Simple Corneal Erosion
Cause: Mostly mechanical trauma
Course: Usually heals within a few days
Characteristics: Transient epithelial defect that does not recur

A corneal epithelial defect is a condition in which the full thickness of the corneal epithelium is lost. It is generally used synonymously with “corneal erosion.” The corneal epithelium consists of approximately 5–7 layers of stratified squamous epithelium. The entire layer is replaced approximately every 7 days. About one layer per day is shed from the surface, and homeostasis is maintained by basal cell division and limbal stem cell supply.
Thoft et al. expressed this homeostasis with the formula X + Y = Z1). X represents corneal basal cell proliferation, Y represents limbal stem cell migration and supply, and Z represents corneal surface cell shedding. When the state X + Y < Z persists, an epithelial defect occurs1).
Corneal epithelial defects are clinically classified into the following three types.
Simple Corneal Erosion
Cause: Mostly mechanical trauma
Course: Usually heals within a few days
Characteristics: Transient epithelial defect that does not recur
Recurrent Corneal Erosion
Cause: Poor adhesion to the basement membrane
Course: Repeated recurrence after healing
Feature: Sudden onset of eye pain upon waking
Persistent Corneal Epithelial Defect (PED)
Cause: Corneal hypoesthesia, stem cell damage, etc.
Course: No epithelialization for 2 weeks or more
Feature: Formation of a rolled-up edge at the defect margin
Common symptoms include eye pain, foreign body sensation, tearing, photophobia, and blurred vision. However, characteristics differ depending on the disease type.
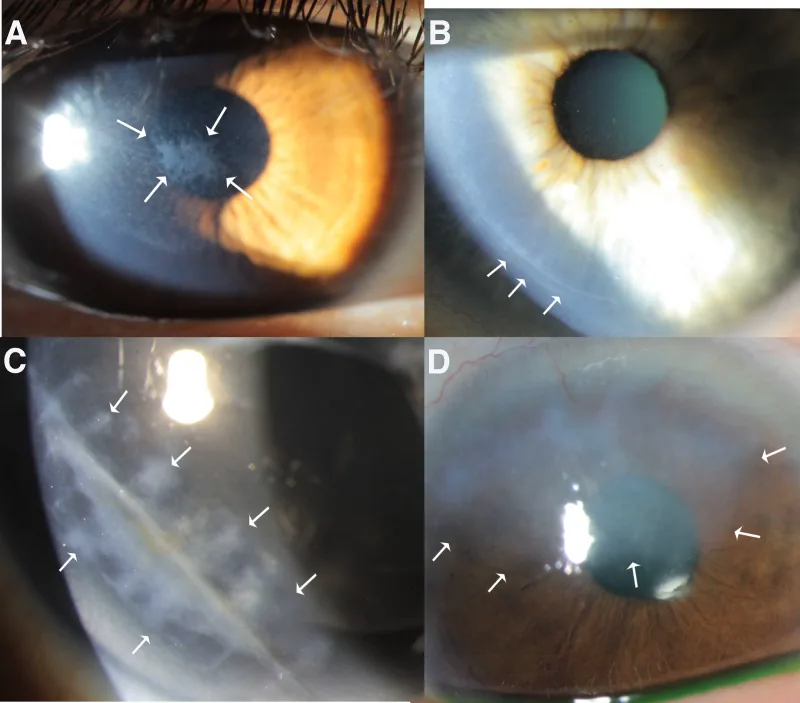
Fluorescein staining vividly highlights the epithelial defect. The cobalt blue filter of the slit lamp microscope is used to evaluate the extent, shape, and depth of the defect.
Ordinary (simple) corneal erosion does not recur once healed. In contrast, recurrent corneal epithelial erosion causes erosion at the same site weeks to years after healing. It typically presents with sudden eye pain upon waking, caused by poor adhesion of the epithelium to the basement membrane. The history of trauma may be unclear, making it easy to misdiagnose as corneal herpes.
The causes of corneal epithelial defect are diverse.
| Classification | Typical causes |
|---|---|
| Trauma | Mechanical trauma, UV keratitis, chemical injury |
| Ocular surface disease | Dry eye, limbal stem cell deficiency |
| Neurological disorders | Neurotrophic keratopathy, diabetic keratopathy |
| Drug-induced | Preservative toxicity / 5-FU / EGFR inhibitors |
| Structural abnormality | Entropion / Incomplete eyelid closure (lagophthalmos) |
This is the most common cause. Corneal abrasions from paper edges, fingernails, and fingers are frequent. Most recurrent erosions are triggered by trauma, although patients may not remember the initial injury.
During general anesthesia, approximately 60% of patients have incomplete eyelid closure, exposing the cornea to drying and trauma2). Exposure keratopathy occurs at a rate of 0.9 to 3.3 per 1,000 general anesthesia procedures2). In patients with eyelash extensions, complete eyelid closure with eye protectors is hindered, further increasing the risk2).
Cope et al. (2024) reported a case of a patient with blepharitis and dry eye associated with eyelash extensions who developed a corneal abrasion during general anesthesia for cesarean section2). Complete eyelid closure could not be achieved with eye protectors, and a 0.5 cm × 0.5 cm epithelial defect was observed in the inferior cornea postoperatively.
Eye drops containing cytotoxic anticancer drugs such as 5-FU suppress the division of corneal basal cells and cause corneal erosions1). Without a drug-free interval (chemo holiday), recurrent corneal erosions may occur1).
Tanaka et al. (2024) reported a case in which continued use of 1% 5-FU eye drops for conjunctival papilloma without a drug holiday resulted in recurrent corneal epithelial erosions1). The erosions healed after discontinuation of the eye drops and recurred upon resumption.
EGFR inhibitors (such as panitumumab) delay corneal epithelial wound healing4). EGF in tears plays a central role in maintaining corneal epithelial homeostasis through EGFR, and EGFR inhibitors block this pathway, leading to impaired healing and thinning of the epithelium4).
Chronic epithelial damage caused by preservatives in eye drops (particularly benzalkonium chloride) is also important. In toxic drug-induced keratopathy, corneal epithelial damage appears more prominently than conjunctival epithelial damage. When severe, punctate superficial keratopathy spreads across the entire cornea and progresses to hurricane keratopathy and epithelial crack lines. Persistent epithelial defects may also occur. Long-term preservative load can lead to limbal dysfunction and ocular cicatricial pemphigoid.
Decreased corneal sensitivity leads to loss of the protective reflex, making epithelial damage more likely to progress. Trigeminal nerve damage due to reactivation of varicella-zoster virus (VZV) is a representative cause.
Gorgani et al. (2021) reported a case in which VZV reactivation of the trigeminal nerve presented with neurotrophic corneal ulcer and iridocyclitis, followed by the development of Ramsay-Hunt syndrome (facial nerve palsy)3). Spread of VZV from the trigeminal ganglion to the geniculate ganglion was suggested, and the complication of facial nerve palsy may further worsen neurotrophic keratopathy.
Corneal nerve damage due to diabetes also provides a basis for epithelial defects through a similar mechanism.
In entropion, the eyelashes come into contact with the cornea, causing persistent mechanical irritation that leads to epithelial defects.
Redd et al. (2022) reported a case of persistent epithelial defect in a newborn with congenital entropion5). Despite antibiotic treatment, the epithelial defect did not improve, and epithelialization was achieved one week after botulinum toxin correction of the entropion. This case demonstrates that correction of the underlying structural abnormality is essential for epithelial healing.
Limbal stem cell deficiency occurs in chemical trauma, Stevens-Johnson syndrome, ocular cicatricial pemphigoid, and other conditions, leading to persistent epithelial defects due to depletion of epithelial regenerative capacity. Corneal dystrophies (particularly map-dot-fingerprint dystrophy) form the basis for recurrent erosions.
Yes, contact lenses are a risk factor for corneal epithelial defects. Mechanical trauma during lens insertion and removal, hypoxia due to poor oxygen permeability, and toxicity from lens contamination can all cause epithelial damage. In particular, prolonged wear of soft contact lenses reduces corneal sensation, which may delay awareness of injury. Proper wearing time and hygiene management are important.
This is the most important test. Corneal epithelial defects are vividly stained green. Use the cobalt blue filter of a slit lamp microscope to evaluate the extent, shape, and depth of the defect. Differentiate from superficial punctate keratopathy (SPK) and check for poor epithelial adhesion around the erosion.
Normal corneal epithelium has a barrier function and does not allow fluorescein to penetrate. Late staining (Vaseline keratopathy) may be seen when the epithelial barrier function is impaired.
This is essential for diagnosing neurotrophic keratopathy. Use the Cochet-Bonnet corneal aesthesiometer for quantitative evaluation. If decreased corneal sensitivity is found, investigation of the cause of trigeminal nerve impairment is necessary.
Dry eye is often present as a basis for persistent epithelial defects. Evaluate tear secretion function using BUT (tear break-up time) and Schirmer test. Consider punctal plug insertion when tear secretion is markedly decreased.
Differentiation from infectious corneal ulcer is important. If stromal infiltration or hypopyon is present, manage as a corneal ulcer.
In unilateral or recurrent corneal epithelial lesions, always include corneal herpes (dendritic ulcer) in the differential diagnosis. Recurrent corneal epithelial erosion is easily misdiagnosed as corneal herpes.
The basic principles of treatment are removal of the cause and promotion of epithelial regeneration. The treatment strategy varies depending on the disease type.
Mild cases (small erosions) heal with artificial tears and observation alone. For moderate to severe cases, the following prescriptions are given to prevent infection and protect the epithelium.
| Medication | Dosage |
|---|---|
| Cravit ophthalmic solution 1.5% | 3 times daily |
| Hyalein ophthalmic solution 0.1% | 5 to 6 times daily |
| Tarivid eye ointment 0.3% | Before bedtime |
If pain is severe, oral Loxonin is added. Symptoms can be alleviated with a bandage soft contact lens (BCL) or an eye patch.
The acute phase is treated the same as simple erosion. The key is to start recurrence prevention once the epithelial erosion has healed. The following treatments are performed in stages.
(1) Ophthalmic ointment before bedtime and artificial tears upon waking
Apply Tarivid ophthalmic ointment before bedtime and instill Soft Santear upon waking. Instruct the patient to keep the eye drop bottle by the pillow and instill drops immediately after waking. Continue for at least 3 months, preferably 6 months, after erosion episodes have resolved.
(2) Use of therapeutic soft contact lenses
Continuous wear is important; replace the lens approximately every week. Disposable contact lenses may also be used.
(3) Surgical treatment
Considered when conservative treatment is ineffective. Since pain and inflammatory reactions occur immediately after the procedure, thorough explanation is necessary.
Treatment of the underlying condition (dry eye, neurotrophic keratopathy, lagophthalmos, etc.) is most important. Epithelial healing may not be achieved without correcting the causative structural abnormalities5).
Conservative treatment
Hyaluronate eye drops: Epithelial protection and promotion of wound healing
Autologous serum eye drops: Contain growth factors and vitamin A
Therapeutic SCL: Mechanical protection of the epithelium
Forced eyelid closure / Tarsorrhaphy: Ensuring corneal coverage
Surgical Treatment
Amniotic membrane transplantation: Anti-inflammatory and wound-healing promoting effects
Limbal transplantation: For limbal stem cell deficiency
Cultured epithelial sheet transplantation: Application of regenerative medicine
Conjunctival flap covering: For refractory ulcers and perforations
In persistent epithelial defects due to neurotrophic keratopathy, treatment that actively promotes wound healing in addition to epithelial protection is necessary. Basic epithelial protection with Tarivid eye ointment (0.3%) is combined with Hyalein ophthalmic solution (0.1%) and Mucosta ophthalmic solution UD (2%). If there is no response to pharmacotherapy, amniotic membrane transplantation or tarsorrhaphy is performed.
Simple small corneal erosions usually heal within 1 to 3 days. Even large epithelial defects often achieve epithelialization within one week if there is no underlying abnormality. However, when underlying conditions such as corneal hypoesthesia, dry eye, or limbal stem cell deficiency are present, healing may be delayed for weeks to months or longer. If epithelialization is not achieved within 2 weeks, further evaluation as a persistent epithelial defect is necessary.
The repair of corneal epithelial defects progresses through the following three stages.
Stage 1 (Extension and Migration Phase): When an epithelial defect occurs, fibronectin appears on the surface of the defect area. Epithelial cells around the defect extend and migrate over this fibronectin.
Stage 2 (Proliferation Phase): Once the defect is covered, proliferation and division of epithelial basal cells begins. The proliferated cells are gradually supplied to the defect area, and the epithelium recovers its thickness.
Stage 3 (Differentiation Phase): Through the period of cell differentiation, the regenerated epithelium normalizes.
Stem cells of the corneal epithelium are located in the limbus. Even if the entire corneal epithelium is lost, if the limbal epithelium is intact, it will repair the defect. The limbus also functions as a barrier that prevents conjunctival epithelium from invading the cornea.
When both the corneal epithelium and limbal epithelium are completely lost, the conjunctival epithelium covers the cornea. If Bowman’s layer is intact, conjunctival epithelialization of the cornea can occur. When Bowman’s layer is damaged or accompanied by vascular invasion, the conjunctival epithelium remains on the cornea while retaining its phenotype, requiring ocular surface reconstruction.
Corneal epithelial homeostasis is maintained when the sum of basal cell division (X) and limbal stem cell migration (Y) balances surface cell shedding (Z)1).
Cytotoxic anticancer drugs such as 5-FU suppress basal cell division (X). If administration continues without a drug holiday, the imbalance of X + Y < Z persists, resulting in corneal erosion1). Introducing a drug-free interval allows normal cells to recover1).
EGFR inhibitors cause epithelial damage through a different mechanism. EGF in tears plays a central role in maintaining corneal epithelial homeostasis via EGFR. EGFR inhibitors block this pathway, leading to impaired epithelial healing and thinning4).
The essence of recurrent erosion is poor adhesion between corneal epithelial basal cells and the basement membrane. Normally, epithelial basal cells are firmly attached to the basement membrane and Bowman’s layer via hemidesmosomes and anchoring fibrils. When this adhesion mechanism is disrupted by trauma or corneal dystrophy, the epithelium easily detaches and recurs.
This is a recombinant human nerve growth factor (NGF) ophthalmic solution. Efficacy has been demonstrated for neurotrophic corneal diseases. A protocol of 20 µg/mL administered 6 times daily for 8 weeks has been reported to achieve higher corneal healing rates compared to placebo.
This is attracting attention as a novel treatment for diabetic keratopathy. It has been reported to promote the proliferation and migration of corneal epithelial cells, and research toward clinical application is underway.
Combination therapy with substance P and IGF-1, fibronectin eye drops, and thymosin β4 have also been reported to be effective in selected cases, but all remain at the research stage.
Cultured corneal epithelial sheet transplantation is advancing toward practical use as a regenerative medicine approach for limbal stem cell deficiency. Cultured sheets derived from autologous oral mucosal epithelium have also been applied clinically.
- Tanaka H, Tabuchi H. Recurrent Corneal Erosion Induced by 1% 5-Fluorouracil Solution. Cureus. 2024;16(11):e73238. doi:10.7759/cureus.73238. PMID:39650961. PMCID:PMC11624916.
- Cope E, Radnor J, Beasley E. Perioperative Exposure Keratopathy and Corneal Abrasion in an Individual With Eyelash Extensions. Cureus. 2024;16(10):e72061.
- Gorgani FM, Beyer TL. Neurotrophic corneal ulcer and iridocyclitis directly preceding Ramsay-Hunt Syndrome. American journal of ophthalmology case reports. 2021;24:101220. doi:10.1016/j.ajoc.2021.101220. PMID:34786517; PMCID:PMC8578019.
- Dietze J, Mauger T. Combined Rothia dentocariosa and Streptococcus viridans Corneal Ulcer in an Immunocompromised Patient. Case Rep Ophthalmol Med. 2021;2021:9014667.
- Redd TK, Kersten RC, Ashraf D, Hennein L, Seitzman GD. Neonatal corneal ulcer secondary to congenital entropion. American journal of ophthalmology case reports. 2022;25:101371. doi:10.1016/j.ajoc.2022.101371. PMID:35169658; PMCID:PMC8829077.