Proptosis
Features: Slowly progressive, unilateral, painless
Pattern: Axial proptosis is typical due to the intraconal location of the mass.
Measurement: Assess asymmetry using the Hertel exophthalmometer.

Orbital cavernous hemangioma is a benign tumor derived from vascular endothelium and is the most representative benign orbital tumor in adults. It forms a well-circumscribed solid mass encapsulated within a capsule, commonly occurring within the muscle cone (the cone-shaped space formed by the extraocular muscles in the orbit).
Histologically, hemangiomas are classified into pleomorphic hemangioma, where all components of the vessel wall become neoplastic, and monomorphic hemangioma, where only one component becomes neoplastic. Cavernous hemangioma belongs to the monomorphic type and is composed of cavernous vascular spaces.
From an age distribution perspective, different vascular orbital tumors are common at different ages. Capillary hemangioma is most frequent in infancy, and lymphangioma is often seen in childhood. In contrast, cavernous hemangioma commonly occurs in adults, particularly in their 30s to 50s. There is a slight female predominance, with a reported male-to-female ratio of approximately 1:1.4 to 1:2.
In recent revisions of the International Society for the Study of Vascular Anomalies (ISSVA) classification, there is a proposal to reclassify cavernous hemangioma, previously categorized as a “tumor,” as a low-flow vascular malformation (venous malformation) [1,7]. However, the term “cavernous hemangioma” is still widely used in clinical practice, so this article adopts that name.
It is a benign tumor, and malignant transformation is extremely rare. It is a well-circumscribed mass with a capsule and does not invade surrounding tissues. The vast majority of hemangiomas are histologically benign, but rarely some may show malignant features such as recurrence or destruction of surrounding tissues. Appropriate diagnosis and treatment selection improve prognosis. Recurrence after complete resection is extremely rare, and the prognosis is generally favorable.
Orbital cavernous hemangioma grows slowly, and symptoms progress gradually over months to years. Rapid enlargement is rare, but can occur when intratumoral hemorrhage happens.
Typical subjective symptoms are as follows:
Note that many cases are discovered incidentally on imaging without symptoms. In such cases, observation is the basic management.
The amount of proptosis is measured with a Hertel exophthalmometer. Fundus examination may reveal choroidal folds due to compression of the eyeball wall by the mass.
Proptosis
Features: Slowly progressive, unilateral, painless
Pattern: Axial proptosis is typical due to the intraconal location of the mass.
Measurement: Assess asymmetry using the Hertel exophthalmometer.
Decreased visual acuity and diplopia
Decreased visual acuity: Caused by compression of the optic nerve. Prominent in orbital apex tumors.
Diplopia: Caused by compression and displacement of extraocular muscles.
Course: Often slowly progressive. Rapid worsening suggests intratumoral hemorrhage.
Imaging features
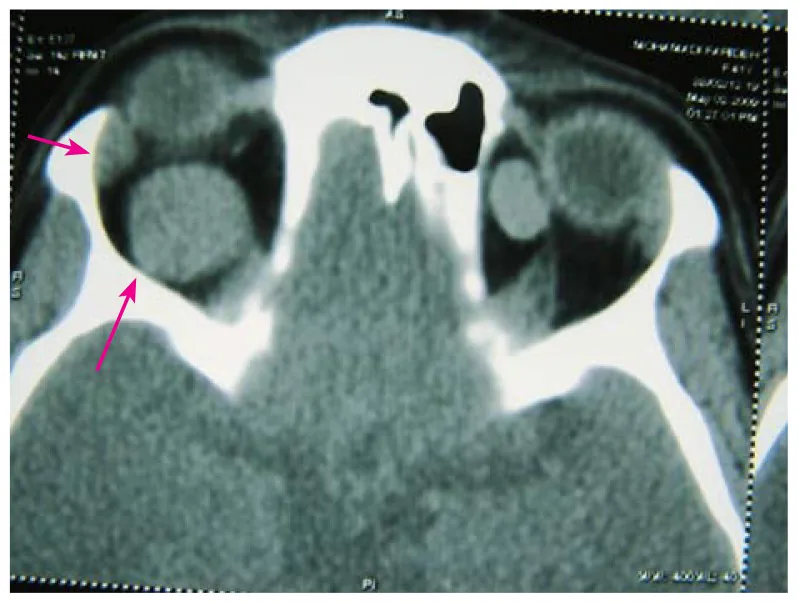
CT: Well-defined, homogeneous solid mass. Commonly located within the muscle cone.
MRI Dynamic: Characteristic gradual enhancement.
Ultrasound: High reflectivity of the capsule with continuous internal spike-like high echoes.
The most common primary orbital tumors are lymphoproliferative disorders, accounting for 50–60% of all orbital tumors. Orbital cavernous hemangioma is the most common benign orbital tumor after lymphoproliferative disorders and is the most frequent benign orbital tumor in adults.
The peak age of onset is 30–50 years, and it is rare in children (in whom capillary hemangioma and lymphangioma are more common). A slight female predominance has been reported, but large-scale epidemiological data are limited.
The diagnosis of orbital cavernous hemangioma is primarily based on imaging studies such as CT and MRI. Imaging is essential for definitive diagnosis, and cerebral angiography is rarely required.
On imaging, benign tumors typically appear well-defined without infiltration into normal tissue. In contrast, malignant tumors and inflammatory diseases often show ill-defined borders and infiltrative patterns, which helps in differentiation.
| Imaging Modality | Findings | Features and Notes |
|---|---|---|
| CT | Well-defined, homogeneous solid mass | Commonly located within the muscle cone. Calcification is rare. Homogeneous enhancement on contrast CT. |
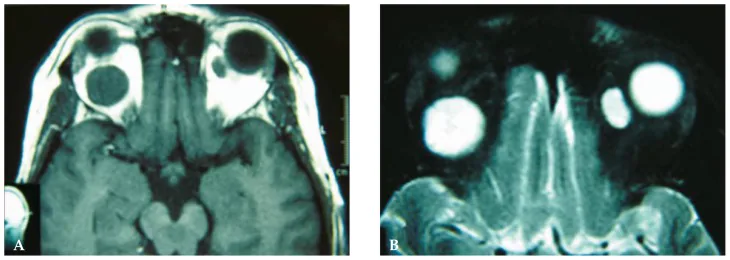
| MRI T1/T2 | T1 low to isointense, T2 hyperintense | Well-defined and homogeneous. The internal signal intensity is uniform. |
| MRI Dynamic (Contrast) | Delayed enhancement (gradual enhancement) | Most characteristic of this disease. Early heterogeneous → homogeneous enhancement over time. |
| Ultrasound (A-mode) | High reflectivity of the capsule + continuous spike-like high internal reflectivity | high internal reflectivity with regular pattern |
| Ultrasound (B-mode) | Well-defined solid mass | High reflectivity of the capsule echo can be observed |
Delayed enhancement (gradual enhancement / progressive filling) on MRI dynamic imaging is the most characteristic imaging finding of orbital cavernous hemangioma [3,4,6]. In the early phase after contrast administration, the internal signal of the tumor is heterogeneous (enhancement starts from one point or a part), and some areas remain unenhanced. Enhancement spreads over time, and eventually the entire tumor becomes uniformly enhanced. This delayed pattern reflects slow blood flow within the tumor, in contrast to schwannoma, which shows early and extensive enhancement, and is important for differentiation from other orbital tumors [3,4].
In A-mode ultrasound, a high reflection indicating the capsule at the anterior wall of the tumor and continuous spike-like high internal reflectivity are observed. This finding is called high internal reflectivity with regular pattern and is characteristic of cavernous hemangioma.
The main differential diagnoses and distinguishing points of orbital cavernous hemangioma are shown below.
| Differential Diagnosis | Distinguishing Points |
|---|---|
| Schwannoma | Difficult to differentiate within the muscle cone. Heterogeneous high signal on T2-weighted MRI (frequent cystic degeneration). Tendency for early enhancement on dynamic MRI. |
| Orbital varices | Mass increases and protrusion worsens with Valsalva maneuver (breath-holding). Changes with positional shift. |
| Lymphangioma | Common in children. Multiloculated with fluid-fluid levels. Recurrent spontaneous hemorrhage. |
| Pleomorphic adenoma of the lacrimal gland | Localized to the lacrimal fossa (superolateral orbit). May cause bony erosion. |
Fine-needle aspiration (FNA) often yields only blood components and has low diagnostic value.
Delayed gradual enhancement on dynamic MRI is the most characteristic finding. Early after contrast injection, the mass appears heterogeneous with some non-enhancing areas, but becomes uniformly enhanced over time. This reflects slow blood flow within the mass. Continuous pattern of high capsular reflection and internal spike-like high reflection on A-mode ultrasound is also characteristic. Combining multiple modalities improves diagnostic accuracy.
Orbital cavernous hemangioma is a benign tumor, and asymptomatic cases are managed with observation as the basic policy. Regular imaging (MRI or CT) is performed to monitor for tumor growth.
Surgery is indicated in the following cases:
In rare pediatric cases where visual development may be affected, or when severe diplopia interferes with daily life, early surgical intervention should be considered.
Lateral Orbitotomy (Standard Procedure)
Indications: Tumors within the muscle cone. Suitable for most cases.
Technique: Temporal skin incision → temporalis muscle dissection → lateral orbital wall osteotomy → access to intraconal tumor.
Key points: En bloc resection of the tumor without rupturing the capsule. Capsule damage increases the risk of intraoperative bleeding and incomplete resection.
Anterior/Transconjunctival Approach
Indications: Small tumors located in the anterior orbit.
Features: Relatively less invasive. Does not require lateral orbital wall osteotomy.
Transconjunctival approach: May be selected as an even less invasive approach for small tumors.
Indications for Observation
Conditions: Asymptomatic with no impact on visual function.
Management: Regular imaging (every 6–12 months) to confirm enlargement.
Indications for intervention: Surgery is considered when visual loss, diplopia, or marked proptosis occurs.
In most cases, tumor removal is possible via lateral orbitotomy [2,5]. The key points of the surgery are as follows.
Complete preservation of the capsule is the most important point. If the capsule is ruptured, blood components from the tumor leak out, impairing the surgical field and making complete removal difficult. Preserving the capsule allows safe en bloc removal of the tumor.
The main complications include the following:
Postoperative transient eye movement disorders often improve over time [2,5]. If there was no visual loss before surgery, visual function is well preserved postoperatively. A large cohort study of 164 cases reported significant improvement in visual acuity, visual field, diplopia, proptosis, and eye movement after surgery [2].
Yes. Since it is a benign tumor, observation is the basic policy if there is no visual impairment, eye movement disorder, or marked proptosis. Surgery is considered when growth tendency or impact on visual function appears. In asymptomatic incidental cases, regular imaging (MRI or CT) is often used to confirm no tumor growth.
If complete resection is achieved without capsule rupture, recurrence is extremely rare. Because the capsule is clear, the complete resection rate is high. However, incomplete resection due to capsule damage poses a risk of recurrence, so preserving the capsule is important during surgery. Rarely, some tumors show malignant features such as recurrence or destruction of surrounding tissues, and appropriate follow-up is recommended.
Orbital cavernous hemangioma is a benign tumor derived from vascular endothelial cells. The entire tumor is surrounded by a fibrous capsule, and the interior consists of a collection of cavernously dilated vascular spaces (cavernous spaces).
The lumina of the vascular spaces are lined with vascular endothelial cells, and the spaces are filled with blood. The septae between the vascular spaces consist of fibrous connective tissue and smooth muscle-like cells. This structure gives the tumor a characteristic soft rubbery texture.
The vascular spaces within the tumor form a closed system with limited communication with the systemic circulation. Therefore, the inflow of contrast agent into the tumor is slow, which causes delayed enhancement (gradual enhancement) observed on dynamic MRI.
Contrast agent gradually permeates from the periphery of the tumor and eventually uniformly enhances the entire tumor. This “gradual enhancement pattern from the periphery to the center” is characteristic of cavernous hemangioma and is useful for differentiation from orbital tumors that enhance uniformly from an early stage (such as some schwannomas or metastatic tumors).
Normal growth is slow and is thought to be due to gradual accumulation of blood in the vascular spaces. Reports of malignant transformation are extremely rare.
Intratumoral hemorrhage (internal bleeding) can cause rapid enlargement. This occurs because the vascular spaces within the tumor rupture and blood accumulates, leading to sudden proptosis, vision loss, and pain. In such cases, emergency surgery may be required.
In the 2018 revision of the ISSVA (International Society for the Study of Vascular Anomalies) classification, it was proposed to reclassify cavernous hemangioma as “venous malformation.” This is based on the understanding that venous malformations are congenital anomalies of vascular structure rather than abnormal proliferation of vascular endothelium. Immunohistochemical studies have also reported findings suggesting a different pathogenesis for encapsulated cavernous lesions in adults compared to infantile hemangiomas [7]. This classification change may affect treatment strategies and understanding of the disease, but whether this reclassification is clinically appropriate for orbital “cavernous hemangioma” remains debated [1].
Following the ISSVA classification revision, there is ongoing debate about reclassifying orbital cavernous hemangioma, previously classified as a “tumor,” as a “low-flow venous malformation.” Whether this reclassification has clinical significance (e.g., indications for sclerotherapy) requires large-scale comparative studies in orbital diseases.
The endoscopic transnasal approach has been reported as a minimally invasive technique for tumors located in the medial (nasal) orbit. It does not require lateral orbital wall osteotomy and is said to have fewer postoperative cosmetic issues, but requires technical proficiency in endoscopic surgery and has limited indications.
Attempts to differentiate benign from malignant orbital tumors using diffusion-weighted MRI (DWI) and apparent diffusion coefficient (ADC) values have been reported. Cavernous hemangiomas are said to have high ADC values, which may be useful for distinguishing them from malignant tumors, but large-scale validation in the orbital region is still insufficient.
Spontaneous regression of orbital cavernous hemangioma is extremely rare, but sporadic case reports exist. It has been suggested that it may be associated with pregnancy or fluctuations in female hormones, but the mechanism remains unclear, and it has not been established as a basis for continued observation in asymptomatic cases.
Calandriello L, Grimaldi G, Petrone G, et al. Cavernous venous malformation (cavernous hemangioma) of the orbit: Current concepts and a review of the literature. Surv Ophthalmol. 2017;62(4):393-403. doi:10.1016/j.survophthal.2017.01.004. PMID: 28131871
Strianese D, Bonavolontà G, Iuliano A, et al. Risks and Benefits of Surgical Excision of Orbital Cavernous Venous Malformations (So-Called Cavernous Hemangioma): Factors Influencing the Outcome. Ophthalmic Plast Reconstr Surg. 2021;37(3):248-254. doi:10.1097/IOP.0000000000001767. PMID: 32826827
Tanaka A, Mihara F, Yoshiura T, et al. Differentiation of cavernous hemangioma from schwannoma of the orbit: a dynamic MRI study. AJR Am J Roentgenol. 2004;183(6):1799-1804. doi:10.2214/ajr.183.6.01831799. PMID: 15547232
Xian J, Zhang Z, Wang Z, et al. Evaluation of MR imaging findings differentiating cavernous haemangiomas from schwannomas in the orbit. Eur Radiol. 2010;20(9):2221-2228. doi:10.1007/s00330-010-1774-y. PMCID: PMC2914262
Kim MH, Kim JH, Kim SE, Yang SW. Surgical Outcomes of Intraconal Cavernous Venous Malformation According to Their Location in Four Right-Angled Sectors. J Craniofac Surg. 2019;30(6):1700-1705. doi:10.1097/SCS.0000000000005501. PMID: 30950949
Zhang L, Li X, Tang F, Gan L, Wei X. Diagnostic Imaging Methods and Comparative Analysis of Orbital Cavernous Hemangioma. Front Oncol. 2020;10:577452. doi:10.3389/fonc.2020.577452. PMCID: PMC7539693
Osaki TH, Jakobiec FA, Mendoza PR, Lee Y, Fay AM. Immunohistochemical investigations of orbital infantile hemangiomas and adult encapsulated cavernous venous lesions (malformation versus hemangioma). Ophthalmic Plast Reconstr Surg. 2013;29(3):183-195. doi:10.1097/IOP.0b013e31828b0f1f. PMID: 23584448