Dissociated vertical deviation (DVD) is an intermittent hypertropia in which the non-fixating eye elevates. When one eye is covered, the covered (non-fixating) eye becomes hypertropic, exhibiting abnormal eye movements that cannot be explained by Hering’s law (the law that equal innervation is sent to both eyes).
DVD always occurs bilaterally, although the degree may vary. Typically, when the non-fixating eye is covered, it slowly elevates, excyclotorts, and abducts. When the cover is removed, the eye slowly returns from upward to downward.
A related concept is dissociated strabismus complex (DSC). This is a collective term for a group of abnormal eye movements including DVD, dissociated horizontal deviation (DHD) in which the eye can become either esotropic or exotropic depending on the fixating eye, cyclotorsion, and latent nystagmus.
DVD is often associated with horizontal strabismus. Helveston reported that DVD occurs in 14% of patients with esotropia, 8.7% with exotropia, and 7.2% with hypertropia1). In infantile esotropia, DVD is found in 46–90% of cases. Many patients have poor binocular vision, but not all. DVD frequently coexists with inferior oblique overaction.
QWhat is the difference between DVD and ordinary vertical strabismus?
A
Ordinary vertical strabismus follows Hering’s law and can be explained by overaction of an elevator or underaction of a depressor in one eye. DVD does not follow Hering’s law; the covered eye elevates regardless of which eye is covered. DVD is always bilateral (though asymmetric), induced or modulated by occlusion, and cannot be diagnosed using Parks’ three-step test for single muscle palsy.
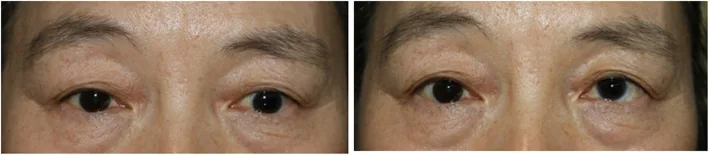
Choi HJ, et al. Heimann-Bielschowsky phenomenon and hypotropic DVD in case of monocular vision loss: a case report. BMC Ophthalmol. 2020. Figure 1. PMCID: PMC7318472. License: CC BY.
Two clinical photographs: on the left, vertical deviation of one eye creates an interocular difference; on the right, the eye position is nearly aligned, illustrating the variability of DVD.
Children rarely complain. Parents often notice “upward gaze” or “eye misalignment” and bring the child for examination. In manifest DVD, the non-fixing eye elevates during fatigue or daydreaming. Latent DVD appears only with monocular occlusion, so daily complaints are even fewer. Many patients have poor binocular vision, but not all.
In manifest DVD, a chin-up head posture may be adopted.
Movement during occlusion: The non-fixating eye slowly elevates. At the same time, it is accompanied by excyclotorsion and abduction.
Movement upon occlusion removal: When the occlusion is removed, the previously occluded eye slowly returns from upward to downward.
Variability in degree: The degree is small with brief occlusion. It becomes more apparent with prolonged occlusion. The strabismus angle also varies with attention. The strabismus angle often changes from day to day.
Associated Findings
Inferior oblique overaction: Overelevation occurs in adduction. It frequently coexists with DVD, and distinguishing between the two can be difficult.
Latent nystagmus: Nystagmus appears when one eye is occluded. According to Guyton’s hypothesis, it is closely related to the development of DVD.
Dissociated horizontal deviation (DHD): Abnormal eye movements that can be either esotropia or exotropia depending on the fixating eye. Combined with DVD, it constitutes dissociated strabismus complex (DSC).
Reduced binocular vision: Poor stereopsis. Often underlying is impaired binocular vision development due to infantile esotropia.
QIs DVD always visible?
A
There are two types of DVD: manifest and latent. Manifest DVD is observed even when both eyes are open, and the elevation of the non-fixating eye becomes apparent during fatigue, etc. Latent DVD appears only when one eye is covered and disappears when both eyes are open. Even if not noticeable in daily life, it is often first confirmed by the cover test.
There is no definitive explanation for the eye movement mechanism of DVD. Currently, the following two main hypotheses have been proposed.
Guyton (latent nystagmus) hypothesis: To attenuate latent nystagmus, a drive occurs for the fixating eye to adduct, depress, and intort. According to Hering’s law, the non-fixating eye shows a conjugate movement of abduction, elevation, and extorsion 2). The presence of latent nystagmus is thought to be closely related to the development of DVD.
Brodsky (dorsal light reflex) hypothesis: Due to lack of binocular vision, the primitive dorsal light reflex seen in fish and crustaceans is disinhibited 3). The phylogenetically old vestibulo-ocular reflex, normally suppressed by binocular vision, surfaces, and the disruption of binocular vision by monocular occlusion causes the occluded eye to elevate.
Both hypotheses can partially explain the features of DVD, but there remain aspects that cannot be explained by a single mechanism.
The alternate cover test is the basic diagnostic method. A characteristic finding is that when the cover is removed, the previously covered eye moves slowly from upward to downward.
Use of a translucent occluder: Using a translucent occluder allows direct observation of the covered eye through the cover, which is useful for evaluating DVD.
Confirmation of manifest and latent DVD: Confirm by both observation with both eyes open and the cover test.
Consideration of variability in severity: The degree may be smaller with brief occlusion. Also, the angle of strabismus can vary with attention, so multiple observations are necessary.
First, perform a rapid alternate cover test to measure the true vertical deviation component.
Next, to measure the DVD component, place a prism in front of the eye to be measured, cover it for a prolonged period, and then find the prism power at which the eye no longer moves when the cover is removed.
Since the deviation angle in DVD varies from day to day, accurate quantification is not easy.
Differentiation of DVD from inferior oblique overaction and true vertical deviation
The Parks 3-step test (a diagnostic method to identify the causative muscle of hypertropia) can lead to incorrect conclusions when DVD is present. The 3-step test cannot be applied in cases of DVD. When evaluating cases involving DVD, it is necessary to first confirm the presence or absence of DVD and then interpret the results of the 3-step test.
QHow is the strabismic angle of DVD measured?
A
The prism prolonged occlusion test is used. A prism is placed in front of the eye to be measured, and after prolonged occlusion, the prism power at which the eye no longer moves when the occlusion is removed is determined. However, since the angle of deviation in DVD often varies from day to day and also fluctuates with attention, accurate quantification is not easy. It is important to make a comprehensive judgment based on multiple measurements.
Surgery is considered when vertical deviation is noticeable in daily life. Specific indications include the following:
Manifest DVD with cosmetic concerns
Significant chin-up head posture
When inferior oblique overaction is associated with horizontal surgery for infantile esotropia
For latent DVD with little impact on daily life, observation is sufficient. Note that a definitive surgical procedure for DVD has not yet been established.
It is considered particularly effective when DVD and inferior oblique overaction coexist 5). The principle is to move the new insertion of the inferior oblique muscle anterior to the center of rotation of the globe, thereby eliminating its elevating function and converting it into a depressor. It is often performed simultaneously with horizontal strabismus surgery for infantile esotropia.
As a postoperative complication, attention should be paid to the risk of anti-elevation syndrome (a condition causing limitation of elevation) 6).
Superior rectus recession (bilateral SR recession)
This is a classic surgical procedure for DVD 7). The superior rectus muscle is recessed in both eyes. The amount of recession is usually 5 to 8 mm, adjusted according to the severity of DVD. Large recessions (7 mm or more) carry a risk of downgrade limitation.
This procedure involves suturing the muscle belly to the sclera 10 to 12 mm posterior to the muscle insertion. It is characterized by reducing only the excessive action without changing the stable eye position, and may be combined with superior rectus recession.
DVD is always binocular, but there is often a difference in severity between eyes. Surgery may be performed only on the more severe side. However, after unilateral surgery, the see-saw phenomenon may make DVD in the other eye more noticeable, in which case additional surgery is considered. Ultimately, bilateral surgery is often required.
DVD is a classic example of abnormal eye movement that does not follow Hering’s law (equal innervation to both eyes). While normal vertical strabismus can be explained by overaction of the elevator or underaction of the depressor in one eye, DVD cannot be explained by this law because the covered eye elevates regardless of which eye is covered.
Guyton proposed a hypothesis based on latent nystagmus as the mechanism of DVD 2). When one eye is covered, the direction of latent nystagmus changes, and the fixating eye moves in the direction of adduction, depression, and intorsion to maintain a more stable position. According to Hering’s law, the non-fixating (covered) eye shows a conjugate movement of abduction, elevation, and extorsion. This mechanism predicts a correlation between the intensity of latent nystagmus and the degree of DVD.
Details of Brodsky’s Dorsal Light Reflex Hypothesis
Brodsky explained DVD as disinhibition of a phylogenetically old reflex 3). Due to lack of binocular vision, the primitive dorsal light reflex (seen in fish and crustaceans, where the back turns toward the light) becomes disinhibited. This phylogenetically old vestibulo-ocular reflex, normally suppressed by binocular vision, emerges when binocularity is disrupted by covering one eye, causing the covered eye to elevate.
Integrated Understanding of Dissociated Strabismus Complex (DSC)
DVD, DHD, cyclodeviation, and latent nystagmus are not independent phenomena but are understood as a series of abnormal eye movements resulting from binocular visual dysfunction. Early disruption of binocular visual development due to infantile esotropia is considered the underlying pathology of DSC, providing a unified explanation for the frequent co-occurrence of these phenomena.
The high frequency of DVD (46–90%) in infantile esotropia suggests that the lack of binocular vision plays a central role in the development of DVD. However, DVD can also occur in cases with relatively preserved binocular vision, leaving aspects that cannot be explained by a single mechanism.
It has been reported that the timing of surgery for infantile esotropia may affect the development of DVD. Yagasaki et al. reported that in the group receiving ultra-early surgery (before 8 months of age), all DVD remained subclinical, whereas in the late surgery group, 38.9% developed manifest DVD 8). Furthermore, Shin et al. reported that late surgery was associated with the risk of manifest DVD, with an odds ratio of 8.23 (P<0.001) 9).
These findings suggest that early surgical intervention for infantile esotropia may reduce the severity of DVD, but currently, evidence from prospective comparative trials is insufficient, and validation through future multicenter studies is needed.
Inferior oblique anterior transposition (IOAT) is considered effective for simultaneous correction of DVD and inferior oblique overaction 5), but ongoing investigation is needed regarding the incidence of anti-elevation syndrome and its management 6). Accumulation of evidence on long-term outcomes remains a future challenge.
Helveston EM. Dissociated vertical deviation-a clinical and laboratory study. Transactions of the American Ophthalmological Society. 1980;78:734-79. PMID:7020216; PMCID:PMC1312158.
Stager DR, Parks MM. Inferior oblique anteriorization in the treatment of dissociated vertical deviation. Ophthalmology. 1995;102(8):1206-11.
Magoon EH. Bilateral superior rectus recession for dissociated vertical deviation. J Pediatr Ophthalmol Strabismus. 1981;18(4):38-42.
Yagasaki T, Yokoyama YO, Maeda M. Influence of timing of initial surgery for infantile esotropia on the severity of dissociated vertical deviation. Japanese journal of ophthalmology. 2011;55(4):383-388. doi:10.1007/s10384-011-0043-1. PMID:21647566.
Shin KH, Paik HJ, Kim SJ, et al. Factors associated with the development of manifest dissociated vertical deviation in patients with infantile esotropia. J AAPOS. 2014;18(6):549-53.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.