Dry Keratoconjunctivitis
Schirmer test: ≤5 mm/5 min indicates decreased secretion.
BUT (tear break-up time): ≤5 seconds indicates unstable tear film.
Fluorescein staining: Punctate epithelial keratopathy of the inferior cornea and conjunctiva.

Rheumatoid arthritis (RA) is a chronic inflammatory autoimmune disease primarily affecting the synovial membrane of joints. It presents with various systemic symptoms involving the lungs, skin, eyes, and other organs, and is the most common among collagen diseases.
It commonly occurs in women aged 30–60 years, with a male-to-female ratio of approximately 1:3. In older-onset cases, the proportion of men increases. The prevalence in Japan is estimated to be about 0.5–1% of the population (approximately 600,000 to 1.2 million people).
Approximately 25–30% of RA patients have some ocular symptoms1). The frequency of ocular complications is associated with RA duration, disease activity, and the presence of extra-articular manifestations2).
Ocular complications associated with RA are classified into the following five types.
| Ocular complications | Frequency | Main features |
|---|---|---|
| Keratoconjunctivitis sicca (dry eye) | Most common | Often associated with Sjögren’s syndrome |
| Scleritis | Relatively common | Eye pain, deep injection, necrotizing form possible |
| Episcleritis | Relatively common | Superficial inflammation, tends to resolve spontaneously |
| Peripheral corneal ulcer | Relatively rare | Rapid corneal thinning and risk of perforation |
| Iridocyclitis | Rare | Anterior uveitis |
Malignant rheumatoid arthritis is a severe type accompanied by scleritis, pleuritis, interstitial pneumonia, pericarditis, myocarditis, multiple mononeuritis, mesenteric artery embolism, and fingertip ulcers, and has a poor prognosis.
Approximately 25–30% of patients have some ocular symptoms. The most common is dry eye (keratoconjunctivitis sicca), followed by scleritis and episcleritis. Peripheral corneal ulcers and necrotizing scleritis are relatively rare but are serious complications directly affecting visual prognosis.
Subjective symptoms vary depending on the type of ocular complication.
Dry Keratoconjunctivitis
Schirmer test: ≤5 mm/5 min indicates decreased secretion.
BUT (tear break-up time): ≤5 seconds indicates unstable tear film.
Fluorescein staining: Punctate epithelial keratopathy of the inferior cornea and conjunctiva.
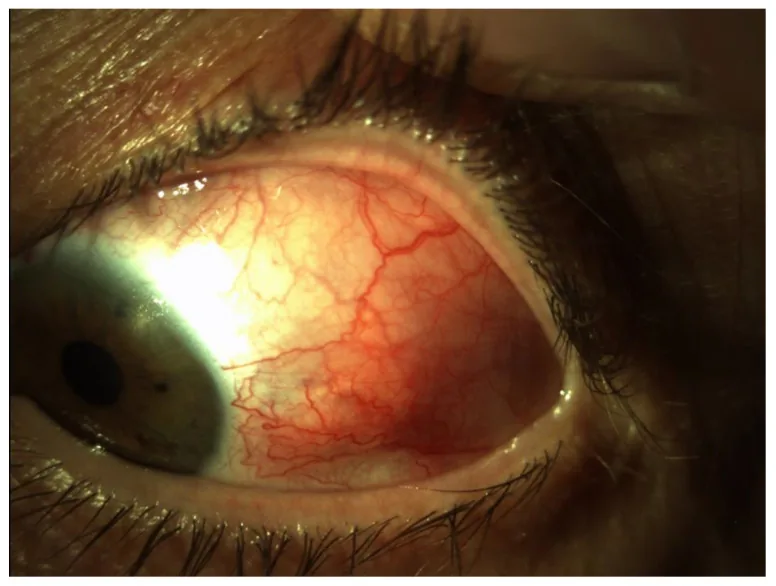
Scleritis
Episcleritis
Sectoral type: Fan-shaped congestion. Improves with topical NSAIDs.
Diffuse type: Widespread congestion. Often associated with RA.
Course: It may resolve spontaneously but can recur.
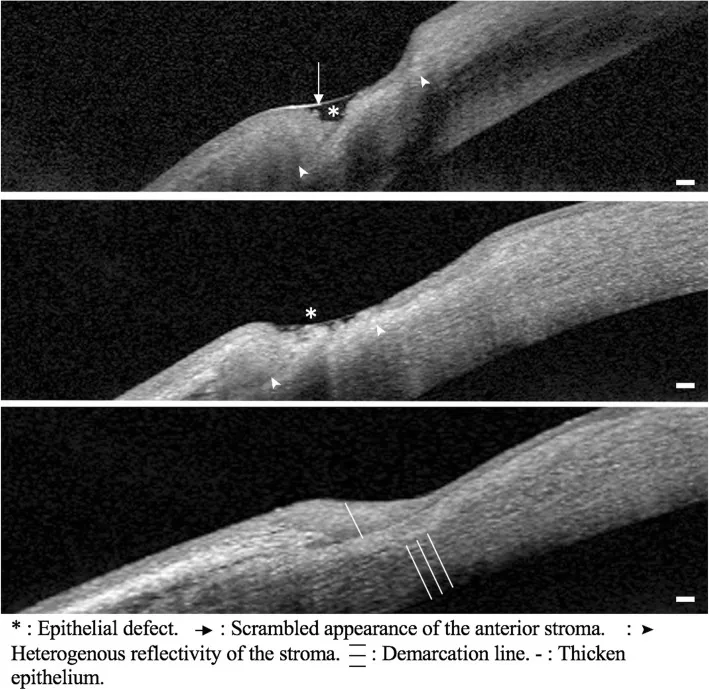
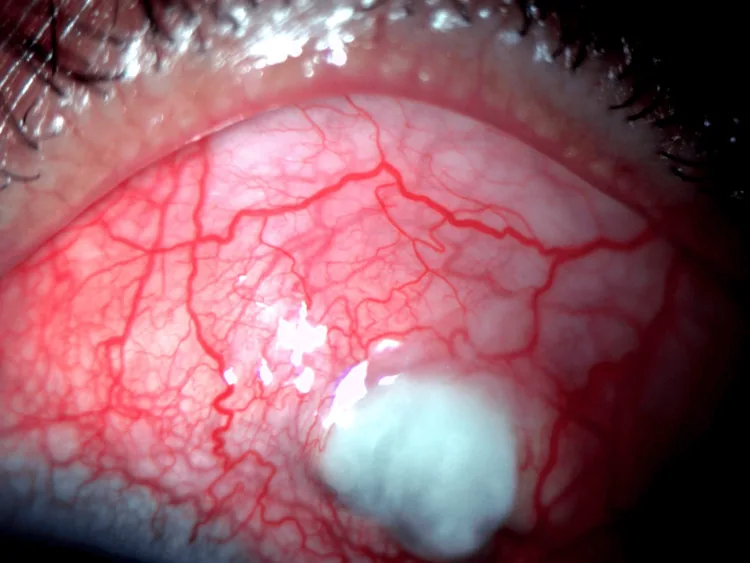
Peripheral Corneal Ulcer
Location: Groove-like thinning along the corneal limbus, 1–2 mm from the edge.
Progression: It expands circumferentially in a crescent shape and may rapidly lead to perforation.
Fluorescein staining: Positive fluorescein staining in the epithelial defect area.
Scleritis is classified according to the Watson classification into anterior scleritis (diffuse, nodular, necrotizing) and posterior scleritis, with necrotizing being the most severe 7). Approximately 30–50% of patients with scleritis have an associated systemic autoimmune disease, with RA being the most common 5).
Scleritis involves inflammation of the blood vessels in the sclera (deep layer of the white of the eye) and is accompanied by severe eye pain (deep, throbbing pain). The redness is dark red and does not easily disappear when pressure is applied to the blood vessels. Conjunctivitis presents with superficial redness that is bright red, with mild pain or a burning sensation, and the redness easily fades with pressure. If scleritis is suspected, prompt ophthalmological consultation is necessary.
Ocular involvement in RA results from systemic vasculitis and granulomatous inflammation due to autoimmune mechanisms spreading to the scleral and corneal limbal vessels11).
Patients who develop necrotizing scleritis or peripheral corneal ulcers have been reported to have a reduced 10-year survival rate 8), and these ocular lesions serve as indicators of systemic vasculitis activity.
The diagnosis of RA is based on the 2010 ACR/EULAR classification criteria 9). It scores four domains: number of swollen joints, serological tests (RF, anti-CCP antibodies), symptom duration, and acute-phase reactants (CRP, ESR).
In blood tests, elevated ESR, elevated CRP, positive RF (approximately 75%; negative in about 25%), anti-CCP antibodies, and elevated MMP-3 are useful for diagnosis 4). On X-ray, joint erosion and bone destruction in the hands and fingers are characteristic.
Evaluate ocular complications using the following tests.
| Examination method | Evaluation target | Criteria for findings |
|---|---|---|
| Schirmer test | Tear secretion volume | Decreased secretion if ≤5 mm/5 min |
| Tear Break-Up Time (BUT) | Tear film stability | Unstable if ≤5 seconds |
| Slit-lamp microscope | Sclera, cornea, anterior segment | Confirmation of necrotic changes and corneal thinning |
| Intraocular pressure measurement | Glaucoma / steroid response | Essential when using steroids |
| Fundus examination | Posterior scleritis, papilledema | Exclusion of posterior lesions |
| B-scan ultrasound | Posterior scleritis | T-sign (Tenon’s capsule edema) |
| Orbital MRI | Assessment of posterior scleritis extent | Scleral thickening and enhancement |
Posterior scleritis is easily overlooked and may present with eye pain, vision loss, proptosis, and diplopia. The T-sign on B-scan ultrasound is useful for diagnosis.
In patients with scleritis, systematic evaluation including RF, ANA, ANCA, complement, and chest X-ray is recommended as a workup for systemic diseases 5).
Regular ophthalmologic examinations are strongly recommended. Early detection and treatment of scleritis and peripheral corneal ulcers are directly linked to visual prognosis. Especially during periods of high RA disease activity or in malignant RA, ophthalmologic screening is important even in the absence of symptoms. Additionally, for patients using hydroxychloroquine, regular monitoring for retinal toxicity is necessary.
Treatment of ocular lesions in RA involves both local ophthalmic treatment and systemic treatment by internal medicine (rheumatology).
For mild to moderate dry keratoconjunctivitis, the following are applied stepwise.
In patients with Sjögren syndrome, dry eye tends to become severe, and the addition of cyclosporine eye drops may be considered.
| Severity | Treatment options |
|---|---|
| Mild | Oral NSAIDs (diclofenac sodium 75–100 mg/day, indomethacin 75 mg/day) |
| Moderate | Prednisolone 0.5–1 mg/kg/day orally. Taper after response. |
| Severe/necrotizing | Methylprednisolone 1 g/day IV pulse therapy for 3 days + immunosuppressant |
| Immunosuppressive drug indicated | Cyclophosphamide (2 mg/kg/day) or azathioprine (2 mg/kg/day) |
| Refractory | Biologic agents such as rituximab and tocilizumab |
| Scleral perforation | Superficial keratoplasty and scleral grafting using preserved cornea |
Nonsteroidal anti-inflammatory drugs may be effective for nodular and diffuse scleritis, but more aggressive immunosuppressive therapy is required for necrotizing scleritis6).
The following are applied as systemic treatment for RA4).
DMARDs (disease-modifying antirheumatic drugs):
Biologic DMARDs:
JAK inhibitors:
Steroids (such as prednisolone) carry risks of cataracts (posterior subcapsular cataracts), increased intraocular pressure, and glaucoma with long-term use, so regular ophthalmologic examinations are necessary. Paradoxical development of uveitis has been rarely reported with some biologic agents such as anti-TNF-α antibodies. Hydroxychloroquine (HCQ) can cause retinal toxicity (hydroxychloroquine retinopathy) when exceeding a certain dose, so annual ophthalmologic monitoring is recommended.
The onset of RA involves a combination of genetic predisposition (e.g., HLA-DR4/DR1) and environmental factors (e.g., smoking, protein citrullination by periodontal pathogens). Autoantibodies against citrullinated proteins (anti-CCP antibodies) are produced and deposited in the joints as immune complexes.
In the synovium, tissue destruction progresses through the following mechanisms.
Ocular lesions are a local manifestation of systemic vasculitis and immune reactions in RA 3).
Mechanism of scleritis:
Mechanism of marginal corneal ulcer:
Mechanism of dry keratoconjunctivitis (associated with Sjögren syndrome):
Scleritis and peripheral corneal ulcers are one of the extra-articular manifestations of RA, and they worsen and remit in parallel with systemic vasculitis activity. Suppression of RA disease activity with biologic agents or immunosuppressive drugs also contributes to improvement of ocular lesions 1).
The efficacy of rituximab (anti-CD20 antibody) 3) and tocilizumab (anti-IL-6 receptor antibody) for refractory scleritis and peripheral corneal ulcers has been reported in case reports and small-scale studies. Intensification of systemic RA treatment with biologics may contribute to improvement and suppression of recurrence of ocular complications.
Cases have been reported in which paradoxical uveitis (demyelinating uveitis-like reaction) develops during anti-TNF-α antibody administration4). Ophthalmologic monitoring before and after administration is necessary, and when inflammation worsens, the advisability of continuing administration should be reconsidered.
JAK inhibitors (tofacitinib, baricitinib, etc.) are becoming widely used as systemic treatments for RA, and research is progressing on their effects on ocular inflammation such as scleritis. The JAK-STAT pathway is involved in ocular inflammation mediated by IL-6 and IFN-γ signaling, and local ocular application is expected.
For perforated cases of severe peripheral corneal ulcers, cell engineering approaches such as amniotic membrane transplantation, artificial cornea, and cultured corneal stromal cell transplantation have been attempted. Evaluating long-term outcomes remains a challenge.
Sainz de la Maza M, Molina N, Gonzalez-Gonzalez LA, Doctor PP, Tauber J, Foster CS. Clinical characteristics of a large cohort of patients with scleritis and episcleritis. Ophthalmology. 2012;119(1):43-50. doi:10.1016/j.ophtha.2011.07.013. PMID:21963265.
Galor A, Thorne JE. Scleritis and peripheral ulcerative keratitis. Rheum Dis Clin North Am. 2007;33(4):835-854. doi:10.1016/j.rdc.2007.08.002.
Artifoni M, Rothschild PR, Brézin A, et al. Ocular inflammatory diseases associated with rheumatoid arthritis. Nat Rev Rheumatol. 2014;10(2):108-116. doi:10.1038/nrrheum.2013.185.
日本リウマチ学会 編. 関節リウマチ診療ガイドライン2020. メディカルレビュー社; 2021.
Akpek EK, Thorne JE, Qazi FA, Do DV, Jabs DA. Evaluation of patients with scleritis for systemic disease. Ophthalmology. 2004;111(3):501-506. doi:10.1016/j.ophtha.2003.06.006. PMID:15019326.
Jabs DA, Mudun A, Dunn JP, Marsh MJ. Episcleritis and scleritis: clinical features and treatment results. American journal of ophthalmology. 2000;130(4):469-76. doi:10.1016/s0002-9394(00)00710-8. PMID:11024419.
P. G. Watson, S. S. Hayreh. Scleritis and episcleritis. British Journal of Ophthalmology. 1976;60(3):163-191. doi:10.1136/bjo.60.3.163.
Foster CS, Forstot SL, Wilson LA. Mortality rate in rheumatoid arthritis patients developing necrotizing scleritis or peripheral ulcerative keratitis. Effects of systemic immunosuppression. Ophthalmology. 1984;91(10):1253-1263. doi:10.1016/s0161-6420(84)34160-4.
Aletaha D, Neogi T, Silman AJ, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569-2581.
Messmer EM, Foster CS. Vasculitic peripheral ulcerative keratitis. Survey of ophthalmology. 1999;43(5):379-96. doi:10.1016/s0039-6257(98)00051-4. PMID:10340557.
Smith JR, Mackensen F, Rosenbaum JT. Therapy insight: scleritis and its relationship to systemic autoimmune disease. Nature clinical practice. Rheumatology. 2007;3(4):219-26. doi:10.1038/ncprheum0454. PMID:17396107.
Bongartz T, Sutton AJ, Sweeting MJ, et al. Anti-TNF antibody therapy in rheumatoid arthritis and the risk of serious infections and malignancies: systematic review and meta-analysis of rare harmful effects in randomized controlled trials. JAMA. 2006;295(19):2275-2285. doi:10.1001/jama.295.19.2275.