Thyroid Eye Disease (TED) is an autoimmune orbital disease caused by thyroid-related autoantibodies acting on orbital tissues. It is also called thyroid-associated ophthalmopathy (TAO) or Graves ophthalmopathy (GO).
Thyroid eye disease can occur in association with hyperthyroidism (Graves’ disease) or as euthyroid ophthalmopathy with completely normal thyroid function. Thyroid eye disease essentially progresses independently of thyroid hormones and is one of the autoimmune diseases involving thyroid-related autoantibodies.
The prevalence of thyroid eye disease is reported as 16 per 100,000 women and 2.9 per 100,000 men per year6). Among patients with Graves’ disease, 25–50% develop eye involvement5). The age of onset shows a bimodal distribution with peaks at 40–50 years and 60–70 years6). Smoking is a major risk factor for both onset and severity12), and smoking cessation guidance is fundamental to treatment.
Hashimoto’s disease (chronic thyroiditis) can also cause eye symptoms, but most cases present as euthyroid ophthalmopathy. The mechanism by which thyroid-related autoantibodies (anti-TPO antibodies, anti-TG antibodies) affect orbital tissues shares common features with Graves’ ophthalmopathy.
QCan eye symptoms occur even if thyroid levels are normal?
A
Yes. As euthyroid ophthalmopathy, eye disease can develop even when thyroid function is normal. Because thyroid-related autoantibodies act directly on orbital tissues, eye symptoms appear independently of thyroid hormone levels. Blood tests for autoantibodies and orbital imaging are important for diagnosing thyroid eye disease.
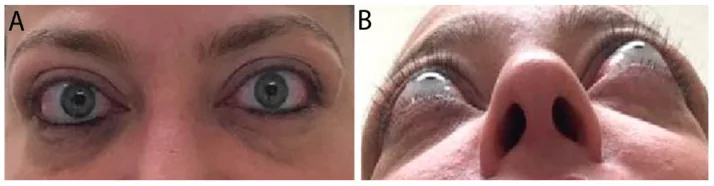
Rashad R, Pinto R, Li E, Sohrab M, Distefano AG. Thyroid Eye Disease. Life (Basel). 2022;12(12):2084. Figure 2. PMCID: PMC9787503. License: CC BY 4.0.
Color photograph of the external eye of a patient with chronic moderate-to-severe thyroid eye disease. (A) Upper and lower eyelid retraction, lateral flare of the upper eyelid, and moderate periorbital fat prolapse are seen; (B) in the chin-up view (worm’s eye view), bilateral proptosis is clearly observed. This corresponds to eyelid retraction and proptosis discussed in the section “2. Main symptoms and clinical findings.”
Clinical symptoms are broadly classified into four categories: eyelid symptoms, proptosis, diplopia, and visual impairment. Proptosis is more common in younger patients, while ocular motility disorders and diplopia are more common in older patients.
Eyelid symptoms
Upper eyelid retraction: The most frequent sign. Caused by sympathetic overactivity to Müller’s muscle or fibrosis of the levator muscle.
Lid lag: The upper eyelid lags behind during downward gaze.
Eyelid swelling: Swelling due to edema and fat proliferation of the eyelids. Inflammatory cases may respond to local steroid injections.
Proptosis
Measured with a Hertel exophthalmometer. Normal value is less than 18 mm, and in patients with thyroid eye disease it often exceeds 21 mm.
The eyeball is pushed forward due to proliferation of orbital fat tissue and enlargement of the extraocular muscles.
Asymmetry (2 mm or more) is a diagnostic clue.
Diplopia and Ocular Movement Disorders
Inferior rectus and medial rectus are commonly affected, often leading to vertical and esotropia.
Contractile changes of the extraocular muscles (sparing the tendon insertions) are characteristic and can be confirmed on CT.
Corneal disorders: Decreased vision due to lagophthalmos and exposure keratitis.
Dysthyroid optic neuropathy (DON): The optic nerve is compressed by increased intraorbital pressure from enlarged extraocular muscles. It occurs in about 5% of patients5) and requires urgent intervention.
Rapid vision loss, color vision abnormalities, and visual field defects are warning signs.
Progression from Initial Symptoms to Severe Disease
Initially, dry eye-like complaints such as dryness, irritation, tearing, and photophobia may precede. Later, eyelid swelling, proptosis, and diplopia become apparent. In severe cases, corneal exposure or dysthyroid optic neuropathy occurs, requiring urgent treatment.
As shown by the Rundle curve14), thyroid eye disease follows a biphasic course: an active (inflammatory) phase and an inactive (fibrotic/stable) phase. The active phase typically lasts 1–3 years, after which it stabilizes spontaneously, but early control of inflammation with appropriate treatment is important.
QI feel my eyes are bulging out. Is it related to the thyroid?
A
Proptosis is one of the main symptoms of thyroid eye disease. The eyeball is pushed forward due to enlargement of orbital fat and extraocular muscles. If you notice proptosis, especially with Graves’ disease, prompt ophthalmologic evaluation is necessary. Measurement with a Hertel exophthalmometer and CT or MRI to assess the orbit are performed.
TSH receptors are expressed on fibroblasts in the retrobulbar tissues of the orbit. These TSH receptors act as antigens, promoting lymphocyte infiltration into orbital tissues, activating macrophages, and triggering an inflammatory response through a local cytokine network.
Infiltration of immune cells (mainly CD4+/CD8+ T cells) into orbital tissues triggers the following cascade 8)16):
TSH receptor antibodies → activation of orbital fibroblasts
Release of inflammatory cytokines (TNF-α, IL-6, IL-1β)
Excessive synthesis of glycosaminoglycans (hyaluronic acid) → tissue edema
Differentiation of fibroblasts into adipocytes and myofibroblasts → orbital fat expansion and extraocular muscle fibrosis
Increased intraorbital pressure → proptosis and optic nerve compression
It has been shown that IGF-1 receptor (IGF-1R) and TSH receptor form a receptor complex that amplifies signal transduction 4), which is the therapeutic target of teprotumumab described later.
Smoking: The strongest modifiable factor. It significantly increases the risk of developing thyroid eye disease, progression, and treatment resistance 12). Smoking cessation directly improves treatment outcomes.
Radioactive iodine (RAI) therapy: Especially when performed without steroid coverage, it increases the risk of worsening eye disease 1).
Unstable thyroid function (rapid fluctuations between hypothyroidism and hyperthyroidism)
Older age and male sex (tendency for more severe disease)
High thyroid-stimulating hormone receptor antibody (TRAb) levels
QHow does smoking affect thyroid eye disease?
A
Smoking is the strongest risk factor for thyroid eye disease. It increases the risk of developing the disease and its severity, and reduces the effectiveness of treatments such as steroids. The risk of worsening eye disease after radioactive iodine therapy is also higher in smokers. Smoking cessation has been shown to improve treatment outcomes, and counseling patients to quit smoking is an important part of treatment.
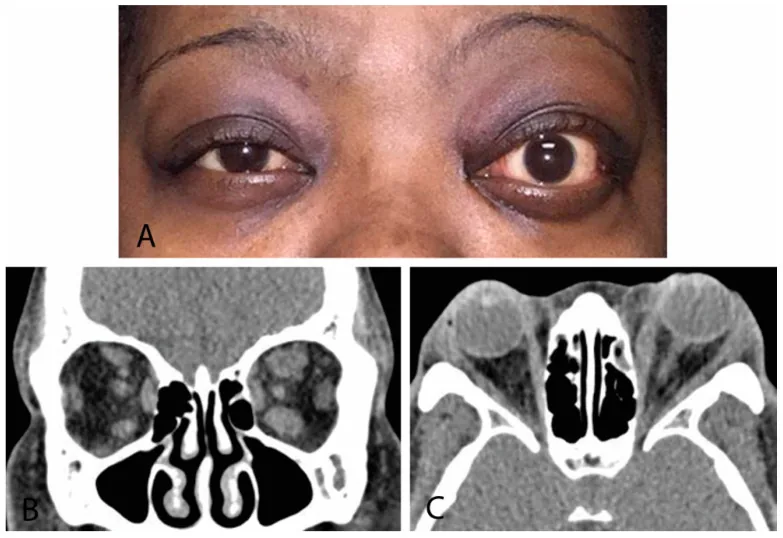
Rashad R, Pinto R, Li E, Sohrab M, Distefano AG. Thyroid Eye Disease. Life (Basel). 2022;12(12):2084. Figure 4. PMCID: PMC9787503. License: CC BY 4.0.
(A) External eye photograph showing asymmetric proptosis with left eye predominance, (B) Coronal orbital CT showing left-predominant thickening of the rectus muscles (muscle belly hypertrophy with tendon sparing pattern), (C) Sagittal CT image of the same. The finding of sparing of the tendon insertion of the rectus muscles is important for differentiation from IgG4-related disease and orbital myositis. This corresponds to the CT evaluation of extraocular muscle hypertrophy discussed in the section “4. Diagnosis and Testing Methods.”
Clinical diagnosis is fundamental. It is diagnosed by the combination of eyelid retraction, proptosis, diplopia, and a history of thyroid disease. An important note is that for a definitive diagnosis of thyroid eye disease, hypertrophy and inflammation of the extraocular muscles must correlate with eye position and restriction of eye movement.
CT: Confirms hypertrophy of extraocular muscles (characterized by sparing of tendon insertions, important for differential diagnosis). Also useful for evaluating the orbital floor and bony structures.
MRI: T1-weighted images assess the morphology of extraocular muscles, and STIR (short-TI inversion recovery) sequences evaluate the presence of inflammation. STIR can depict inflammatory areas as high signal regions without contrast, useful for assessing disease activity in thyroid eye disease.
B-scan ultrasound: Evaluates extraocular muscle enlargement and acoustic reflection patterns
The CAS9) proposed by Mourits et al. is widely used as an objective indicator of activity in thyroid eye disease.
CAS Assessment Items
Points
Spontaneous orbital pain or retrobulbar pressure
1 point
Pain on eye movement
1 point
Eyelid redness
1 point
Conjunctival injection (diffuse)
1 point
Eyelid swelling
1 point
Chemosis
1 point
Inflammation of caruncle and plica semilunaris
1 point
In the original report by Mourits et al., patients with an activity score of 3 or more showed a good response to anti-inflammatory treatment, which was considered useful for treatment selection9).
QHow is the activity of thyroid eye disease determined?
A
It is assessed using the Clinical Activity Score (CAS). Seven items are scored: pain, pain with eye movement, eyelid redness, conjunctival injection, eyelid swelling, chemosis, and caruncle inflammation. A score of 3 or more out of 7 indicates active disease. Determining activity is important for deciding on immunosuppressive therapy such as steroid pulse therapy. MRI STIR sequence can also be useful to confirm orbital inflammatory activity.
If hyperthyroidism is present, normalization of thyroid hormone levels is an essential prerequisite. This is achieved with antithyroid drugs such as thiamazole (MMI). However, thyroid treatment does not directly improve eye disease; eye treatment is carried out concurrently.
Radioactive iodine (RAI) therapy carries a risk of worsening eye disease, so it should be used cautiously in patients with moderate to severe active eye disease, and steroid coverage should be considered if administered 1).
Selenium supplementation: Selenium methionine 100 μg twice daily for 6 months has been shown to be effective in preventing progression of mild thyroid eye disease in an RCT (Marcocci 2011 NEJM)13). The EUGOGO guidelines 20211) recommend its use in mild cases.
Symptomatic treatment: Corneal protection with artificial tears and lubricating eye ointment, photophobia management with tinted lenses, and correction of diplopia with prism lenses.
In the RCT by Kahaly et al., intravenous administration of methylprednisolone 0.5 g once weekly for 6 weeks, followed by 0.25 g once weekly for 6 weeks (cumulative 4.5 g), was more effective and better tolerated than oral prednisolone tapering therapy11).
During the inflammatory phase, pulse therapy with methylprednisolone 1 g for 3 days per course is also used.
Second-line: Orbital radiotherapy
A total dose of 20 Gy is delivered in 2 Gy fractions, 5 times per week for 2 weeks. Synergistic effects can be expected when combined with steroids7). It is particularly effective for diplopia and ocular motility disorders. Radiotherapy should be considered cautiously in young patients (under 35 years) and those with diabetes or hypertension.
Other immunotherapies
Rituximab (anti-CD20 antibody): Has been reported to reduce disease activity in refractory active moderate-to-severe cases10)
Tocilizumab (IL-6 inhibitor): Considered for refractory cases 17)
Surgery is generally performed during the inactive phase when inflammation has sufficiently subsided. The order of procedures is important and should follow the sequence below 15):
Eyelid surgery (correction of eyelid retraction) — Performed last to balance the upper and lower eyelids.
Orbital decompression18): Removal of part of the medial, inferior, and lateral orbital walls to expand the orbital volume, relieving proptosis and optic nerve compression. Minimally invasive endoscopic approaches are widely used.
Visual prognosis is good if intervention is performed at the appropriate time. However, in thyroid eye disease presenting with compressive optic neuropathy, visual prognosis may be poor, making early detection and treatment important 15).
QWhen is the best time to perform surgery for thyroid eye disease?
A
Surgery is generally performed during the inactive phase when inflammation has subsided. The standard sequence is: ① orbital decompression → ② strabismus surgery → ③ eyelid surgery. Following this order prevents earlier surgeries from affecting later results (e.g., strabismus changes after orbital decompression). However, compressive optic neuropathy is an indication for emergency surgery, and orbital decompression is performed promptly regardless of the active or inactive phase.
Fibroblasts in the retrobulbar orbital tissues express TSH receptors, which become targets of the autoimmune response. TSH receptor antibodies (TRAb) produced in patients with Graves’ disease bind not only to thyroid TSH receptors but also to TSH receptors on orbital fibroblasts, initiating an inflammatory cascade locally in the orbit8).
The pathogenesis progresses through the following steps:
Antigen presentation and autoantibody production: Activated T cells recognize the TSH receptor. B cells produce TRAb and TSAb.
Activation of orbital fibroblasts: TRAb binds to TSH receptors on orbital fibroblasts, leading to activation of intracellular signaling pathways.
Amplification of the IGF-1R pathway4): TSH receptors and IGF-1 receptors (IGF-1R) form receptor complexes, amplifying signals. Teprotumumab improves ophthalmopathy by blocking IGF-1R.
Release of inflammatory cytokines: Inflammatory cytokines such as TNF-α, IL-6, and IL-1β are released locally in the orbit, causing increased vascular permeability, edema formation, and further infiltration of immune cells 16).
Excessive synthesis of glycosaminoglycans (hyaluronic acid): Stimulated orbital fibroblasts overproduce glycosaminoglycans such as hyaluronic acid, leading to fluid retention and swelling of orbital tissues.
Differentiation into adipocytes: Fibroblasts differentiate into adipocytes (adipogenesis), increasing orbital fat volume.
Changes in extraocular muscles: Lymphocytes, plasma cells, and macrophages infiltrate the extraocular muscles, causing edema and deposition of glycosaminoglycans between muscle fibers. In the late inflammatory to inactive phase, fibrosis progresses, reducing muscle mobility.
Mechanisms of increased orbital pressure and proptosis
Proliferation of orbital fat and hypertrophy of extraocular muscles increase orbital content volume, raising pressure within the fixed bony orbit (orbital volume approximately 30 mL). This increased intraorbital pressure pushes the eyeball forward (proptosis) and may progress to venous stasis and optic nerve compression (orbital apex syndrome).
Optic nerve compression at the orbital apex is the main mechanism of compressive optic neuropathy, which can be identified on CT as apical crowding due to accumulation of extraocular muscles at the orbital apex.
The Rundle curve 14) is a model illustrating the natural course of thyroid eye disease, showing a biphasic pattern with an active (inflammatory) phase and an inactive (stable/fibrotic) phase. The active phase generally lasts 1 to 3 years, after which disease activity decreases and stabilizes. However, even after transitioning to the inactive phase, morphological changes such as proptosis, diplopia, and eyelid retraction often persist, and surgical correction is considered during this period.
Teprotumumab (TEPEZZA®) is a human monoclonal antibody targeting IGF-1R, approved by the US FDA in 2020 for moderate-to-severe active thyroid eye disease2)3).
The dosing protocol is an initial dose of 3 mg/kg, followed by 10 mg/kg for the second dose, and then 20 mg/kg (maximum) for the third and subsequent doses, administered as intravenous infusions every 3 weeks for a total of 8 doses.
A meta-analysis of 5 RCTs involving a total of 411 patients (Cong et al. 2024) 4) showed that compared to placebo, the teprotumumab group had:
Significant improvement in proptosis
Improvement in diplopia (significant increase in diplopia response rate)
Significant reduction in CAS score
No significant difference in the incidence of serious adverse events compared to placebo
The main adverse events requiring attention include hearing impairment (high-frequency hearing loss), hyperglycemia, and muscle cramps 4).
The joint position statement of the American Thyroid Association (ATA) and the European Thyroid Association (ETA) recommends it for active moderate-to-severe TED.
Rituximab (anti-CD20 antibody): Targets B cells; some RCTs have reported reduced activity in thyroid eye disease10)
Tocilizumab (IL-6 inhibitor): Case reports and small studies in refractory cases have shown improvement in eye disease activity; future clinical trials are expected 17)
Bartalena L, Kahaly GJ, Baldeschi L, et al. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur J Endocrinol. 2021;185(4):G43-G67. doi:10.1530/EJE-21-0479. PMID:34297684.
Douglas RS, Kahaly GJ, Patel A, et al. Teprotumumab for the treatment of active thyroid eye disease. N Engl J Med. 2020;382(4):341-352. doi:10.1056/nejmoa1910434.
Smith TJ, Kahaly GJ, Ezra DG, et al. Teprotumumab for thyroid-associated ophthalmopathy. N Engl J Med. 2017;376(18):1748-1761. doi:10.1056/nejmoa1614949.
Cong X, Pei L, Hu H. Teprotumumab for treating active thyroid eye disease: A meta-analysis. Medicine (Baltimore). 2025 Jun 27;104(26):e42966. doi:10.1097/MD.0000000000042966. PMID:40587732; PMCID:PMC12212777.
Rebecca S. Bahn. Graves’ Ophthalmopathy. N Engl J Med. 2010;362(8):726-738. doi:10.1056/nejmra0905750.
Wiersinga WM, Bartalena L. Epidemiology and prevention of Graves’ ophthalmopathy. Thyroid. 2002;12(10):855-860. doi:10.1089/105072502761016476.
Stan MN, Salvi M. Management of thyroid eye disease. J Clin Endocrinol Metab. 2017;102(11):4088-4100.
Bahn RS. Clinical review 157: Pathophysiology of Graves’ ophthalmopathy: the cycle of disease. J Clin Endocrinol Metab. 2003;88(5):1939-1946. doi:10.1210/jc.2002-030010.
Mourits MP, Koornneef L, Wiersinga WM, Prummel MF, Berghout A, van der Gaag R. Clinical criteria for the assessment of disease activity in Graves’ ophthalmopathy: a novel approach. The British journal of ophthalmology. 1989;73(8):639-44. doi:10.1136/bjo.73.8.639. PMID:2765444; PMCID:PMC1041835.
Salvi M, Vannucchi G, Curro N, Campi I, Covelli D, Dazzi D, et al. Efficacy of B-cell targeted therapy with rituximab in patients with active moderate to severe Graves’ orbitopathy: a randomized controlled study. J Clin Endocrinol Metab. 2015;100(2):422-431. PMCID: PMC4318899. doi:10.1210/jc.2014-3014.
Kahaly GJ, Pitz S, Hommel G, Dittmar M. Randomized, single blind trial of intravenous versus oral steroid monotherapy in Graves’ orbitopathy. The Journal of clinical endocrinology and metabolism. 2005;90(9):5234-40. doi:10.1210/jc.2005-0148. PMID:15998777.
Prummel MF, Wiersinga WM. Smoking and risk of Graves’ disease. JAMA. 1993;269(4):479-482. doi:10.1001/jama.1993.03500040045034.
Marcocci C, Kahaly GJ, Krassas GE, Bartalena L, Prummel M, Stahl M, et al. Selenium and the course of mild Graves’ orbitopathy. The New England journal of medicine. 2011;364(20):1920-31. doi:10.1056/NEJMoa1012985. PMID:21591944.
RUNDLE FF, WILSON CW.. Development and course of exophthalmos and ophthalmoplegia in Graves’ disease with special reference to the effect of thyroidectomy. Clin Sci. 1945;5(3-4):177-194. PMID:21011937.
Wakelkamp IM, Baldeschi L, Saeed P, et al. Surgical or medical decompression as a first-line treatment of optic neuropathy in Graves’ ophthalmopathy? A randomized controlled trial. Clin Endocrinol. 2005;63(3):323-328. doi:10.1111/j.1365-2265.2005.02345.x.
James A. Garrity, Rebecca S. Bahn. Pathogenesis of Graves Ophthalmopathy: Implications for Prediction, Prevention, and Treatment. American Journal of Ophthalmology. 2006;142(1):147-153.e2. doi:10.1016/j.ajo.2006.02.047.
Kabra A, Higuchi K, Sheth A, et al. Tocilizumab in refractory thyroid eye disease: a case series. Ophthalmology. 2018;125(9):1326-1328.