Non-specific acute to subacute inflammatory lesions that are not infectious often occur in orbital tissues. This condition is characterized by simultaneously meeting the following three criteria:
Pathologically non-specific — no specific cause can be identified
Unresponsive to antibiotics — difficult to identify an infectious source
Corticosteroids are highly effective
This condition was previously called “orbital inflammatory pseudotumor.” It was named in an older era because it causes proptosis and eyelid swelling as if a tumor had formed. This term dates from a time when diagnostic imaging was limited; now that MRI makes it relatively easy to identify inflammatory lesions, the term is considered inappropriate and is being replaced by the diagnosis idiopathic orbital inflammation (IOI)1).
The most common primary orbital tumors are lymphoproliferative disorders, accounting for 50–60% of all orbital tumors. This group includes malignant lymphoma, reactive lymphoid hyperplasia, IgG4-related ophthalmic disease (IgG4-ROD), and idiopathic orbital inflammation. IOI is reported to account for approximately 8–10% of all orbital mass lesions 1,2).
In recent years, with the establishment of IgG4-related ophthalmic disease as an independent entity, cases previously included in IOI have been reclassified, and the disease concept of IOI has been narrowed and refined. Current IOI refers to “true nonspecific inflammation” that remains after excluding these specific diseases 3,4).
QAre "orbital pseudotumor" and "idiopathic orbital inflammation" the same disease?
A
Essentially, they refer to the same condition. “Orbital inflammatory pseudotumor” is an older term from an era when diagnostic imaging was limited, named because it causes proptosis like a tumor. Now that MRI can detect inflammatory lesions, it is being replaced by “idiopathic orbital inflammation.” However, in recent years, IgG4-related ophthalmic disease and MALT lymphoma have been separated as independent diseases, so the disease concept has become narrower than before.
Onset is often acute to subacute, presenting with the following symptoms.
Eyelid swelling and redness: Swelling and redness of the affected eyelid
Proptosis: Due to increased orbital content
Globe displacement: The eyeball is pushed out depending on the lesion location
Ocular motility disorder and diplopia: Especially prominent in the extraocular muscle type and apical type
Pain: Severe pain in the orbital apex type and myositic type
Visual loss: Occurs in the orbital apex type due to compression or infiltration of the optic nerve
Lesions rarely spread diffusely within the orbit; they often center on the lacrimal gland, extraocular muscles, periorbital area, or orbital apex, and tend to spread with relatively indistinct borders.
Based on CT/MRI findings, inflammation is classified into five types according to the site of origin: anterior orbital type, diffuse type, orbital apex type, myositic type, and lacrimal gland type1,2).
Orbital Apex Type
Common site: Orbital apex (around the optic canal and superior orbital fissure)
Main symptoms: Decreased vision, severe pain, and eye movement disorder
Notes: The most severe of the five types. High risk of optic nerve damage due to proximity to the optic nerve. Differentiation from infection (especially fungal) is essential.
Main symptoms: Eye movement disorder, diplopia. Pain during eye movement.
Notes: Selectively affects extraocular muscles. Good prognosis. Differentiation from thyroid eye disease is important (involvement of tendon insertions is a distinguishing feature).
Lacrimal Gland Type
Common site: Lacrimal gland
Main symptoms: Swelling and pain in the lacrimal gland area. Swelling of the outer eyelid.
Notes: Differentiation from IgG4-related ophthalmic disease (IgG4-ROD) is most important. IgG4-ROD is often painless and bilateral.
The characteristics of each localized type are shown below.
Type
Common site
Main symptoms
Notes
Anterior orbital type
Periocular area
Eyelid swelling, conjunctival injection
—
Diffuse type
Orbital fat tissue
Proptosis
Diffuse lesion. Rare.
Apical type
Orbital apex
Vision loss, severe pain
Most severe. Differentiation from infection is essential.
Chronic type (idiopathic sclerosing orbital inflammation): Lesions with extensive fibrosis. Poor steroid response and refractory.
QWhich type of idiopathic orbital inflammation is most severe?
A
The orbital apex type is the most severe. Due to proximity to the optic nerve, there is a high risk of vision loss and severe pain. The chronic type (idiopathic sclerosing orbital inflammation) has poor steroid response and is refractory due to extensive fibrosis. The myositic type localized to extraocular muscles generally has a good prognosis.
Among primary orbital tumors, lymphoproliferative disorders (including malignant lymphoma, reactive lymphoid hyperplasia, IgG4-related ophthalmic disease, and IOI) are the most common, accounting for 50–60% of all orbital tumors. Among them, idiopathic orbital inflammation is one of the representative benign orbital diseases in adults.
As a result of the establishment of IgG4-related ophthalmic disease as an independent entity, some cases previously diagnosed as IOI have been reclassified, and the frequency of pure IOI is decreasing. International reports indicate a predilection for middle-aged adults (40s–60s), but detailed epidemiological data within Japan are limited. Large-scale data showing a consistent trend regarding sex differences are also lacking.
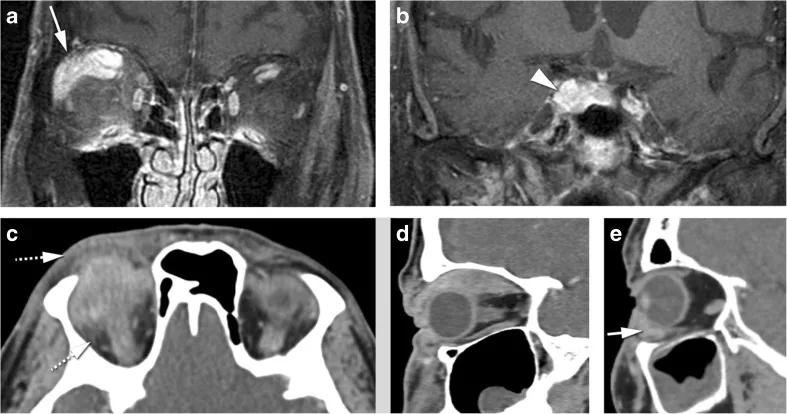
Ferreira TA, Saraiva P, Genders SW, et al. CT and MR imaging of orbital inflammation. Neuroradiology. 2018;60(12):1253–1266. Figure 8. PMCID: PMC6244997. DOI: 10.1007/s00234-018-2103-4. License: CC BY 4.0.
Coronal contrast-enhanced T1-weighted MRI (a, b) shows multifocal enhancement of the levator palpebrae superioris–superior rectus complex and lacrimal gland in the right orbit, confirming diffuse orbital inflammation. Sagittal CT (d) shows continuous contrast enhancement (tubular pattern) from the belly to the tendinous insertion of the superior rectus muscle, corresponding to myositis involving the tendinous insertion (a distinguishing feature from thyroid eye disease) discussed in section “4. Diagnosis and Differential Diagnosis.”
When acute to subacute eyelid swelling, proptosis, and globe displacement are observed, CT and MRI imaging should be performed.
MRI T2-weighted STIR sequence: Inflammatory lesions appear as high signal. Excellent for evaluating the localization of inflammation.
MRI T1-weighted gadolinium-enhanced with fat suppression: Inflammatory lesions appear as high signal areas. Useful for assessing the extent of the lesion.
CT: Used to evaluate the localization pattern of intraorbital lesions (confirmation of the 5-type classification), presence of bone destruction, and sinus involvement.
Histopathological findings of nonspecific inflammation
No response to antibiotics
Excellent response to steroids
Clinically, when idiopathic orbital inflammation is suspected on imaging, a trial of steroid therapy is administered; if there is an excellent response, the clinical diagnosis is generally confirmed.
Biopsy during the acute phase or before treatment is generally avoided because it can easily cause sequelae such as ocular motility disorders after treatment. However, biopsy should be considered in the following cases:
In particular, differentiation from infectious diseases (orbital cellulitis) and malignant diseases (MALT lymphoma) is important. In a report by Aryasit et al. (2021), IgG4-positive plasma cell infiltration was confirmed in the tissues of 21 out of 45 cases (46.7%) initially diagnosed as IOI, and histological reassessment and IgG4 immunostaining are strongly recommended4).
Indolent course. Diagnosis confirmed by biopsy. IgH gene rearrangement testing.
Rupture of paranasal sinus cyst
Acute onset. CT imaging shows sinus lesion.
Infectious diseases such as orbital cellulitis and intraorbital rupture of a paranasal sinus cyst are important differential diagnoses as they cause acute eyelid swelling, proptosis, and globe displacement. Differential diagnosis is made using blood tests and imaging such as CT. Subacute progressive orbital diseases include specific orbital inflammatory diseases such as thyroid eye disease and granulomatosis with polyangiitis.
QHow is idiopathic orbital inflammation distinguished from thyroid eye disease?
A
Thyroid eye disease is a condition in which the extraocular muscles enlarge in the setting of thyroid dysfunction (e.g., Graves’ disease). A characteristic imaging finding is that only the muscle belly is enlarged while the tendon insertion is spared. In IOI, thyroid function is normal, and inflammation diffusely involves the extraocular muscles including the tendon insertions. Differentiation is made by combining blood tests (thyroid hormones, TSH receptor antibodies) and imaging findings.
First-line treatment is oral steroid therapy. However, if symptoms such as pain are not severe, spontaneous remission may occur, so observation is also an option.
Before starting steroids, it is essential to sufficiently rule out infection (especially fungal infection of the orbital apex).
Start with prednisolone 0.25–1.0 mg/kg/day, then taper gradually with the goal of discontinuing within 3–6 months1,3). Relapse during tapering is common. Rapid tapering increases the risk of relapse, so it is important to taper slowly over a sufficient period.
A prescription example is shown below.
Drug
Dosage and administration
Notes
Prednisone 5 mg tablets
6 tablets daily in 2 divided doses (4 in the morning, 2 at noon, after meals)
Taper according to progress. Aim to discontinue within 3–6 months.
Caster D 10 mg tablets (alfacalcidol)
2 tablets daily in 2 divided doses (after breakfast and dinner)
Used concomitantly to prevent steroid-induced osteoporosis.
The following treatments may be tried for refractory cases with repeated relapses.
Steroid pulse therapy: High-dose intravenous methylprednisolone infusion. Indicated for severe cases or apical orbital type with impending optic neuropathy.
Radiation therapy: An option for refractory cases with repeated recurrence. Appropriate dosing requires evaluation at a specialized facility.
Methotrexate: Used as an immunosuppressant to reduce or discontinue steroids (off-label). In a study of 14 cases by Smith et al. (2001), 71% completed a 4-month trial, and clinical efficacy was reported in 64% 5).
Response to steroids is generally good. With adequate treatment, many cases can be controlled without recurrence. However, rapid tapering may lead to recurrence, so careful follow-up is necessary. Cases localized to the extraocular muscles (idiopathic orbital myositis) generally have a favorable prognosis. Rarely, some cases become persistent and refractory.
QWhy does recurrence occur when steroids are reduced?
A
This disease is a nonspecific inflammation of unknown cause. Steroids suppress inflammation but do not eliminate the underlying cause. Therefore, inflammation tends to flare up with tapering. Gradual tapering over 3 to 6 months is important to prevent recurrence. In refractory or frequently recurring cases, consider switching to radiation therapy or immunosuppressants.
6. Pathophysiology and Detailed Mechanism of Onset
The etiology of idiopathic orbital inflammation is unknown. It is considered a nonspecific inflammation of orbital tissues of unknown cause.
Histologically, it shows nonspecific inflammatory cell infiltration (mainly lymphocytes and plasma cells). No specific causative microorganism or specific autoantibodies have been identified, but an autoimmune mechanism is suspected.
Inflammation rarely spreads diffusely within the orbit; it often occurs in specific sites such as the lacrimal gland, extraocular muscles, peribulbar region, and orbital apex, spreading with relatively indistinct borders. The mechanism of this site selectivity remains largely unknown.
Idiopathic sclerosing orbital inflammation is a chronic subtype with extensive fibrosis. The main features are fibroblast activation and excessive collagen deposition, leading to poor steroid response and poor prognosis.
Historically, the group of lesions collectively called “orbital pseudotumor” has been separated into IgG4-related ophthalmic disease and MALT lymphoma as distinct entities, and the remaining nonspecific inflammation is now classified as IOI in the narrow sense. Current IOI refers to the concept of “true nonspecific inflammation” that remains after excluding these specific diseases.
Differentiation from reactive lymphoid hyperplasia is also a challenge, and especially since IgG4-related ophthalmic disease was established as an independent entity, most lymphoproliferative lesions have been reclassified as IgG4-ROD or MALT lymphoma.
With the establishment of IgG4-related disease as an independent entity, the disease concept of IOI has been narrowed and refined. Advances in molecular biological techniques (flow cytometry, immunohistochemistry, IgH gene rearrangement testing, etc.) have enabled more precise differentiation and classification of cases previously categorized as IOI. Identification of molecular markers that may elucidate the etiology of IOI is expected in the future.
Treatment Development for Sclerosing Orbital Inflammation
Idiopathic sclerosing orbital inflammation (sclerosing variant) often shows steroid resistance and is difficult to treat. Evidence is accumulating on the efficacy of immunosuppressive agents such as methotrexate and mycophenolate mofetil.
Biologic agents such as rituximab (anti-CD20 antibody) have been tried in refractory cases of IOI. In a phase 1/2 randomized clinical trial by Suhler et al. (2014), improvement at 24 weeks was confirmed in 7 of 10 cases of steroid- and other immunosuppressant-resistant orbital inflammation, and successful steroid tapering was achieved 6). However, there is diagnostic overlap with IgG4-ROD, and large-scale evidence for IOI alone is still accumulating. Verification of efficacy through future clinical studies is necessary.
Yeşiltaş YS, Gündüz AK. Idiopathic Orbital Inflammation: Review of Literature and New Advances. Middle East Afr J Ophthalmol. 2018;25(2):71-80. PMID: 30122852. PMCID: PMC6071347. DOI: 10.4103/meajo.MEAJO_44_18.
Espinoza GM. Orbital inflammatory pseudotumors: etiology, differential diagnosis, and management. Curr Rheumatol Rep. 2010;12(6):443-447. PMID: 20803107. DOI: 10.1007/s11926-010-0128-8.
Fang Y, Shen B, Dai Q, et al. Orbital inflammatory pseudotumor: new advances in diagnosis, pathogenesis, and treatment. Eur J Med Res. 2023;28(1):395. PMID: 37794419. PMCID: PMC10548690. DOI: 10.1186/s40001-023-01330-0.
Aryasit O, Tiraset N, Preechawai P, et al. IgG4-related disease in patients with idiopathic orbital inflammation. BMC Ophthalmol. 2021;21(1):356. PMID: 34625052. PMCID: PMC8499436. DOI: 10.1186/s12886-021-02115-x.
Smith JR, Rosenbaum JT. A role for methotrexate in the management of non-infectious orbital inflammatory disease. Br J Ophthalmol. 2001;85(10):1220-1224. PMID: 11567968. PMCID: PMC1723732. DOI: 10.1136/bjo.85.10.1220.
Suhler EB, Lim LL, Beardsley RM, et al. Rituximab therapy for refractory orbital inflammation: results of a phase 1/2, dose-ranging, randomized clinical trial. JAMA Ophthalmol. 2014;132(5):572-578. PMID: 24652467. PMCID: PMC4321949. DOI: 10.1001/jamaophthalmol.2013.8179.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.