Phototherapeutic keratectomy (PTK) is a procedure that uses an excimer laser (wavelength 193 nm) to remove superficial corneal opacities, irregularities, and deposits. It is positioned as a bridge between medical and surgical treatments for corneal diseases and is used for both therapeutic and refractive purposes.
From the late 1980s to the early 1990s, the excimer laser was applied to photorefractive keratectomy (PRK) and LASIK. PTK was approved by the US FDA in 1995 for the treatment of anterior segment corneal diseases.
The excimer laser operates on the principle of photoablation, breaking intermolecular bonds and vaporizing corneal tissue. Approximately 0.25 µm of tissue is removed per pulse, allowing precise control of ablation depth. Opacities up to 150 µm from the surface, including the epithelium (about 50 µm), can be removed. Compared to manual keratectomy, PTK results in less irregular astigmatism and shorter treatment time.
QHow is PTK different from PRK (photorefractive keratectomy)?
A
PTK is a therapeutic procedure to remove superficial corneal opacities and irregularities. PRK is a procedure to change the curvature of a normal cornea to correct refractive errors. Both use the same excimer laser (193 nm), but the laser irradiation profile and purpose differ.
In lattice corneal dystrophy type I, PTK is the first choice when amyloid deposits are mainly in the superficial cornea. PTK can be performed up to about two times, but if recurrence is frequent or opacities extend deeper than the mid-stroma, superficial, deep, or full-thickness keratoplasty is selected.
In granular and lattice corneal dystrophies, PTK is a reasonable means to delay eventual deep lamellar keratoplasty or PK 1). However, postoperative haze may occur.
For corneal opacities after shield ulcer, PTK is advantageous both for visual function and wound healing when there is strong scar opacity in the superficial stroma.
Refractory filamentary keratitis localized to the central cornea is also an indication for PTK.
Deep stromal scars: Require deep ablation, high risk of haze and hyperopic shift
Systemic diseases: Poorly controlled diabetes or collagen diseases (e.g., rheumatoid arthritis, SLE) can cause delayed epithelial healing
Herpes activity within 6 months: Risk of herpes simplex virus reactivation by excimer laser 1)
Corneal hypoesthesia: Increases risk of epithelial healing problems and stromal melting
QWhat corneal opacities are suitable for PTK?
A
Superficial opacities confined to the anterior 10–20% of the cornea (within about 150 µm from the surface) are the best candidates. Deep stromal scars require excessive ablation, leading to haze and hyperopic shift, and are not indicated. A residual stromal bed of at least 250 µm is required.
4. Preoperative Evaluation and Examination Methods
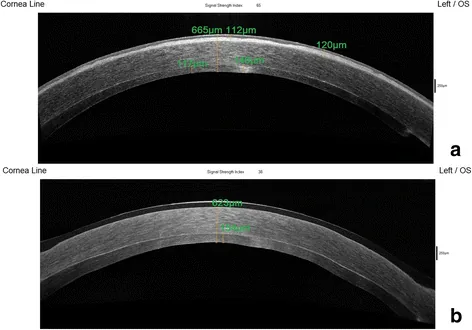
Kymionis G, Oikonomakis K, Petrelli M, et al. Treatment of anterior corneal scarring, following DSAEK graft failure, with combined graft exchange and phototherapeutic keratectomy. Eye Vis (Lond). 2017;4:12. Figure 2. PMID: 28484724; PMCID: PMC5418814; DOI: 10.1186/s40662-017-0078-6. License: CC BY.
Anterior segment OCT allows comparison of corneal surface shape and stromal thickness changes before and after treatment. This image shows the effect of PTK on corneal surface irregularity.
Performed under topical anesthesia (4% xylocaine or 0.5% proparacaine hydrochloride). General anesthesia may be used in children. A lid speculum is placed to begin the procedure.
The patient fixates on a fixation light, or the laser is manually centered for ablation. If the surface is rough, a masking agent (hydroxypropyl methylcellulose [HPMC] 0.7–2%) is applied to smooth it, ensuring the laser hits only the elevated areas.
When 70–80% of the target ablation depth is reached, confirmation is performed using a slit-lamp microscope.
Corrected visual acuity improves due to reduction in opacity density and irregular astigmatism. When flap creation and PTK are combined, corrected visual acuity significantly improves at 2, 6, and 12 months postoperatively1).
However, central ablation flattens the cornea and induces hyperopic shift. A 6 mm diameter, 100 µm depth ablation causes approximately 1.5 D of hyperopic shift.
QHow much hyperopic shift occurs after PTK?
A
For a 6 mm diameter, 100 µm ablation, approximately 1.5 D (diopters) of hyperopic shift is expected. The deeper the ablation, the greater the hyperopic shift. In some cases, PTK and PRK are combined to adjust the refractive change.
The excimer laser (ArF laser, wavelength 193 nm) is a far-ultraviolet laser. The photon energy at this wavelength exceeds the dissociation energy of carbon-carbon and carbon-nitrogen bonds, directly cleaving intermolecular bonds in corneal tissue and causing vaporization. Thermal damage is minimal, and the effect on surrounding tissue is minimized.
The reason PTK is uniquely effective in band keratopathy is that calcium deposits are ablated faster than the surrounding corneal tissue 1). However, this differential ablation may create surface irregularities, making proper use of masking agents important.
A study comparing PTK (Cretan protocol) and mechanical epithelial removal for epithelial removal during corneal cross-linking reported that the PTK group showed better visual and refractive outcomes2). PTK not only removes the epithelium but also has the effect of reshaping the irregular corneal surface.
Simultaneous combination (PTK/PRK + corneal cross-linking) has been reported to be more effective than sequential combination (PRK 6 months after corneal cross-linking)2), and further accumulation of evidence is expected.
American Academy of Ophthalmology Corneal/External Disease Preferred Practice Pattern Panel. Corneal Edema and Opacification Preferred Practice Pattern. San Francisco: AAO; 2024.
Randleman JB, Khandelwal SS, Hafezi F. Corneal cross-linking. Open Ophthalmol J. 2018;12:181-195.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.