Immune checkpoint inhibitors (ICIs) are monoclonal antibodies that inhibit checkpoint molecules, which act as brakes on T cells, thereby enhancing the immune response against cancer cells1). While they have revolutionized cancer treatment, they also cause immune-related adverse events (irAEs), which are non-specific inflammation in tissues other than tumors1).
CTLA-4 controls T cell activation in lymph nodes, while PD-1 suppresses T cell responses in peripheral tissues1). Inhibition of these pathways enhances antitumor immunity but can also trigger autoimmune reactions. ICIs are a significant cause of drug-induced uveitis4,5).
The incidence of ocular irAEs is 1–3%1). Posterior segment inflammation (retina and choroid) accounts for approximately 5–20% of all ocular irAEs, but it is often severe and can lead to permanent vision loss if not managed appropriately1). As the approved indications for ICIs expand, awareness among both ophthalmologists and oncologists is becoming increasingly important.
QHow often do ocular side effects of immune checkpoint inhibitors occur?
A
Ocular irAEs occur in 1–3% of all cases1). The incidence varies by drug type: approximately 1% with CTLA-4 monotherapy, 0.3–0.6% with PD-1 monotherapy, and a 2–3 times higher risk with combination therapy4). Most cases are dry eye or anterior uveitis, but posterior segment inflammation (5–20% of all ocular irAEs) can be a serious complication affecting visual prognosis.
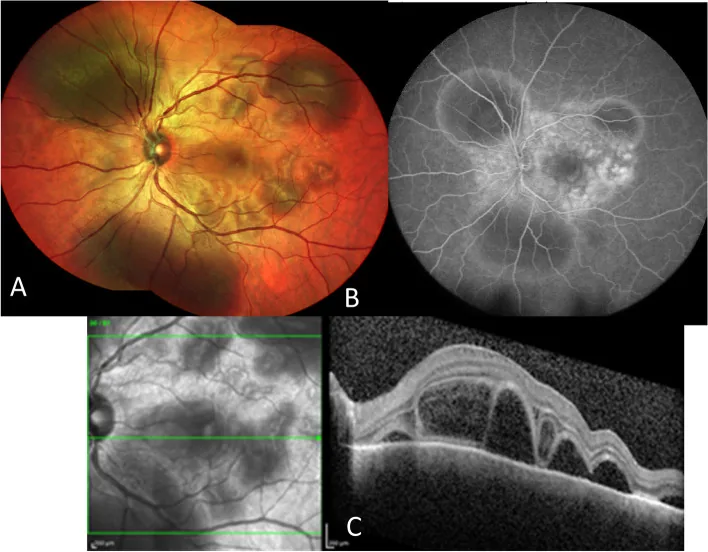
Paez-Escamilla M, et al. Challenges in posterior uveitis-tips and tricks for the retina specialist. J Ophthalmic Inflamm Infect. 2023. Figure 1. PMCID: PMC10435440. License: CC BY.
Fundus photograph shows yellowish-white lesions and serous retinal detachment. Multiple leakages on fluorescein angiography and multiloculated serous retinal detachment on OCT indicate posterior inflammation in immune checkpoint inhibitor-associated uveitis.
Uveitis primarily presents with hyperemia, blurred vision, photophobia, and eye pain. Posterior segment inflammation leads to decreased visual acuity, floaters, and metamorphopsia1). Orbital myositis manifests as diplopia, ptosis, and proptosis2). Dry eye is mainly characterized by dryness and foreign body sensation.
ICI-related ocular irAEs can occur in almost all areas of the eye.
Anterior Segment and Ocular Surface
Dry eye (most frequent): PD-1/PD-L1 inhibitors may cause Sjögren’s syndrome-like tear secretion reduction.
Anterior uveitis: Anterior chamber inflammatory cells and flare. Accounts for 30–40% of all ocular irAEs. Many cases respond to steroid eye drops7).
Corneal erosion: May appear as part of Behçet’s-like syndrome.
Posterior Segment
VKH-like panuveitis: Exudative retinal detachment and optic disc edema. Occurs in 5–14% of melanoma ICI patients1). The mechanism involves cross-reactivity with melanin-containing cells.
Retinal vasculitis: vascular leakage, macular edema, arteriovenous occlusion. Occurs in 5–10% of all ocular irAEs4).
Orbital myositis (most common with anti-CTLA-4): tends to appear bilaterally. MRI shows enlargement and contrast enhancement of extraocular muscles2).
Orbital fat inflammation: may extend to the orbital apex and superior orbital fissure2).
Thyroid eye disease-like inflammation: Can occur even in patients with normal thyroid function.
Neurological
Ocular myasthenia gravis: Associated with anti-AChR antibody production. Reported with pembrolizumab9).
Optic neuritis: Early steroid treatment can preserve vision8).
Abducens nerve palsy: Often improves with drug discontinuation plus high-dose steroids8).
The onset of orbital inflammation ranges from 2 days to 2 months after the first dose2). Caution is needed for severe cases when combined with systemic irAEs (myositis, myocarditis, colitis).
The root cause of ocular irAEs induced by ICIs is the triggering of autoimmune reactions due to the release of T-cell immune checkpoints1).
CTLA-4 inhibition: Releases the brake controlling T-cell activation, allowing attacks on normal tissues1)
PD-1/PD-L1 inhibition: Directly disrupts PD-L1-dependent immune privilege in ocular tissues1)
CTLA-4 + PD-1 combination: The risk of ocular irAE increases 2–3 times compared to monotherapy4)
Melanoma patients: Cross-reactivity between melanin-containing ocular tissues (choroid, RPE) and tumor antigens leads to a high risk of VKH-like panuveitis1, 10)
Pre-existing BRB disruption: Conditions such as diabetic retinopathy with pre-existing blood-retinal barrier disruption increase risk1)
Host genetic predisposition: Involvement of HLA types such as HLA-DR15 has been suggested7)
QWhy do immune checkpoint inhibitors cause ocular inflammation?
A
ICIs activate T cells by releasing immune checkpoints to attack cancer, but they also disrupt the PD-L1-dependent immune privilege of ocular tissues1). The pathological mechanisms are classified into three types (see Section 6): (1) cross-reactivity between anti-tumor T cells and melanin-containing ocular tissues (VKH-like reaction), (2) retinal vasculitis due to bystander effects, and (3) autoantibody-mediated inflammation.
The diagnosis of ICI-related ocular irAE is based on the temporal association between ICI use and ocular findings. The diagnostic principle is to perform basic uveitis screening, confirm the temporal relationship between the suspected drug use and symptom onset, and exclude other causes3).
In anterior uveitis, differentiation from infectious and non-infectious uveitis is necessary. VKH-like reactions are clinically similar to primary VKH, but a history of ICI use for melanoma is an important clue 1, 10). Orbital myositis requires differentiation from thyroid eye disease, IgG4-related disease, and idiopathic orbital inflammation2). MAR (melanoma-associated retinopathy)-like retinopathy requires differentiation from paraneoplastic syndromes 1). Infectious uveitis and metastatic intraocular tumors (masquerade syndromes) are also included in the exclusion criteria.
Treatment is individualized based on CTCAE Grade in consultation between the medical oncologist and ophthalmologist. In severe cases, interruption of ICI may be considered, but since the antitumor effect is directly linked to life, the decision to discontinue or resume should be made carefully by a multidisciplinary team.
Complicated by myasthenia gravis: consider plasma exchange therapy9)
Orbital inflammation: most cases improve with systemic steroids, but some cases present with residual diplopia2)
QDo I have to stop medication for ICI uveitis?
A
Discontinuation of ICI is rarely necessary. For Grade 1–2, it is often possible to manage with steroid eye drops or local injections while continuing ICI. For Grade 3 or higher (≥2-step decrease in vision, panuveitis), consider systemic steroids and ICI interruption 5). For Grade 4 with risk of blindness, resumption may be difficult. Decisions to discontinue or resume must always be made in consultation with the oncologist.
QCan ICI be resumed after developing uveitis?
A
After inflammation is sufficiently controlled (Grade 1 or lower), resumption may be considered in consultation with the oncologist. However, for severe ocular irAEs such as VKH-like panuveitis, the risk of recurrence is high, and the decision to resume should be made on a case-by-case basis. After resumption, close ophthalmologic follow-up is necessary6).
Haliyur et al. (2025) classified ICI-induced posterior segment irAE into three types1).
Type 1: T-cell cross-reactivity
Type 1a: Antitumor T cells cross-react with ocular tissues such as melanin-containing cells, triggering VKH-like panuveitis. It occurs in 5–14% of melanoma patients1).
Type 1b: Eye-specific tissue-resident memory T cells are expanded and activated by ICI, causing autoimmune retinopathy1).
Type 2: Bystander vasculitis
Systemic inflammation enhancement associated with ICI use nonspecifically disrupts the blood-retinal barrier1).
Perivascular lymphoplasmacytic infiltration by CD4+ T cells and increased expression of adhesion molecules cause retinal vasculitis and arteriovenous occlusion1).
Type 3: Autoantibody-mediated
PD-1 is also expressed on B cells, and ICIs induce expansion of B cell lineages and production of tissue-specific autoantibodies from plasma cells1).
It is also involved in exacerbation of paraneoplastic syndromes (such as MAR-like retinopathy)1).
Clinical findings are not limited to a single mechanism; multiple mechanisms may overlap. VKH-like panuveitis (Type 1a) presents with exudative retinal detachment and choroidal hyperfluorescence, and may be clinically difficult to distinguish from Harada disease1).
Anti-CTLA-4 inhibitors (ipilimumab) most frequently cause orbital inflammation2). Similar clinical presentations have been reported with anti-PD-1/PD-L1 inhibitors2). MRI shows enlargement and contrast enhancement of extraocular muscles and inflammatory changes in orbital fat, with a tendency to appear bilaterally2).
The application of IL-6 receptor antibody (tocilizumab) to steroid-resistant irAE has been reported6)
The development of intraocular tumor therapy using a combination of ICI and anti-VEGF agents is also attracting attention
Quantification of irAE incidence and treatment outcomes through prospective multicenter registries is urgently needed6)
Currently, understanding of the pathophysiology of posterior segment irAE is mainly based on case reports and case series, and diagnostic criteria and treatment guidelines have not been established1). There is an urgent need to develop collaboration protocols between oncology and ophthalmology departments.
Haliyur R, Elner SG, Sassalos T, Kodati S, Johnson MW. Pathogenic Mechanisms of Immune Checkpoint Inhibitor (ICI)-Associated Retinal and Choroidal Adverse Reactions. American journal of ophthalmology. 2025;272:8-18. doi:10.1016/j.ajo.2024.12.028. PMID:39755350.
Terence Ang, Viraj Chaggar, Jessica Y. Tong, Dinesh Selva. Medication-associated orbital inflammation: A systematic review. Survey of Ophthalmology. 2024;69(4):622-631. doi:10.1016/j.survophthal.2024.03.003.
Dalvin LA, Shields CL, Orloff M, Sato T, Shields JA. CHECKPOINT INHIBITOR IMMUNE THERAPY: Systemic Indications and Ophthalmic Side Effects. Retina. 2018;38(6):1063-1078. doi:10.1097/iae.0000000000002181. PMID:29689030.
Brahmer JR, Abu-Sbeih H, Ascierto PA, Brufsky J, Cappelli LC, Cortazar FB, Gerber DE, Hamad L, Hansen E, Johnson DB, Lacouture ME, Masters GA, Naidoo J, Nanni M, Perales MA, Puzanov I, Santomasso BD, Shanbhag SP, Sharma R, Skondra D, Sosman JA, Turner M, Ernstoff MS. Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immune checkpoint inhibitor-related adverse events. J Immunother Cancer. 2021;9(6):e002435. doi:10.1136/jitc-2021-002435. PMID:34172516; PMCID:PMC8237720.
Fortes BH, Liou H, Dalvin LA. Ophthalmic adverse effects of immune checkpoint inhibitors: the Mayo Clinic experience. Br J Ophthalmol. 2021;105(8):1108-1113.
Bitton K, Michot JM, Barreau E, Lambotte O, Haigh O, Marabelle A, Voisin AL, Mateus C, Rémond AL, Couret C, Champiat S, Labetoulle M, Rousseau A. Prevalence and Clinical Patterns of Ocular Complications Associated With Anti-PD-1/PD-L1 Anticancer Immunotherapy. Am J Ophthalmol. 2019;202:109-117. doi:10.1016/j.ajo.2019.02.012. PMID:30772350.
Matas-García A, Milisenda JC, Selva-O’Callaghan A, et al. Ocular myasthenia gravis and myositis following immune checkpoint inhibitor therapy. Neurology. 2020;95(14):e1672-e1680.
Schulz TU, Urner J, Seegräber M, et al. Immune checkpoint inhibitor-induced Vogt-Koyanagi-Harada-like syndrome: a case report and review of literature. Ocul Immunol Inflamm. 2022;30(3):731-741.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.