly classified into congenital and acquired types.
The following table compares the causes.
| Classification | Main Causes |
|---|---|
| Congenital | Tendon shortening/loss of elasticity, trochlear malformation, fibrous bands |
| Acquired/Inflammatory | RA, juvenile idiopathic arthritis, SLE, post-COVID-19 trochleitis |
| Acquired/Traumatic/Iatrogenic | Orbital fracture/surgery, after scleral buckling surgery |
Congenital:
The basic cause is structural abnormality of the superior oblique tendon-trochlea complex 1). Shortening and loss of elasticity of the tendon, trochlear malformation, tendon nodules, and fibrosis are observed. A recent explanation proposes the presence of a fibrotic strand originating from the posterior part of the SO tendon to the trochlear area and having the same insertion 1). An association with congenital cranial dysinnervation disorders (CCDDs) has also been reported.
There is also a report that elongation of the ZT distance (distance from the annulus of Zinn to the trochlea) is associated with the development of BS. In 12 normal children, the average was 37.1±1 mm (range 35.8–38.7 mm), whereas in BS patients it was elongated to 41.2 mm 6).
Acquired:
Note that ocular myasthenia gravis has been newly reported to present with BS-like findings (AChR antibody positive) 3), and should be included in the differential diagnosis.
In both adults and children, the development of Brown syndrome due to trochleitis after COVID-19 infection has been reported 5)8). MRI shows swelling and gadolinium enhancement of the SO tendon sheath, and it improves with systemic corticosteroid administration. It can occur even in cases without multisystem inflammatory syndrome.
Diagnosis is a clinical diagnosis based on medical history and clinical findings1).
Main examination methods:
Imaging diagnosis:
Key points for differential diagnosis:
| Disease | FDT | Characteristic findings |
|---|---|---|
| Inferior oblique palsy | Negative | SO overaction, A-pattern strabismus |
| Double elevator palsy | Positive in both adduction and abduction | Elevation limitation in all directions |
| Orbital fracture | Positive in both adduction and abduction | History of trauma, infraorbital hypoesthesia |
| Myasthenia gravis | Negative (restrictive-like findings) | AChR antibody positive3) |
Obtaining a family history is also important to rule out familial Brown syndrome1).
In congenital Brown syndrome, observation is the first choice. Spontaneous improvement is seen in up to 75-80% of cases, and the basic policy is not to rush into surgery1).
Corticosteroids are effective for inflammatory acquired Brown syndrome.
Surgery is considered in the following cases1).
Tendon lengthening
Silicone expander method (Wright method): Marked improvement in 3 of 4 cases. The SO tendon is lengthened by 10 mm.
Z-plasty lengthening: Performed with Mersilene 5-0 suture in a case of sequential bilateral BS. If insufficient, conversion to complete tenotomy is performed 6).
The advantage is that the risk of iatrogenic superior oblique palsy can be reduced.
Tenectomy
SO tendon tenotomy/tenectomy: Most effective initial surgery in a retrospective study of 38 cases. AHP resolution rate 81.5% 1).
There is a risk of iatrogenic superior oblique palsy due to overcorrection. Careful postoperative monitoring is required.
Other surgical techniques
SO tendon split lengthening: Significant improvement in hypotropia and elevation limitation in 15 severe BS cases 1). Overcorrection in 2 of 20 cases (10%) in a retrospective study.
SO tendon thinning: Effective in 21 eyes with thickened SO tendon 1).
Revision surgery for iatrogenic BS: A case where the SO complex was released by repositioning titanium mesh after orbital fracture ORIF 4).
In congenital cases, spontaneous improvement is observed in up to 75–80%, so the basic approach is observation without rushing to surgery 1). In acquired idiopathic cases, complete remission is reported in 30%. However, in severe cases (hypotropia in primary position, significant abnormal head posture), surgical intervention is considered.
Iatrogenic superior oblique palsy can occur after SO tenotomy or resection. Tendon lengthening procedures (silicone expander technique, Z-tenotomy) are thought to reduce this risk, and lengthening procedures have been increasingly chosen in recent years 1). Careful postoperative follow-up is necessary.
Dysfunction of the superior oblique tendon–trochlea complex is the main mechanism of Brown syndrome 1).
Embryological background:
Sevel’s study showed that the superior oblique muscle, tendon, and trochlea develop from a common mesenchymal tissue 1). This finding explains the natural course of congenital BS, which gradually improves with growth. An association with congenital cranial dysinnervation disorders (CCDDs) has been proposed, but many cases do not show limitation of depression in adduction, so it cannot explain all cases 1).
Fibrotic strand hypothesis:
A recent hypothesis proposes the existence of a fibrotic strand originating from the posterior part of the SO tendon to the trochlear area and inserting at the same site as the SO tendon 1). Variations in insertion can explain not only typical elevation limitation in adduction but also atypical patterns of elevation impairment.
ZT distance elongation hypothesis:
Elongation of the ZT distance (distance from the annulus of Zinn to the trochlea) is proposed to cause anterior displacement of the trochlea, increasing traction on the reflected SO tendon and impairing telescoping 6). The ZT distance in patients (41.2 mm) was significantly longer than in normal children (37.1 ± 1 mm).
COVID-19-related mechanisms:
Possible mechanisms include direct viral invasion of skeletal muscle via ACE2 receptors, or immune-mediated myotoxicity and autoimmunity triggered by cytokine release 5). Onset approximately 3 weeks after infection is consistent with a reactive response.
It has been newly reported that ocular myasthenia gravis can present with BS-like findings 3). A mechanism by which AChR receptor blockade causes symptoms similar to restrictive strabismus has been suggested, and the need to include myasthenia gravis in the differential diagnosis for BS patients with vertical strabismus has been pointed out.
Based on a report of intermittent and recurrent BS (a 5-year-old boy who experienced spontaneous remission within one day), two new theories have been proposed 7).
Shilo et al. (2022) proposed two new theories: the “Stretch theory” (repeated stretching of a congenitally short SO tendon leads to tendon sheath thickening → stenosing tenosynovitis) and the “Avoidance theory” (acute pain → avoidance of eye movement → reduced tendon stretching → rapid spontaneous remission) 7).
Further validation through prospective studies is expected regarding the association between ZT distance and BS onset 6). It is anticipated to be used as a predictive indicator for the onset of congenital BS.