Fungal keratitis is a general term for keratitis caused by fungal infection of the cornea. It is also called “keratomycosis,” including conditions where fungi proliferate in the cornea without inflammation, but the Japanese Infectious Keratitis Clinical Practice Guidelines, 3rd edition, use the term “fungal keratitis” for the usual inflammatory condition 1).
Fungi are morphologically divided into the following two types. Their clinical features, risk factors, and treatment strategies differ significantly.
Filamentous fungi: Multicellular structures with branching filaments. Causative organisms include Fusarium species (representative: Fusarium solani), Aspergillus species, Alternaria species, Paecilomyces species, etc. 1)
Yeast-like fungi: Unicellular, spherical or oval, about 3–4 μm in diameter. Most are Candida species, with C. albicans being the representative species 1).
Epidemiologically, filamentous fungal infections are often caused by trauma from fungi living on plant surfaces or in soil, and are thus contrasted as “rural type,” while yeast infections are associated with ocular surface diseases and steroid eye drops, and are contrasted as “urban type.”
A multicenter prospective observational study by Inoue et al. (2016, Journal of the Japanese Ophthalmological Society) reported the current status of patient background, clinical findings, treatment, and prognosis of fungal keratitis8). Globally, the frequency is higher in warmer regions, and it is estimated that more than one million people per year are affected in tropical and subtropical areas7). In temperate Asia, Alternaria species are the third most frequently isolated filamentous fungi after Candida and Fusarium species1). In temperate regions, rare causative organisms such as Curvularia species, in addition to Fusarium species, have been sporadically reported6).
Fungal keratitis rarely occurs in healthy eyes with no risk factors; it is often triggered by trauma, steroid eye drops, contact lens wear, or ocular surface diseases1).
QHow is fungal keratitis different from bacterial keratitis?
A
Fungal keratitis progresses more slowly than bacterial keratitis, with relatively mild pain and no response to broad-spectrum antibiotics. Filamentous fungi show feathery, ill-defined infiltrates, and satellite lesions or endothelial plaques may be observed. Definitive diagnosis requires demonstration of fungi by smear microscopy or culture, and treatment involves antifungal agents.
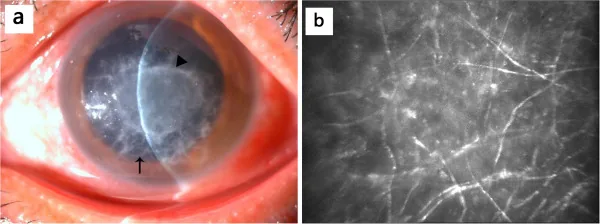
Qiu WY, et al. Mycotic keratitis caused by concurrent infections of Exserohilum mcginnisii and Candida parapsilosis. BMC Ophthalmol. 2013. Figure 1. PMCID: PMC3751109. License: CC BY.
The anterior segment photograph shows gray-white infiltration and opacity in the corneal stroma with irregular, feathery margins. The confocal microscopy image shows branching linear hyperreflective structures, supporting the clinical and diagnostic findings of fungal keratitis.
Patient-reported symptoms are as follows. Compared to bacterial keratitis, progression is slower and early symptoms are mild, which can lead to delayed diagnosis1).
Redness: Mixed conjunctival and ciliary injection. In cases on steroid eye drops, redness may be absent1)
Eye pain: Mild cases may have a foreign body sensation; severe cases present with intense pain
Vision loss: Progresses with enlargement of the lesion and corneal opacity
Photophobia: Appears depending on the degree of inflammation
Tearing and discharge: Non-specific symptoms associated with inflammation
In the very early stages, subjective symptoms may be mild, with only slight epithelial damage. The relatively mild pain and slow progression are characteristic of fungal keratitis and serve as clues for differentiation from bacterial keratitis1).
The clinical appearance observed with a slit lamp differs significantly between filamentous fungi and yeasts.
Filamentous Fungi
Hyphate ulcer: Presents with ill-defined, feathery gray-white infiltrates. This is a characteristic finding of filamentous fungal infection.
Elevated lesions: Firm on scraping.
Satellite lesions: Small infiltrates scattered around the main lesion.
Endothelial plaque: Forms a disc-shaped white deposit on the posterior corneal surface. It results from fungal hyphae that have crossed Descemet’s membrane into the anterior chamber or from a strong immune reaction to deep hyphae.
Hypopyon: A severe finding indicating inflammatory spread into the anterior chamber.
Yeasts
Localized abscess: Presents as a well-demarcated, button-shaped or round infiltrate.
Superficial localization: Often confined to the superficial corneal stroma.
Tendency to melt: Corneal stromal melting is observed around the lesion. Soft on scraping.
Similarity to bacterial keratitis: Clinically difficult to distinguish from staphylococcal infection; smear microscopy and culture are essential for differentiation.
Filamentous fungi tend to progress toward the deep corneal layers, and as the infection spreads, it eventually causes severe stromal melting leading to corneal perforation. On the other hand, species such as Alternaria, which grow well at low temperatures, tend to spread superficially across the corneal surface. If steroid eye drops have been administered, typical findings may be modified, making diagnosis difficult, so caution is required1).
Among filamentous fungi, the most frequent and likely to cause severe disease is the genus Fusarium, with Fusarium solani being the representative species. Other genera such as Aspergillus, Alternaria, Paecilomyces (now Purpureocillium lilacinum), and Curvularia can also cause corneal infection1).
Among yeasts, Candida species are overwhelmingly the most common, with Candida albicans being the representative. In recent years, the isolation frequency of C. parapsilosis has increased, and caution is needed because C. glabrata and C. krusei have low susceptibility to fluconazole1).
A common risk factor for fungal keratitis shared by filamentous fungi and yeasts is the use of steroid eye drops before onset1).
Risk factors for filamentous fungi: Plant-related trauma (poking the eye), ocular injury during farm work, contact lens wear, steroid eye drops1). Since filamentous fungi inhabit plant surfaces and soil, trauma involving these is the greatest risk factor. This is called the “rural type.”
Risk factors for yeasts: History of ocular surface disease, history of ophthalmic surgery (especially after corneal transplantation), steroid eye drops, diabetes1). It occurs when commensal yeast-like fungi proliferate on a susceptible ocular surface. This is called the “urban type.”
QShould I always see an ophthalmologist if I injure my eye during farm work?
A
Ocular trauma from plants or soil is the greatest risk factor for filamentous fungal keratitis. Symptoms are often mild initially, so it tends to be neglected, and delayed diagnosis can lead to corneal perforation. If redness, foreign body sensation, or decreased vision persist after injury, see an ophthalmologist early.
Corneal ulcers that do not respond to broad-spectrum antibiotics, the presence of satellite lesions, and large ulcers with minimal discharge are important findings that should raise suspicion for fungal infection 1). Based on corneal findings, it is clinically possible to estimate whether the infection is filamentous or yeast, and patient background (history of trauma, steroid use, contact lens wear, ocular surgery) is used as a reference for differential diagnosis.
Definitive diagnosis requires demonstration of fungi from the lesion 1). Since fungi require time to grow, treatment should be initiated when this disease is clinically suspected, without waiting for culture results 1).
Specimen collection: Corneal scrapings are collected from the border between the ulcer and normal cornea. Using a spatula or similar instrument, scrape a larger area than the lesion, collect the scraped tissue with a cotton swab, and inoculate it onto fungal culture media 1).
Smear microscopy: The following staining methods are used 1):
Gram stain: Fungi stain gram-positive, but detection is difficult if the number is small.
Fungi-Flora Y stain: Specifically fluorescently stains chitin and cellulose, enabling sensitive detection of fungi. Observed with a fluorescence microscope. This is the standard staining method in Japan.
Culture examination: Use Sabouraud dextrose agar or potato dextrose agar, and incubate at 37°C and room temperature for at least 2 weeks 1). Slow-growing fungi may require 3–4 weeks for identification.
Antifungal susceptibility testing: Since drug susceptibility varies greatly by fungal species, perform testing if possible to guide treatment selection 1).
Anterior segment OCT (AS-OCT): Can objectively evaluate the depth and thickness of corneal lesions. Useful for detecting satellite lesions, necrotic spaces, and hyperreflective endothelial plaques on the endothelial surface 1).
In vivo confocal microscopy (IVCM): Allows non-invasive direct observation of corneal cells, nerve fibers, fungi, and Acanthamoeba. Requires skill to perform and interpret results 1).
Molecular diagnosis (PCR): Useful for rapid species identification. Todokoro et al. identified Alternaria alternata by DNA sequence analysis 4). Not available at all facilities.
Fungal keratitis must be differentiated from other infectious keratitis. In particular, lesions caused by yeast resemble staphylococcal infections, so microbiological examination is important for differentiation1).
Contact lens wear history, radial keratoneuritis, ring infiltrate
Herpes keratitis
Dendritic lesions, history of recurrence, decreased corneal sensation
QWhat tests are needed for a definitive diagnosis of fungal keratitis?
A
For definitive diagnosis, it is necessary to demonstrate fungi from scrapings of the corneal lesion. Hyphae are confirmed by smear microscopy using Fungiflora Y staining or Gram staining, and culture is performed on Sabouraud agar medium. Since culture takes at least 2 weeks, treatment should be started based on clinical findings without waiting for culture results.
Treatment of fungal keratitis responds poorly compared to bacterial infections and is prolonged. Based on the Japanese Infectious Keratitis Clinical Practice Guidelines, 3rd edition, a multifaceted approach combining topical and systemic antifungal agents and lesion debridement is recommended1). Since it may take at least 1 week, or up to 4 weeks for slow-growing fungi, to identify the causative organism, treatment should be started immediately if this disease is suspected based on clinical findings1).
Three classes of antifungal agents are used depending on the fungal species. Among ophthalmic topical medications, only the polyene pimaricin (5% eye drops, 1% eye ointment) is covered by insurance; all others are extemporaneous preparations used clinically1).
Polyene agents: Bind to ergosterol in the fungal cell membrane, directly damaging the membrane and exerting fungicidal effects. Includes pimaricin and amphotericin B. Pimaricin is the first-line drug for Fusarium species1). 5% pimaricin eye drops are called natamycin overseas and are widely used internationally. 1% pimaricin eye ointment is a dosage form sold only in Japan, and the ointment formulation causes less eye irritation1). Since 5% pimaricin eye drops are a suspension, white powder may adhere to the eyelid margin and the base of corneal ulcers. Penetration into the deep cornea is poor.
Azole agents: Inhibit the synthesis of ergosterol, a major component of the fungal cell membrane, and act fungistatically. They have high selectivity and are relatively safe. Extemporaneously prepared fluconazole 0.2% solution, miconazole 0.1% solution, and voriconazole 1% solution are used1). Fluconazole eye drops have a long history of use but are ineffective against filamentous fungi. Voriconazole eye drops have a broad antifungal spectrum and are an important alternative to pimaricin, but they are less effective against Fusarium species1).
Candin agents: Selectively inhibit β-glucan synthesis in the fungal cell wall, exerting fungicidal effects. Extemporaneously prepared micafungin sodium 0.1% solution is used as eye drops1). Effective against Candida species or Aspergillus species, but ineffective against Fusarium species. Corneal tissue penetration is poor.
The Infectious Keratitis Clinical Practice Guidelines, 3rd edition, recommend establishing treatment strategies by dividing into yeast-like fungi (Candida species), Fusarium species, and filamentous fungi other than Fusarium species1).
Yeast (Candida species)
First-line: Azole agents alone or in combination with multiple drugs.
Combination therapy: Combination of azole and candin agents is also recommended.
Cautions: Be aware of the increase in fluconazole-resistant strains (C. glabrata, C. krusei). 1% pimaricin eye ointment can also be used, but be cautious of corneal epithelial damage due to drug toxicity.
Filamentous fungi
Fusarium species: Polyene pimaricin is the first-line treatment. Considering the high isolation frequency, a regimen including pimaricin should be considered from the start.
Non-Fusarium: Voriconazole 1% eye drops are recommended. Especially consider use for Aspergillus, Paecilomyces, and Scedosporium species.
Refractory cases: If no improvement with pimaricin, consider adding voriconazole eye drops.
In severe cases, the following combination of drugs is considered as a reference prescription. Add subconjunctival injection (item 4) depending on corneal findings.
In addition to eye drops, systemic administration of antifungal agents is combined. In severe cases, subconjunctival or intrastromal injections are used. Atropine is used for anti-inflammation, and steroid eye drops are not used. Antibacterial eye drops are combined for bacterial co-infection management.
Recommendation level for extemporaneous voriconazole eye drops
In the 3rd edition of the Infectious Keratitis Clinical Practice Guidelines, CQ-6 states that voriconazole extemporaneous eye drops are conditionally recommended for the treatment of fungal keratitis, with a recommendation strength of “weak recommendation” and evidence level of “B”1).
The RCTs supporting voriconazole eye drops were all conducted overseas (India) and mainly targeted filamentous fungal keratitis1).
Mycotic Ulcer Treatment Trial (MUTT): The largest RCT involving 323 cases compared 1% voriconazole eye drops with 5% pimaricin (natamycin) eye drops. Results showed that 5% pimaricin eye drops were superior in both healing rate and improvement in corrected visual acuity1),9). Fusarium species accounted for 40% of the causative fungi, and in the subgroup analysis of Fusarium species alone, the pimaricin group also showed better outcomes1)
118-case RCT: 5% pimaricin was superior in both healing rate and final visual acuity. Similar results were seen for Fusarium species, but no significant difference for Aspergillus species1)
120-case RCT: No significant difference in corrected visual acuity at 3 months between the 1% voriconazole group and the 5% pimaricin group. For Fusarium species, corneal perforation was significantly more frequent in the voriconazole group1)
40-case RCT (refractory cases): In cases unresponsive to 5% pimaricin eye drops, comparison between the group adding 1% voriconazole eye drops and the group adding voriconazole intrastromal injection (50 μg/0.1 mL). No significant difference in healing rate, but corrected visual acuity at 3 months was better in the eye drop addition group1)
Based on this evidence, 1% voriconazole eye drops are shown to be a treatment option for fungal keratitis caused by filamentous fungi other than Fusarium species. It is particularly worth considering in cases unresponsive to pimaricin, especially those caused by Aspergillus species1).
There is no clear evidence for the efficacy of systemic administration of antifungal drugs 1). Polyene pimaricin is poorly water-soluble and has a high molecular weight, resulting in poor penetration into the deep corneal layers. In severe cases of Fusarium with corneal neovascularization, intravenous infusion of liposomal amphotericin B may compensate for poor drug penetration 1). The azole voriconazole, when administered systemically, penetrates into the anterior chamber1). Because systemic administration has many side effects, it is desirable that the causative fungus has been identified and the target is clear 1).
Lesion debridement enhances the penetration of eye drops into the tissue and physically reduces the fungal load 1). Since the effectiveness of drug therapy varies depending on the type of fungus, debridement should be actively combined to enhance treatment efficacy. In prescription examples, debridement is performed about twice a week. Caution is needed for corneal perforation if the cornea is thinned. For superficial types such as Alternaria, superficial keratectomy as an extension of debridement is also effective 1).
Superficial keratectomy: In cases that respond poorly to treatment and where lesion debridement is insufficient, the lesion is removed along with the pathogen 1)
Therapeutic keratoplasty: Performed when the lesion reaches deep layers and responds poorly to medication, or when perforation occurs. It is important to excise the abscess and the surrounding hyphate ulcer sufficiently. If transplantation is performed in a highly active state, fungi are likely to remain at the margin, leading to a poor prognosis1)
Conjunctival flap: Promotes healing of infection through abundant blood supply
Intrastromal injection: For deep abscesses that do not respond to topical treatment, voriconazole or amphotericin B can be injected directly into the stroma. For details, see the “Latest Research” section
QHow long does treatment for fungal keratitis take?
A
Treatment for fungal keratitis can last from several weeks to several months. Compared to bacterial keratitis, the response to medication is slower, and penetration of eye drops into the deep corneal layers is poor, requiring long-term continuation of treatment. Regular follow-up during treatment is essential, and if the causative organism is identified, revising the prescription based on drug susceptibility test results is also useful.
When the integrity of the corneal epithelium is compromised by trauma or ocular surface disease, adherent fungi proliferate within the tissue and establish infection 1). In addition to trauma, when there is increased susceptibility of the ocular surface due to conditions such as diabetes or long-term use of steroid eye drops, yeast-like fungi (e.g., Candida) that normally reside on the conjunctival sac or skin can become causative agents. In contact lens wearers, environmental fungi that proliferate in the lens case can be the cause.
Once fungi adhere to and proliferate on the corneal epithelium, establishing infection, neutrophils migrate and aggregate at the lesion, forming a white infiltrate. As tissue destruction progresses, an abscess forms, and ulceration occurs beyond Bowman’s membrane. Neutrophil migration also occurs into the anterior chamber, and when inflammatory cells become numerous, hypopyon forms. Proteolytic enzymes, antigens, and toxins produced by the fungi are released into the cornea, causing necrosis and structural damage.
Differences in Pathophysiology between Filamentous Fungi and Yeasts
Filamentous fungi (especially Fusarium species) tend to extend hyphae toward the deep corneal layers, and when they breach Descemet’s membrane and expand on the posterior corneal surface, they form an endothelial plaque. Even without breaching Descemet’s membrane, a strong immune response to deeply infiltrated filamentous fungi can also produce an endothelial plaque. As the infection spreads, severe melting eventually occurs, which can lead to corneal perforation.
On the other hand, yeasts tend to take a form of corneal mycosis with less inflammation than filamentous fungi. The lesion is confined to the superficial corneal stroma, forming a well-demarcated abscess with a tendency to melt.
Polyenes: Fungicidal agents that irreversibly bind to ergosterol in the fungal cell membrane, disrupting the cell membrane. They have a broad spectrum and strong efficacy, but because they can also act on human cell membranes, side effects are relatively common 1).
Azoles: Fungistatic agents that inhibit ergosterol synthesis. They have high selectivity and relatively high safety 1).
Echinocandins: Selectively inhibit the synthesis of β-D-glucan in the fungal cell wall. They are fungicidal against Candida species and fungistatic against Aspergillus species. Because the target is absent in human cells, side effects and toxicity are low, but corneal tissue penetration of eye drops is poor 1).
7. Latest Research and Future Perspectives (Investigational Reports)
Dong et al. reported two cases of deep corneal fungal infection resistant to topical antifungal agents, in which a single intracameral injection of amphotericin B (10 μg/0.1 mL) achieved a final best-corrected visual acuity of 20/20 in both cases 2). This method has the advantage of delivering the drug directly to the deep corneal layers and anterior chamber, which are difficult to reach with topical or systemic administration.
Because topical antifungal eye drops have large molecular weights and poor penetration into the deep corneal stroma, intrastromal injection, which directly injects the drug into the lesion, has been attempted for refractory deep lesions.
The drugs used are voriconazole (50 μg/0.1 mL) and amphotericin B (5–10 μg/0.1 mL). A technique has been reported in which, under an operating microscope, the needle bevel is oriented downward and inserted obliquely from a disease-free area, and the drug is divided into five injections around the abscess to form a drug barrier. The injected drug remains as a depot in the stroma and is said to maintain effective concentrations for about 7 days. Animal studies have reported that concentrations of amphotericin B exceeding 20 μg/0.1 mL cause corneal edema, epithelial erosion, and neovascularization, so careful concentration management is necessary.
Ler et al. reported a case of deep filamentous fungal infection (Penicillium species) successfully treated with intrastromal injections of voriconazole 50 μg/0.1 mL administered circumferentially around the lesion, repeated three times at 5-day intervals 3).
In a study of 25 patients who did not respond to natamycin and voriconazole eye drops, 72% responded to intrastromal voriconazole injection. Most of the non-responders were culture-positive for Fusarium species. In another study of 20 patients, 14 responded to injection, requiring an average of 2.65 injections.
In an RCT of 40 patients with fungal keratitis unresponsive to 5% pimaricin eye drops, comparing the addition of 1% voriconazole eye drops versus intrastromal voriconazole injection, there was no significant difference in cure rate, but corrected visual acuity at 3 months was better in the eye drop addition group 1). Although this RCT had a limited number of cases, it did not demonstrate superiority of intrastromal injection over eye drops.
Intrastromal injection is an adjunctive therapy to topical and systemic administration, not a standalone treatment. Future challenges include establishing the optimal number and interval of injections, verifying efficacy by fungal species (especially against Fusarium species), and evaluating the combined effects with other adjunctive therapies.
PACK-CXL (Photoactivated Chromophore for Keratitis-Corneal Cross-linking) is a treatment that stabilizes the corneal stroma and simultaneously inactivates pathogens using riboflavin and ultraviolet A irradiation 7). Corneal cross-linking was originally developed for the treatment of keratoconus (Dresden protocol), but since 2008 it has been clinically applied to infectious keratitis, and the name PACK-CXL was adopted in 2013 7). It has a mechanism of action that does not depend on antibiotics and is expected as a new treatment option for the increasing drug-resistant bacteria. Many preclinical studies on fungal infections have also been reported, but the optimal protocol for refractory fungi such as Fusarium species is still under development 7).
Importance of species identification and drug susceptibility testing
Todokoro et al. successfully treated a case of Alternaria alternata keratitis associated with Mooren’s ulcer by identifying the fungal species through DNA sequence analysis and confirming the MIC of voriconazole as 0.5 μg/mL in drug susceptibility testing 4). With combined use of topical voriconazole and topical steroids, visual acuity recovered to 0.7 after three months. This suggests that combining molecular diagnosis and drug susceptibility testing may improve the precision of individualized treatment.
Risk of fungal infection after amniotic membrane transplantation
Chen et al. reported two cases of Fusarium keratitis and Sistotrema biggsiae keratitis that developed within 10 days after amniotic membrane transplantation5). This is the first report of human infection with Sistotrema biggsiae in the literature. The interval for developing infectious keratitis after amniotic membrane transplantation is usually reported as 28 to 347 days, and attention has been drawn to early-onset cases 5).
Multicenter prospective observational study in Japan
Inoue et al. conducted a multicenter prospective observational study on patient background, clinical findings, treatment, and prognosis of fungal keratitis, and reported the current status of this disease in Japan in the Journal of the Japanese Ophthalmological Society 8). This provides important baseline data on the distribution of causative fungi and treatment outcomes of fungal keratitis in Japan.
Dong LK, Krebs DB. An intracameral approach for recalcitrant fungal keratitis. American journal of ophthalmology case reports. 2022;25:101369. doi:10.1016/j.ajoc.2022.101369. PMID:35146213; PMCID:PMC8818535.
Ler D, Pidro A, Miokovic AP. Challenging case of treating fungal keratitis. Romanian journal of ophthalmology. 2022;66(1):69-74. doi:10.22336/rjo.2022.14. PMID:35531444; PMCID:PMC9022159.
Todokoro D, Miyakubo T, Komori A, Tamura T, Makimura K, Akiyama H. Successful Management of Fungal Keratitis by Alternaria alternata Complicating Mooren’s Ulcer. Case reports in ophthalmology. 2023;14(1):153-158. doi:10.1159/000529979. PMID:37065728; PMCID:PMC10091228.
Chen L, Dahshan D, Mauger T. Fungal keratitis after amniotic membrane placement. American journal of ophthalmology case reports. 2024;33:101972. doi:10.1016/j.ajoc.2023.101972. PMID:38188608; PMCID:PMC10770418.
Reiber MA, Touleyrou L. Not All Fungi and Games: An Unusual Case of Fungal Keratitis in Michigan. Cureus. 2025;17(9):e92251. doi:10.7759/cureus.92251. PMID:41098247; PMCID:PMC12518886.
Kowalska ME, Pot SA, Hartnack S. Photoactivated Chromophore for Keratitis-Corneal Cross-linking (PACK-CXL)-A Scoping Review Based on Preclinical Studies. Translational vision science & technology. 2024;13(7):14. doi:10.1167/tvst.13.7.14. PMID:39023444; PMCID:PMC11262473.