Multifocal contact lenses (MFCLs) are a type of contact lens that integrates different focal distances, such as distance and near, into a single lens. Their main use is for correcting presbyopia (age-related loss of accommodation), but they are also used for myopia progression control (mainly in children and young adults).
More than half of the Japanese population is myopic, and the proportion of people who notice a decline in accommodative ability increases rapidly after age 40. The presbyopic population (age 40 and over) in Japan is approximately 57 million, and the demand for bifocal contact lenses among contact lens users transitioning to presbyopia is increasing year by year.
Bifocal soft contact lenses (SCLs) are basically simultaneous vision type, so the quality of vision is somewhat inferior to that of bifocal spectacle lenses or alternating vision hard contact lenses (HCLs). However, using bifocal SCLs expands the clear vision range and reduces the burden on accommodation, thereby improving quality of life in daily activities.
Multifocal contact lenses for myopia management have a different design philosophy from those for presbyopia; they intentionally create myopic defocus on the peripheral retina to suppress axial elongation. The global myopic population is projected to reach 4.9 billion by 2050 15), increasing the public health importance of myopia progression control.
The following products and designs are being studied for myopia progression control with multifocal contact lenses.
Dual-focus design (e.g., MiSight 1 day): central distance correction zone + concentric plus addition zones (+2.00D)
Extended depth of focus (EDOF) design (e.g., MYLO): controls peripheral defocus by widening the depth of focus
Power gradient design: power changes progressively from center to periphery
Multifocal design (multi-zone type): has multiple focal zones (3 or more)
QHow are multifocal contact lenses different from regular single-vision contacts?
A
Multiple focal distances from distance to near are incorporated into a single lens, designed to allow those who have difficulty seeing near without glasses due to presbyopia to cover both distance and near vision in a state close to natural vision. However, compared to single-vision lenses, image sharpness is slightly inferior and contrast sensitivity in low light is reduced.
The main clinical findings to be checked when prescribing multifocal contact lenses are as follows.
QWill my vision at night worsen if I use multifocal contact lenses?
A
Due to the optical characteristics of multifocal designs, contrast sensitivity tends to decrease in low-light conditions compared to single-vision lenses. You may experience inconvenience in situations requiring fine vision in dim light, such as nighttime driving. If you drive frequently at night, we recommend consulting your doctor before prescription and preparing backup glasses as needed.
Presbyopia begins in the 40s, and accommodative power is almost lost by around age 60. The basic principle of presbyopia correction is to set the correction amount so that half of the accommodative power is reserved, and the remaining accommodative power can cover near work. The population aged 40 and over in Japan has reached approximately 57 million, indicating a large demand for presbyopia correction.
Before deciding on a prescription, try multifocal contact lenses to see how they work in daily life. It is important to evaluate them in situations that match the patient’s lifestyle, such as desk work, reading, driving, and smartphone use. The focus of evaluation is not on visual acuity numbers but on whether the patient can comfortably see what they want to see.
QIf I have dry eye before surgery, can I still use multifocal contact lenses?
A
Dry eye can worsen the wearing comfort of contact lenses and increase the risk of epithelial disorders such as smile-mark punctate keratopathy. First, treat the dry eye (with artificial tears, diquafosol sodium eye drops, etc.) and stabilize the ocular surface before considering a multifocal contact lens prescription. Choosing a silicone hydrogel lens with good water retention may improve wearing comfort.
Multifocal SCL designs are broadly divided into concentric ring type and EDOF type. Since different designs result in slightly different visual experiences, select the CL type that best matches the patient’s needs: one that stabilizes distance vision, intermediate vision, or near vision.
Principles of prescription procedure:
Prescription of multifocal SCLs should be performed after clarifying the goals of presbyopia correction.
Choose whether to set the dominant eye for distance and the non-dominant eye for near (monovision type) or set both eyes for multifocal (modified monovision).
Start trial fitting with a low addition (+1.00 to +1.50 D) and gradually increase the addition.
Trial fitting should last at least 15–20 minutes, evaluating at distance, intermediate, and near distances.
Evaluation at the patient’s primary viewing distances, such as PC, smartphone, reading, and driving, is important.
Obtain patient feedback on satisfaction and discomfort after the trial.
Backup glasses instruction: Because contrast decreases in dark environments where the pupil dilates, instruct patients to always carry backup glasses for nighttime driving.
Precautions for prescribing multifocal SCLs for myopia control:
When prescribing CLs to children, confirm that the parents have an appropriate management system.
Measure axial length every 6 months to monitor treatment efficacy.
If the effect is insufficient, consider switching to or adding orthokeratology or low-concentration atropine.
Myopia management CLs such as MiSight have a completely different purpose from presbyopia-correcting multifocal SCLs, and this should be clearly stated on the prescription.
Prescription of multifocal HCLs (hard contact lenses)
Multifocal HCLs generally have a design with distance vision in the center and near vision in the periphery. While they have elements of simultaneous vision, they also have elements of alternating vision like glasses, so posture and gaze direction during use are important.
Guidance on gaze usage:
With multifocal HCLs, which part of the lens is used changes depending on the gaze direction. The principle is that when looking downward, the HCL moves upward, bringing the peripheral near portion in front of the pupil.
Multifocal SCLs (simultaneous vision type)
Design: Concentric ring type, EDOF type, etc. Light for both distance and near reaches the retina simultaneously.
Advantages: Easy to wear. Soft material causes less foreign body sensation.
Disadvantages: Image sharpness is inferior to single vision lenses. Reduced contrast in low light.
Prescription tips: Set the dominant eye for distance. Start with low addition.
Bifocal/Multifocal HCL (Alternating Vision Type)
Design: The mainstream design has distance vision in the center and near vision in the periphery. The part of the lens used changes depending on the direction of gaze.
Advantages: High quality of vision. Can switch between distance and near by changing gaze direction.
Disadvantages: Requires adaptation to wearing. Posture and gaze guidance are important.
Prescription tips: When looking downward, the HCL moves upward, allowing use of the near portion.
Unlike HCLs, all SCLs require disinfection. Neglecting care such as rubbing, rinsing, and cleaning and drying the lens case can lead to serious eye disorders such as corneal ulcers. It is recommended to replace the lens case every month.
Care for daily disposable lenses (e.g., MiSight): Since they are discarded daily, the risk of infection is low and no care products are needed. This reduces the burden of hygiene management when prescribing to children. Many contact lenses for myopia management, such as MiSight 1 day, are daily disposable types, so no actual care during use is required.
Care for regularly replaced lenses:
Perform daily rubbing cleaning with a multipurpose contact lens care product.
Rinse the lens case daily and let it dry; replace every month.
Discard promptly if discoloration, deformation, or noticeable scratches appear.
Rinsing with tap water is strictly prohibited (risk of Acanthamoeba infection).
Regular check-ups:
All contact lens wearers, regardless of whether they use multifocal CLs, need regular eye examinations. Corneal condition, axial length (for myopia management), corrected visual acuity, and fitting evaluation should be performed every 6 months12).
QHow is the addition power of multifocal contact lenses determined?
A
The addition power is set so that half of the patient’s remaining accommodation is reserved, and the other half is used for near work. When switching from single-vision CLs, it is standard to start with a low addition (around +1.00 to +1.50 D) regardless of the prescription addition, and gradually adjust based on the patient’s subjective visual experience.
Selection of addition power for myopia control CLs
For multifocal CLs used for myopia management, the choice of addition power (+ADD) affects treatment efficacy. Key clinical data are summarized below.
Addition power
Representative product
Key study
Axial length suppression effect
+2.00 D
MiSight 1 day
Chamberlain 20195)
52% (3 years)
+2.50 D
BLINK study CL
BLINK RCT10)
36% (3 years)
High add power
Various manufacturers
Multiple studies4)
Tends to be higher
Higher add powers tend to have a greater effect on suppressing axial elongation, but also increase the reduction in visual quality (especially under low-light conditions). Therefore, the decision should be made considering the patient’s age, lifestyle, and daily activities. In the risk-benefit analysis by Bullimore et al. (2021), the safety profile of myopia management interventions was comprehensively evaluated, and multifocal CLs are considered to have good overall safety8).
Selection criteria for various optical therapies in myopia management
In the systematic review by Yam et al. (2025), the efficacy and safety of various myopia management interventions were summarized10), and selection of the optimal intervention for each patient is recommended. Situations where multifocal CLs are particularly suitable are as follows.
Children and adolescents who prefer daytime CL wear or are already CL users
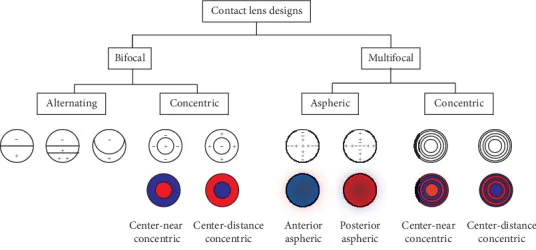
Remón L, et al. Bifocal and Multifocal Contact Lenses for Presbyopia and Myopia Control. J Ophthalmol. 2020;2020:8067657. Figure 1. PMCID: PMC7152962. License: CC BY.
Diagram showing main design variations of concentric multifocal contact lenses (red: near zone, blue: distance zone). Corresponds to the optical characteristics of simultaneous vision design discussed in section “6. Pathophysiology and Detailed Mechanism of Onset”.
Optical Mechanisms of Simultaneous Vision and Alternating Vision
Simultaneous vision type (bifocal/multifocal SCL): Light from both distance and near reaches the retina simultaneously. The brain uses neural suppression to select the dominant focus based on viewing distance. The smaller the pupil size, the greater the depth of focus, making it easier to achieve a bifocal CL effect. When the pupil dilates in dark conditions compared to bright conditions, light interferes between distance and near zones, reducing contrast.
Alternating vision type (bifocal HCL): The part of the lens used is determined by the direction of gaze and head tilt. Similar to the principle of bifocal eyeglass lenses, looking downward causes the lens to move upward, bringing the peripheral near zone in front of the pupil.
Concentric SCL: The distance and near portions each have a weak progressive power design, with a steep progressive power connection between them (design a), or a design where the power progresses from distance to near (design b). There are two types: center-distance and center-near.
EDOF type (Extended Depth of Focus): Concentric progressive power lenses are arranged aperiodically with varying powers, designed to extend the depth of focus. There is no concept of center-distance or center-near, and stable vision is obtained from distance to intermediate distances.
Presbyopia is a condition in which near accommodation becomes difficult with aging due to decreased elasticity of the crystalline lens and reduced function of the ciliary muscle. Symptoms typically appear around age 40, and accommodative power is almost completely lost by age 60. Bifocal/multifocal CLs optically compensate for this loss of accommodation and do not treat the crystalline lens itself.
On the other hand, multifocal SCLs for myopia progression control (peripheral myopic defocus design) have a completely different optical design from those for presbyopia correction. The center provides distance correction, and concentric treatment zones have plus addition power (+2.00 to +2.50 D), creating myopic defocus on the peripheral retina to suppress axial elongation. This design principle is based on the same “peripheral retinal myopic defocus hypothesis” as orthokeratology and DIMS spectacles. A comprehensive review by Remón et al. (2020) details the diversity of designs and their impact on clinical outcomes for bifocal/multifocal CLs in presbyopia and myopia control 7).
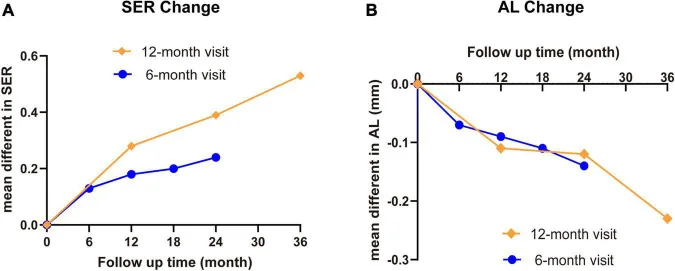
Chen M, et al. Myopia Control With Multifocal Lens in School-Aged Children: A Meta-Analysis. Front Pediatr. 2022;10:889243. Figure 7. PMCID: PMC9251339. License: CC BY.
Meta-analysis summary diagram summarizing differences in spherical equivalent refraction and axial length changes between multifocal lenses (MFL) and single vision lenses (SVL) in school-age children. Corresponds to multifocal soft CLs for myopia control discussed in Section “7. Latest Research and Future Perspectives”.
Multifocal soft CLs designed to slow myopia progression, with a different design from bifocal SCLs for presbyopia, are being developed and studied. A mechanism has been proposed in which a center-distance, periphery-near design reduces hyperopic defocus in the peripheral retina, thereby suppressing myopia progression.
In the AAO Ophthalmic Technology Assessment (Cavuoto 2024), a review of 12 studies (11 Level I, 1 Level II) was conducted 4). SE change was −0.22 to −0.81 D in the treatment group (control: −0.50 to −1.45 D), and axial elongation was 0.05 to 0.39 mm in the treatment group (control: 0.17 to 0.67 mm), with statistically significant differences confirmed in 11–12 studies. No serious adverse events were reported 4). Bullimore et al. (2021) examined the risks and benefits of myopia management in general and confirmed that multifocal CLs have a favorable safety profile 8). A meta-analysis by Haarman et al. (2020) showed that the risk of complications increases exponentially with each 1 D increase in myopia9), supporting the medical rationale for intervention. The global myopia population is projected to reach 4.9 billion by 2050 15), highlighting the growing public health importance of myopia progression control.
In a 3-year double-blind RCT of MiSight 1 day (dual-focus design) (Chamberlain 2019), significant suppression was shown: refraction −0.51 D (control −1.24 D, p<0.0001) and axial elongation 0.30 mm (control 0.62 mm, p<0.0001) 5).
The Cochrane systematic review by Walline et al. (2020) also summarized intervention evidence for myopia progression control, positioning multifocal CLs as an effective option 1).
With the spread of digital devices, development is progressing on trifocal designs that cover distance, intermediate, and near vision, as well as smart contact lenses that electronically switch focus. In particular, emphasis is being placed on addressing intermediate distances (50–80 cm, the distance for smartphone and PC use)2).
In a randomized controlled trial using dual-focus contact lenses by Aller et al. (2016), significant myopia progression control was demonstrated over one year: SE change −0.22 D (control −0.79 D, p<0.001) and axial elongation 0.05 mm (control 0.24 mm, p<0.001)6). A systematic review by Yam et al. (2025) also confirmed the role of multifocal contact lenses in myopia progression control10).
The Guidelines for Myopia Management Spectacle Lenses (1st edition, 2025) organize the differences in characteristics between segmented lenses and multifocal contact lenses, recommending selection based on age, lifestyle, and compliance11). In cases of rapid myopia progression, combination with low-concentration atropine eye drops may be considered12). Compared with orthokeratology, a meta-analysis (Si 2015) reported an axial length suppression rate of 43% for orthokeratology13), making it an option alongside multifocal contact lenses. Together with the combination therapy RCT by Kinoshita et al. (2020)14), a myopia management strategy tailored to each patient’s situation is important.
Advances in Bifocal/Multifocal Contact Lens Design
The design of bifocal/multifocal contact lenses (especially SCLs) is changing rapidly, with older designs being discontinued and new designs continuously appearing. It is necessary to prescribe while constantly updating the latest product information. To improve patient satisfaction, research on individualized prescribing (customized prescribing) according to individual visual needs is also progressing3).
Remón et al. (2020) comprehensively reviewed the design and optical characteristics of bifocal and multifocal contact lenses for presbyopia and myopia control, discussing that the choice of design significantly affects clinical outcomes7).
Walline JJ, Lindsley KB, Vedula SS, et al. Interventions to slow progression of myopia in children. Cochrane Database Syst Rev. 2020;1(1):CD004916. doi:10.1002/14651858.cd004916.pub4.
Wolffsohn JS, Calossi A, Cho P, et al. Global trends in myopia management attitudes and strategies in clinical practice - 2019 Update. Cont Lens Anterior Eye. 2020;43(1):9-17.
Woods J, Woods C, Fonn D. Visual Performance of a Multifocal Contact Lens versus Monovision in Established Presbyopes. Optometry and vision science : official publication of the American Academy of Optometry. 2015;92(2):175-82. doi:10.1097/OPX.0000000000000476. PMID:25525891.
Cavuoto KM, Trivedi RH, Prakalapakorn SG, Oatts JT, Nallasamy S, Morrison DG, Pineles SL, Chang MY. Multifocal Soft Contact Lenses for the Treatment of Myopia Progression in Children: A Report by the American Academy of Ophthalmology. Ophthalmology. 2025;132(4):495-503. doi:10.1016/j.ophtha.2024.09.031. PMID:39503665; PMCID:PMC11930616.
Chamberlain P, Peixoto-de-Matos SC, Logan NS, Ngo C, Jones D, Young G. A 3-year Randomized Clinical Trial of MiSight Lenses for Myopia Control. Optometry and vision science : official publication of the American Academy of Optometry. 2019;96(8):556-567. doi:10.1097/OPX.0000000000001410. PMID:31343513.
Aller TA, Liu M, Wildsoet CF. Myopia Control with Bifocal Contact Lenses: A Randomized Clinical Trial. Optometry and vision science : official publication of the American Academy of Optometry. 2016;93(4):344-52. doi:10.1097/OPX.0000000000000808. PMID:26784710.
Remón L, Pérez-Merino P, Macedo-de-Araújo RJ, Amorim-de-Sousa AI, González-Méijome JM. Bifocal and Multifocal Contact Lenses for Presbyopia and Myopia Control. Journal of ophthalmology. 2020;2020:8067657. doi:10.1155/2020/8067657. PMID:32318285; PMCID:PMC7152962.
Mark A. Bullimore, Eric R. Ritchey, Sunil Shah, Nicolas Leveziel, Rupert R.A. Bourne, D. Ian Flitcroft. The Risks and Benefits of Myopia Control. Ophthalmology. 2021;128(11):1561-1579. doi:10.1016/j.ophtha.2021.04.032.
Annechien E. G. Haarman, Clair A. Enthoven, J. Willem L. Tideman, Milly S. Tedja, Virginie J. M. Verhoeven, Caroline C. W. Klaver. The Complications of Myopia: A Review and Meta-Analysis. Invest. Ophthalmol. Vis. Sci.. 2020;61(4):49. doi:10.1167/iovs.61.4.49.
Yam JC, Zhang XJ, Zaabaar E, Wang Y, Gao Y, Zhang Y, et al. Interventions to reduce incidence and progression of myopia in children and adults. Progress in retinal and eye research. 2025;109:101410. doi:10.1016/j.preteyeres.2025.101410. PMID:41109517.
Si JK, Tang K, Bi HS, et al. Orthokeratology for myopia control: a meta-analysis. Optom Vis Sci. 2015;92:252-257. doi:10.1097/OPX.0000000000000505. PMID:25599338.
Kinoshita N, Konno Y, Hamada N, et al. Efficacy of combined orthokeratology and 0.01% atropine solution for slowing axial elongation in children with myopia: a 2-year randomised trial. Sci Rep. 2020;10:12750. doi:10.1038/s41598-020-69710-8. PMID:32728111; PMCID:PMC7391648.
Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123:1036-1042. doi:10.1016/j.ophtha.2016.01.006. PMID:26875007.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.