Blepharitis is an inflammatory disease centered on the eyelid margin. It is also called marginal blepharitis. It is one of the most common conditions in ophthalmology, occurring in all age groups and ethnicities. Although it usually does not directly threaten vision, severe cases can lead to corneal epithelial damage and corneal neovascularization.
Anatomically, it is broadly divided into anterior blepharitis and posterior blepharitis. Anterior blepharitis involves inflammation from the eyelash roots to the skin side and is classified by cause into staphylococcal (ulcerative) blepharitis and seborrheic (squamous) blepharitis. Mixed types with both features are not uncommon. Posterior blepharitis primarily involves inflammation of the meibomian glands and is often treated as meibomian gland dysfunction (MGD)3)4).
MGD is defined as “a condition with diffuse abnormalities in meibomian gland function due to various causes, accompanied by chronic ocular discomfort” 4). MGD is broadly classified into two types: hyposecretory and hypersecretory, with hyposecretory type accounting for the majority 4).
In addition, Demodex blepharitis associated with infestation by hair follicle mites (Demodex folliculorum and Demodex brevis) has gained attention as a disease subtype1). Demodex infestation is found in approximately 30% of patients with chronic blepharitis, and antiparasitic treatment may be effective in refractory cases.
A population-based study of residents aged 6 to 96 years in Japan showed that the prevalence of MGD clearly increases with age4).
Age 19 and under: 0%
20s: 11.8%
30s: 5.6%
40s: 21.6%
50s: 32.8%
60s: 41.9%
70s: 48.4%
80s: 63.9%
Regarding sex differences, multiple reports indicate a higher prevalence in men and postmenopausal women4). Risk factors include aging, Asian ethnicity, rural residence, video display terminal work, smoking, soft contact lens wear, and long-term use of glaucoma eye drops4). In a US survey, signs of blepharitis were found in 37–47% of ophthalmic outpatients, with staphylococcal blepharitis being more common in relatively younger individuals (mean age 42 years) and women. Demodex-related blepharitis has been reported in over 80% of those aged 60 years and older, and nearly 100% in those aged 70 years and older1).
QHow common are blepharitis and MGD?
A
In a survey of Japanese residents, the prevalence of MGD was approximately 11.8% in their 20s, 21.6% in their 40s, 41.9% in their 60s, and 63.9% in their 80s4). It clearly increases with age, and more than half of elderly individuals are estimated to have some degree of meibomian gland dysfunction. It is reported to be more common in men and postmenopausal women4).
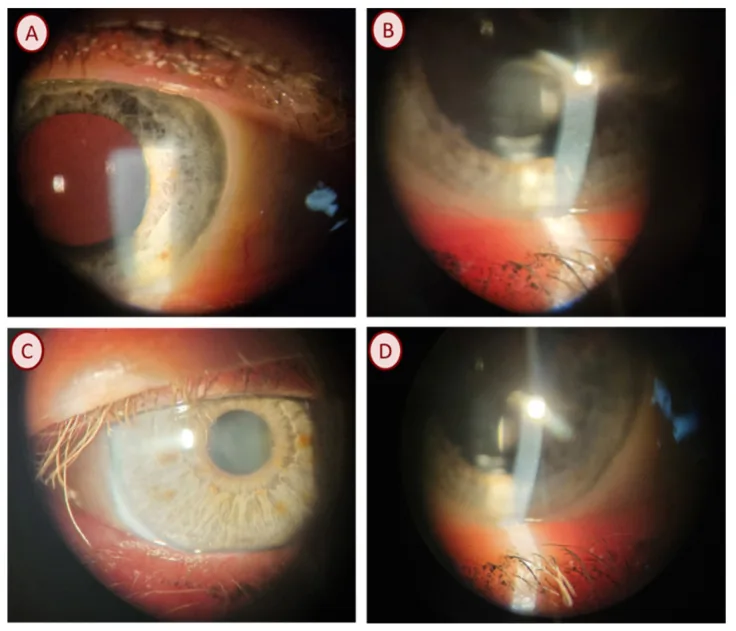
Pyzia J, et al. Demodex Species and Culturable Microorganism Co-Infestations in Patients with Blepharitis. Life (Basel). 2023. Figure 2. PMCID: PMC10533081. License: CC BY.
(A) Meibomian gland dysfunction, keratinous dandruff, mild blepharitis; (B) Meibomian gland dysfunction, telangiectasia of the eyelid margin, tearing; (C) Meibomian gland obstruction, telangiectasia of the eyelid margin; (D) Clinical picture of Demodex blepharitis showing meibomian gland obstruction. Corresponds to “Meibomian gland dysfunction” discussed in the section “2. Main symptoms and clinical findings.”
The main symptoms of chronic blepharitis are burning sensation, foreign body sensation, and itching of the eyelids. It may also be accompanied by hyperemia, tearing, discharge, blurred vision, and photophobia. Symptoms tend to worsen in the morning and are characterized by repeated remissions and exacerbations. In staphylococcal blepharitis, patients often experience acute burning sensation and redness of the eyelid margin. In contrast, seborrheic blepharitis typically presents with relatively mild chronic burning and foreign body sensation.
MGD is characterized by ocular discomfort, a feeling of pressure, dryness, fatigue, and a sensation described as “sticky” 4). Differential diagnosis based solely on subjective symptoms is difficult, and comprehensive assessment with slit-lamp microscopy findings is necessary 4).
Demodex blepharitis is characterized by intense itching from night to early morning, with 80% of patients reporting interference with daily activities, 47% difficulty driving at night, and 34% restrictions on contact lens use or makeup 1).
Observation using a slit-lamp microscope, especially with a diffuser, is fundamental. Findings by disease type are summarized below.
Anterior blepharitis
Staphylococcal (follicular): Bilateral eyelid margin redness, small papules, small pustules, small ulcers, and crusting. Fibrin-derived collarettes surrounding the base of the eyelashes are a characteristic finding. In severe cases, hair follicles are destroyed, leading to hair loss (madarosis) or trichiasis, and chronic conjunctivitis or keratoconjunctival punctate epithelial erosions may occur.
Seborrheic: Redness and edema are milder than in staphylococcal blepharitis, but there is hyperemia around the eyelid margin and greasy, easily removable scales. Multiple eyelashes clumping together, known as “seborrheic eyelashes”, is a characteristic finding. Since hair follicles are not destroyed, eyelashes regenerate.
Posterior blepharitis (MGD)
Opening findings: Obstruction of meibomian gland openings (plugging, pouting, ridge), disarrangement, anterior or posterior displacement of the mucocutaneous junction, irregular eyelid margin, and telangiectasia of the eyelid margin are observed 4). Upon lid pressure, yellow liquid or solidified contents are expressed.
Associated findings: In seborrheic cases, meibomian foam forms at the lower eyelid margin. Severe cases may involve tarsal thickening and palpebral conjunctival papillary hypertrophy. Decreased tear lipid layer leads to evaporative dry eye, often complicated by diffuse superficial keratitis 3)4).
Demodex blepharitis
Pathological signs: Cylindrical dandruff at the base of the eyelashes is a highly significant pathological finding and, like collarettes, serves as a diagnostic clue1)2). It is accompanied by conjunctival hyperemia, redness and swelling of the eyelid margin, telangiectasia, and excessive eyelash loss.
Special forms: Demodex brevis resides within the meibomian glands and may not be detected by eyelash epilation testing. Cases have been reported where it can be detected by expressing meibum after cleaning the eyelid margin and directly observing it under a microscope5). In pediatric cases, severe keratitis with corneal ulcers and neovascularization has been reported, and it is important to consider Demodex in the differential diagnosis of treatment-resistant keratitis2).
In Japanese clinical practice, the Shimazaki classification, which evaluates the quality of meibum by applying moderate pressure to the center of the tarsal plate, is widely used.
Grade 0: Clear meibum is easily expressed with light pressure (normal)
Grade 1: Cloudy meibum is expressed with light pressure
Grade 2: Cloudy meibum is expressed with moderate or greater pressure
Grade 3: No meibum is expressed even with strong pressure
Grade 2 or higher is considered abnormal and is used to determine “decreased meibum secretion” in the diagnostic criteria for MGD4).
QWhat are collarettes?
A
Collarettes are scales (dandruff-like deposits) that form around the base of the eyelashes. In staphylococcal blepharitis, fibrin formed at ulcerated areas of the eyelid margin is lifted as the eyelashes grow. In Demodex blepharitis, they are called cylindrical dandruff and serve as a diagnostic clue as a highly significant pathological finding1)2).
The etiology of blepharitis is multifactorial, and the main causes differ depending on the type.
Staphylococcal blepharitis is associated with staphylococcal proliferation on the ocular surface. Cultures are positive for Staphylococcus aureus in 46–51% of patients, significantly higher than the 8% in healthy individuals. Bacterial exotoxins cause punctate epithelial keratopathy in the adjacent corneal and conjunctival epithelium. Moraxella is an important cause of angular blepharitis.
Seborrheic blepharitis is frequently associated with seborrheic dermatitis, with reports that 95% of patients have seborrheic dermatitis. Rosacea dermatitis has been reported in 20–42% of patients with all types of blepharitis and is recognized as an important cause of blepharitis.
Mechanism of MGD development: The main pathology of hyposecretory MGD is considered to be hyperkeratinization of the meibomian gland duct epithelium and atrophy of the acini4). Acinar atrophy may occur not only secondary to obstruction but also due to primary damage to gland cells from aging and other factors.
Ocular factors: Asian ethnicity, prolonged visual display terminal work, soft contact lens wear, long-term use of glaucoma eye drops, history of ocular surgery
Demodex (Demodex folliculorum and Demodex brevis) parasitizes sebaceous glands, hair follicles, and meibomian glands, and their excreta and secretions cause follicular obstruction and inflammation1). Inflammatory cytokines such as IL-1β and IL-17, and MMP-9 are activated. Demodex also acts as a vector for bacteria such as Staphylococcus aureus, Acinetobacter baumannii, and Streptococcus pneumoniae, potentially promoting secondary infection of the ocular surface1).
Association with dry eye is also important. Dry eye is observed in 50% of patients with staphylococcal blepharitis. In MGD, deficiency of the tear lipid layer leads to increased evaporation, and the comorbidity rate of dry eye reaches 25–40%3). MGD and dry eye have a mutually exacerbating relationship.
QHow are dry eye and blepharitis related?
A
The two conditions are closely related. Qualitative and quantitative reduction of the tear oil layer due to MGD is a major cause of evaporative dry eye3). Conversely, decreased tear production leads to reduced lysozyme and immunoglobulins, promoting the development of staphylococcal blepharitis. Therefore, treatment of blepharitis and dry eye should be carried out concurrently.
Diagnosis is based on medical history and slit-lamp examination. Determine whether onset is acute or chronic, bilateral or unilateral, and painful or painless. Inquire about systemic diseases (Sjögren syndrome, rosacea, diabetes, atopy, thyroid disease, sinusitis), allergy history, use of cosmetics and eye drops, contact lens wear, and smoking history.
Inspection and palpation evaluate eyelid redness, swelling (diffuse or localized), tenderness, and eczema. Unilateral painful localized swelling suggests hordeolum or acute chalazion; bilateral diffuse painful swelling suggests eyelid abscess or orbital cellulitis.
Diagnosis of hyposecretory MGD requires all three of the following items to be positive4).
Diagnostic Item
Positive Criteria
Subjective symptoms
Symptoms such as ocular discomfort, foreign body sensation, or pressure sensation
Findings around the orifice
One or more of the following: vascular dilation, displacement of the mucocutaneous junction, or irregularity of the eyelid margin
Orifice obstruction findings
Obstructive findings such as plugging, and Shimazaki classification grade 2 or higher
This diagnostic criteria proposed by the MGD Working Group in 2010 is widely used, but there is still no internationally unified diagnostic criteria4).
Meibography (infrared): Allows non-invasive observation of meibomian gland morphology. Dropout area, gland shortening, and dilation can be quantified, and it is recommended for MGD diagnosis4)
Tear film break-up time (TBUT): Often shortened in MGD, but not a specific test4)
Slit-lamp observation of meibum: Recommended for performance4)
Fluorescein staining: Most versatile for evaluating corneal and conjunctival epithelial damage4)
Tear osmolarity measurement: Useful for diagnosing concurrent dry eye, reported to have 59% sensitivity and 94% specificity at ≥316 mOsm/L
Microscopic examination of epilated eyelashes is the basic method. Lee et al. identified adult and larval D. folliculorum under light microscopy by epilating 4 eyelashes from each upper and lower lid2). However, D. brevis may not be detected by eyelash epilation because it hides within the meibomian glands. Zhang and Liang reported detecting 15 D. brevis by expressing meibum after antiseptic treatment of the eyelid margin and microscopic observation, noting that Demodex blepharitis can present with D. brevis only in the meibum without external findings5).
In cases of severe recurrent anterior blepharitis or treatment-resistant cases, bacterial culture of the eyelid margin (Staphylococcus, Moraxella) is indicated. For marked asymmetry, unilateral refractory chalazion-like lesions, or in middle-aged to elderly patients, eyelid biopsy should be considered to rule out sebaceous gland carcinoma. Sebaceous gland carcinoma is known to masquerade as refractory blepharitis or chalazion-like lesions.
Differential diagnoses include chalazion, eyelid abscess, orbital cellulitis, herpetic blepharitis (VZV, HSV), allergic blepharitis, eyelid dermatitis (contact, drug-induced, atopic), eczematous blepharitis, and sebaceous gland carcinoma.
Blepharitis is a chronic condition, and the mainstay of treatment is control of symptoms and inflammatory signs. There is no strong evidence for a cure, and long-term management is required. When MGD is present, treatment should be built around warm compresses, eyelid hygiene, and meibum expression 4).
First-line: Eyelid care (warm compresses, eyelid hygiene, meibum expression)
Warm compresses raise the eyelid temperature to the melting point of meibum, dissolving it and promoting secretion, while also improving eyelid blood flow 4). Instruct patients to use a commercially available warm eye mask at home twice daily for at least 5 minutes. Hot towels are convenient but difficult to regulate temperature, and when wet, they cool due to evaporative heat loss, making them a second choice.
Eyelid hygiene involves using a cotton ball moistened with water or a commercially available cleansing agent (e.g., diluted baby shampoo) to gently clean the eyelash roots with a cotton swab 4). Improvement is expected in subjective symptoms, meibomian gland orifice findings, meibum grade, TBUT, and keratoconjunctival epithelial damage. Note that adverse events may occur depending on the type of cleansing agent 4).
Meibum expression is considered for obstructive MGD4). In the clinic, use specialized instruments such as the Arita meibomian gland forceps (Inami) and perform the procedure at intervals of 10 days to 1 month. If plugging is large, remove it with forceps or an injection needle after topical anesthesia.
Topical antibiotics: For staphylococcal blepharitis, apply bacitracin or erythromycin ophthalmic ointment to the eyelid margin before bedtime for 2 to 8 weeks. Azithromycin hydrate ophthalmic solution may improve subjective symptoms, orifice findings, and meibum grade in MGD4).
Oral antibiotics: Tetracyclines and macrolides are used for their anti-inflammatory and lipid-regulating effects. Tetracycline tapered from 1,000 mg/day to 250 mg/day, minocycline hydrochloride tapered from 200 mg/day to 100 mg/day, doxycycline 100 mg orally twice daily tapered over 3–4 months, and combination with macrolides such as clarithromycin are employed. These are thought to exert effects by inhibiting bacterial enzyme activity and biofilm formation.
Topical steroids: When inflammation is severe, 0.1% fluorometholone is used short-term in combination. Combined with eyelid hygiene and warm compresses, it may improve symptoms, tear break-up time (TBUT), eyelid margin findings, and meibum quality4). In Japan, insurance coverage is limited to cases with blepharitis4).
Artificial tears and supplemental eye drops: Used adjunctively in cases complicated by evaporative or aqueous-deficient dry eye. If used four or more times daily, preservative-free formulations are preferred. Sodium diquafosol eye drops may improve dry eye symptoms in complicated cases, but are not typically used as monotherapy for MGD4).
Treatment of Demodex Blepharitis
Tea tree oil (TTO): The main component, terpinen-4-ol (T4O), exhibits acetylcholinesterase inhibitory activity, exerting a miticidal effect1). Used at concentrations of 5–50%. A report described improvement in all cases with weekly 50% TTO eyelid scrubs and daily 0.4% PHMB scrubs for 6 weeks2).
Oral and topical antiparasitic drugs: Combination of ivermectin (acts on GABA receptors of parasites, inducing paralysis) and metronidazole (DNA damage via nitro radicals) is considered most effective1). Both oral and topical routes are considered.
Mechanical debridement: Combined eyelid margin scrubs and warm compresses, with daily eyelid care continued.
Adjunctive therapy: Artificial tears are added in cases complicated by dry eye.
The mechanisms of action of drugs against Demodex are compared below.
Treatment
Mechanism of Action
Remarks
TTO
AChE inhibition1)
Widely available
Ivermectin
GABA receptor inhibition1)
Enhanced effect when combined with metronidazole1)
Angular blepharitis: Administer antibiotic eye drops or ointment with high sensitivity to staphylococci.
Herpetic blepharitis (HSV): Start acyclovir ointment (Zovirax ointment) 5 times daily, then reduce frequency as improvement occurs. Combine with antibiotic eye drops 3 times daily to prevent mixed infection. Generally, do not use steroids concurrently.
Herpetic blepharitis (VZV, herpes zoster ophthalmicus): Systemic administration of acyclovir or valacyclovir hydrochloride from early onset can lead to early improvement of lesions.
Cyclosporine A eye drops have limited efficacy for MGD alone and are usually not performed4). IPL (Intense Pulsed Light) treatment has been reported to be effective, but it should be considered at specialized facilities after confirming its approval and insurance coverage in Japan4).
QPlease tell me about eyelid care that can be done at home.
A
The basics are warm compresses, eyelid massage, and eyelid hygiene, three steps in total3)4). First, apply a clean towel or a warm eye mask to the eyelids for at least 5 minutes twice a day. Next, gently massage the upper and lower eyelids in a vertical direction to promote meibomian gland secretion. Finally, carefully clean the eyelash roots with a water-moistened cotton ball or a dedicated cleansing agent. Even after the acute phase subsides, daily continuation is important.
The development of staphylococcal blepharitis involves direct ocular surface irritation by bacterial toxins and enhanced cell-mediated immunity against Staphylococcus aureus. Bacterial exotoxins cause punctate epithelial damage to the adjacent corneoconjunctival epithelium. Bacterial lipases act on meibomian gland lipids to produce free fatty acids, which trigger inflammation and further gland obstruction, forming a vicious cycle.
The essence of MGD is obstruction of the terminal ducts of the meibomian glands3). The main pathologies of hyposecretory MGD are hyperkeratinization of the ductal epithelium and atrophy of the acini4). Atrophy of the acini may occur not only secondary to meibomian gland obstruction but also as a primary impairment of gland cells due to aging, among other factors4). Hyperkeratinization of the ductal epithelium and increased viscosity of meibum lead to progressive obstruction, resulting in gland dropout, atrophy, and decreased secretion.
The tear film lipid layer consists of an outer nonpolar layer and an inner polar layer, contributing to evaporation prevention and smoothing of the optical surface3). Reduced lipid supply from the meibomian glands leads to evaporative dry eye and increased tear osmolarity, inducing ocular surface inflammation and epithelial damage3). Changes in lipid layer composition (increased ceramides and cholesterol) have been shown to cause disruption and destabilization of the meibomian lipid film3).
In Demodex infestation, mite excrement and secretions cause physical obstruction of hair follicles and activate host hypersensitivity reactions1). Inflammatory cytokines such as IL-1β and IL-17, as well as MMP-9, are induced. Furthermore, D. folliculorum has been reported to act as a vector for bacteria such as Staphylococcus aureus, Acinetobacter baumannii, and Streptococcus pneumoniae, potentially promoting secondary infection of the ocular surface1). D. brevis has been reported to reside within meibomian glands and present with MGD-like findings, and some cases are difficult to diagnose based solely on external findings5).
Development of new treatments for Demodex-related blepharitis has been actively progressing in recent years.
Lotilaner ophthalmic solution 0.25% (XDEMVY) is an isoxazoline compound that inhibits Demodex GABA receptors and glutamate-activated chloride channels, inducing spastic paralysis1). In a phase 3 clinical trial (Saturn-2 trial, 412 patients), twice-daily instillation for 6 weeks achieved a collarette resolution rate of 56%, mite eradication rate of 51.8%, and erythema resolution rate of 31.1%1). 90.7% of participants reported good tolerability, with side effects such as burning sensation and mild visual impairment being minor1). It has been approved by the US FDA, but approval in Europe is expected around 2027, and the approval timeline in Japan is undetermined1).
IPL (Intense Pulsed Light) therapy irradiates broadband light, immobilizing and killing mites through photothermal effects1). In vitro experiments have confirmed mite death when their temperature rises to approximately 49°C. After four IPL treatments, significant improvements in OSDI, tear lipid layer, TBUT, meibomian gland secretion, and a reduction in mite count were reported1). Some reports indicate that improvement at one month was more rapid and pronounced compared to TTO alone. It is necessary to confirm domestic approval and insurance coverage before considering its use in specialized facilities4).
BlephEx is a method that mechanically removes debris, mites, and collarettes from the eyelid margin using a rotating microsponge1). It is also expected to disrupt bacterial biofilms. Combined use with TTO has been reported to significantly improve OSDI parameters and mite count, but further research is needed to verify long-term efficacy1).
Exploration of natural essential oils is also underway, with reports that sage oil kills mites within 7 minutes and peppermint oil within 11 minutes1). Synergistic effects of castor oil, bergamot oil, and nigella seed oil are also being investigated.
Czepińska-Myszura et al. state that “among novel treatments, only Lotilaner ophthalmic solution has demonstrated high efficacy in large-scale clinical trials, while IPL and BlephEx have only been validated in limited patient groups”1).
Lee et al. analyzed 9 cases of Demodex blepharitis, reporting that all cases were D. folliculorum and that pediatric cases (ages 5, 13, and 14) also presented with severe keratitis involving corneal ulcers and neovascularization2). Demodex infection in children is easily overlooked, and differential diagnosis of Demodex is important in recurrent keratitis2). Additionally, Zhang and Liang reported a 46-year-old male with 15 Demodex brevis organisms found only in the meibum without external findings, demonstrating that direct observation of meibum after lid margin cleaning contributes to diagnosis in refractory cases5).
QCan Lotilaner (XDEMVY) be used in Japan?
A
As of 2025, Lotilaner ophthalmic solution 0.25% (XDEMVY) is approved by the US FDA but not yet approved in Japan or Europe1). Approval in Europe is expected around 2027. The approval timeline in Japan is undetermined, and treatment currently relies on TTO and antiparasitic drugs.
Czepińska-Myszura A, Kozioł MM, Rymgayłło-Jankowska B. Pharmacotherapy of Demodex-Associated Blepharitis: Current Trends and Future Perspectives. Pharmacy. 2025;13(5):148. doi:10.3390/pharmacy13050148. PMID:41149876; PMCID:PMC12567107.
Lee YI, Seo M, Cho KJ. Demodex Blepharitis: An Analysis of Nine Patients. The Korean journal of parasitology. 2022;60(6):429-432. doi:10.3347/kjp.2022.60.6.429. PMID:36588421; PMCID:PMC9806504.
Saama Sabeti, Ahmad Kheirkhah, Jia Yin, Reza Dana. Management of meibomian gland dysfunction: a review. Survey of Ophthalmology. 2020;65(2):205-217. doi:10.1016/j.survophthal.2019.08.007.