Congenital red-green color vision deficiency is found in about 5% of Japanese males and about 0.2% of Japanese females. It is an X-linked genetic disease caused by deletion or expression abnormality of the L and M genes on the X chromosome, and is the most common type of congenital color vision deficiency. There are racial differences: about 6–8% in Caucasian males, 4–5% in Asian males, and 2–4% in Black males.
The purposes of color vision testing can be summarized into the following four points.
① Screening: Detection of color vision abnormalities in school checkups and occupational aptitude tests.
② Type and severity assessment: Classification into type 1, type 2, or type 3 and evaluation of severity.
③ Detection of acquired color vision deficiency: Auxiliary diagnosis and disease monitoring for retinal and optic nerve diseases.
④ Career and employment counseling: Evaluation of occupational aptitude and collection of information for lifestyle guidance.
Testing is based on a three-step approach: screening → severity assessment → definitive diagnosis, depending on the purpose. The Ishihara color vision test is most widely used as the first step of screening, followed by the Panel D-15 test for severity assessment, and finally the anomaloscope for definitive diagnosis.
Color vision testing in schools was removed from the mandatory items of regular health checkups in 2003 with the revision of the School Health and Safety Act Enforcement Regulations. Subsequently, cases of students facing difficulties in career choices without being aware of their color vision deficiency increased, and in 2014, a notice from the Ministry of Education, Culture, Sports, Science and Technology recommended the implementation of color vision testing in schools (for those who wish) 4).
QWho should undergo color vision testing?
A
Testing is recommended mainly in the following situations: ① School health checkups around the fourth grade of elementary school or voluntary testing. ② Before career or employment choices (if interested in occupations with color vision restrictions, such as aviation, railways, police, etc.). ③ When monitoring color vision changes is necessary for follow-up of eye diseases (e.g., retinitis pigmentosa, optic neuritis, macular diseases). ④ To confirm carrier status when there is a family history of color vision deficiency. Early identification of the presence, type, and severity of color vision deficiency enables appropriate career choices and lifestyle guidance.
2. Indications and clinical significance of each color vision test
Step 1 (Screening): Pseudoisochromatic plates (Ishihara plates, Standard Color Vision Test Part 1) → Detects presence of color vision deficiency.
Step 2 (Severity assessment): Panel D-15 test → Evaluates type and severity.
Step 3 (Definitive diagnosis): Anomaloscope → Confirms type and precise severity.
For evaluation of acquired color vision deficiency, the Standard Color Vision Test Part 2 or the FM 100 Hue Test is used. Acquired color vision deficiency is broadly classified into acquired blue-yellow deficiency and acquired red-green deficiency depending on the degree of impairment of each cone system, but neither appears alone; both are always present together, albeit to varying degrees.
QWhat types of color vision tests are available?
A
They are broadly classified into four types. ① Pseudoisochromatic plates (color confusion plates): Ishihara plates, Standard Color Vision Test Parts 1 and 2, etc. Used for screening and evaluation of acquired deficiencies. ② Hue arrangement tests: Panel D-15 test, FM 100 Hue test. Used for severity assessment and analysis of confusion axes. ③ Anomaloscope: A diagnostic device based on matching a mixture of red and green to a yellow monochromatic light. ④ Computerized tests (e.g., Cambridge Colour Test): Allow quantitative evaluation of congenital and acquired deficiencies. Each test has its advantages and disadvantages, so it is important to combine them according to the purpose.
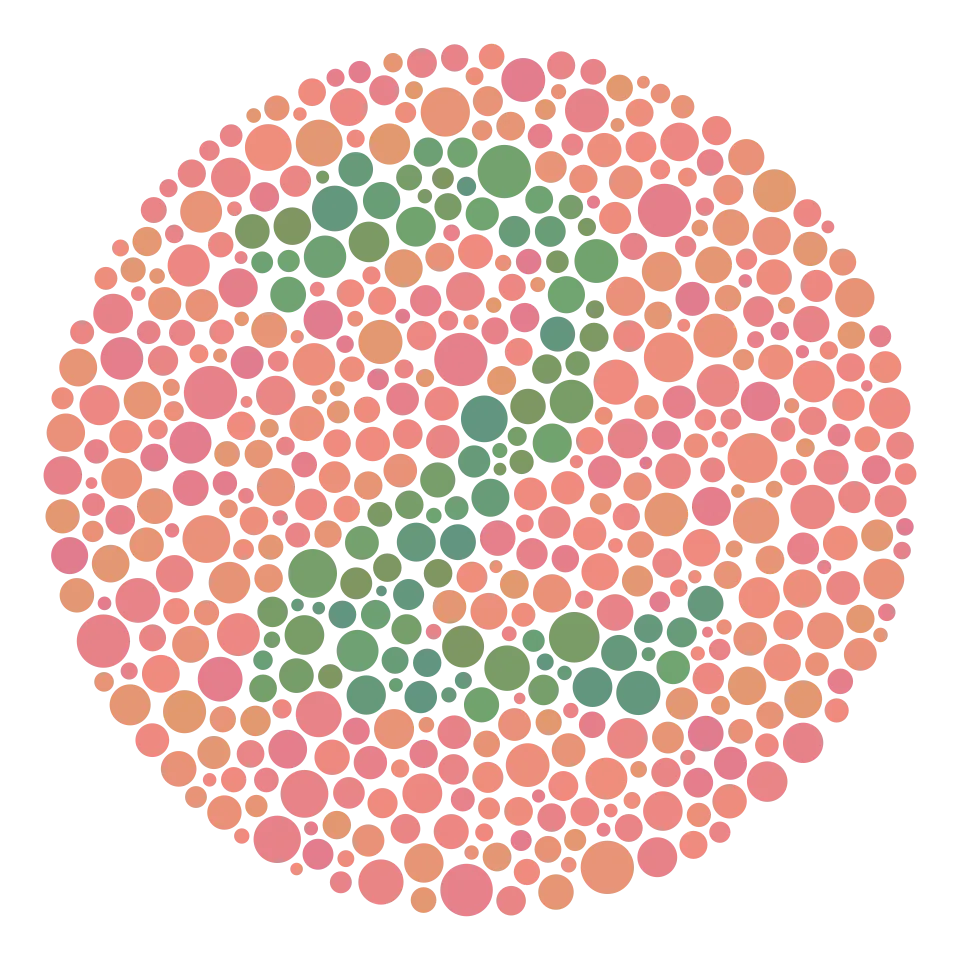
One of the Ishihara color vision test plates, a pseudoisochromatic plate in which the number “2” is drawn with confusion color dot patterns that are difficult for people with red-green color vision deficiency to read. This corresponds to the pseudoisochromatic principle of the Ishihara color vision test discussed in the section “3. Principles and Procedures of Each Test.”
Ishihara Color Vision Test (Pseudoisochromatic Plates)
Principle: Uses figures (numbers, patterns) that appear differently to people with red-green color vision deficiency and those with normal color vision. It employs the principle of confusion colors, including plates that are unreadable to those with color vision deficiency and plates that are unreadable to those with normal color vision.
Testing conditions: Performed under natural daylight or standard illumination. Follow the instructions for the specific test plates regarding testing distance and presentation time.
Interpretation: The international 38-plate edition includes three types: transformation plates, vanishing plates, and classification plates. The presence of red-green color vision deficiency is determined by the pattern of misreadings. It is suitable for screening red-green color vision deficiency but insufficient for detailed determination of type and severity, and cannot detect tritan (blue-yellow) deficiency2).
Recommendation: It is recommended to combine two or more types of pseudoisochromatic plates rather than using only one type.
Panel D-15 Test (Hue Arrangement Test)
Principle: The patient is asked to arrange 15 color chips based on the Munsell color system in order of closest similarity to a fixed reference chip. Individuals with normal color vision can arrange them in nearly correct order 5).
Procedure: Start with 1 fixed chip and 15 movable chips arranged in random order. The patient sequentially selects the chip that appears closest to the reference chip. The test takes about 3–5 minutes.
Interpretation patterns:
Normal: Nearly correct order (no confusion)
Protan: Crossing pattern along the protan confusion axis
Deutan: Crossing pattern along the deutan confusion axis
Tritan: Crossing pattern along the scotopic axis
Features: Suitable for evaluating mild to moderate color vision deficiencies. Very mild anomalous trichromats may pass the test. It can also be used to assess acquired color vision deficiencies 5).
FM 100 Hue Test (Detailed Examination)
Principle: A precise hue arrangement test in which 85 color chips are arranged in hue order. As an expanded version of the Panel D-15, it evaluates finer hue discrimination ability 5).
Procedure: The 85 chips are divided into 4 boxes (22–23 chips each) and tested independently. Error scores are calculated for each box. The test takes 15–30 minutes (susceptible to fatigue and concentration).
Interpretation: Error scores are plotted on a deviation plot to evaluate the pattern of confusion axes. Quantitative assessment is performed using confusion angle, C-index, and S-index 3).
Uses: Useful for detecting subtle acquired color vision deficiencies, detailed evaluation of hue discrimination, and longitudinal monitoring. Primarily used in specialized facilities 5).
Standard Color Vision Test Chart Part 2 (For Acquired Deficiencies)
Principle: A pseudoisochromatic plate specialized for detecting acquired color vision deficiencies (including blue-yellow defects). It can detect acquired abnormal patterns that the Ishihara plates cannot.
Procedure: Test each eye separately. Since acquired color vision deficiencies may show differences between eyes, monocular testing is important.
Indications: Used for screening acquired color vision deficiencies secondary to retinal diseases, optic nerve diseases, glaucoma, etc. Also used in follow-up of diabetic retinopathy, age-related macular degeneration, optic neuritis, etc.
Note: Not used for screening congenital color vision deficiencies.
QHow is the Panel D-15 test interpreted?
A
Record the order of the 15 color caps and plot the cap numbers on a polar coordinate diagram (desaturation diagram). In normal color vision, lines connecting adjacent caps show a regular pattern close to a circle. In color vision deficiency, large crossing lines appear across the confusion axis. In protan defects, crossing lines along the protan confusion axis; in deutan defects, along the deutan confusion axis; in tritan defects, along the scotopic axis. Very mild anomalous trichromats may pass, requiring additional evaluation with the FM 100 Hue test or anomaloscope.
Gabriela P. Farnsworth–Munsell Hue Color Vision Test, Material and Finishing Laboratory. Wikimedia Commons. 2019. Figure 2. Source ID: commons.wikimedia.org/wiki/File:Farnsworth%E2%80%93Munsell_Hue_Color_Vision_Test,_Material_and_Finishing_Laboratory.jpg. License: CC BY 4.0.
Photograph of the actual Farnsworth-Munsell Hue test with four boxes and color caps taken in a laboratory, showing each box containing 22–23 color caps. This corresponds to the color cap set evaluated in the hue arrangement tests discussed in section “4. Interpretation of Test Results.”
Types of Congenital Color Vision Deficiency and Test Findings
The classification of congenital red-green color vision deficiency and corresponding findings in each test are shown below. The most common type is deuteranomaly, followed by deuteranopia, then protanomaly and protanopia.
Ishihara plates have high sensitivity for detecting red-green color vision deficiency, but low accuracy for determining type and severity. It is recommended to combine two or more types of pseudoisochromatic plates. Tritan color vision deficiency (congenital blue-yellow deficiency) cannot be detected by Ishihara plates and is evaluated using the Standard Pseudoisochromatic Plates Part 2 or the Panel D-15 test.
Acquired color vision deficiency can be caused by abnormalities anywhere in the visual pathway, including the cornea, lens, vitreous body, retina, optic nerve, optic tract, primary visual cortex, optic radiation, and visual centers of the cerebral cortex. The most common causes are retinal and optic nerve diseases.
Acquired color vision deficiency is broadly divided into acquired blue-yellow deficiency and acquired red-green deficiency, but neither appears alone; both are always present to varying degrees.
In retinitis pigmentosa, color vision impairment worsens with the decline of cone function, and acquired blue-yellow color vision deficiency is detected at a high frequency 1). Color naming tasks are useful for understanding real-life color misidentification and providing advice to patients.
QWhat test is suitable for detecting acquired color vision deficiency?
A
For the evaluation of acquired color vision deficiency, the Standard Pseudoisochromatic Plates Part 2 or the Farnsworth-Munsell 100 Hue Test is suitable. The Ishihara plates are designed for congenital red-green color vision deficiency and are not suitable for detecting acquired color vision deficiency (especially blue-yellow). The FM 100 Hue Test has high sensitivity for detecting mild acquired color vision deficiency and is also suitable for longitudinal monitoring. In the follow-up of retinal and optic nerve diseases, it is important to test each eye separately and track changes in asymmetry.
Due to the 2003 amendment of the School Health and Safety Act Enforcement Regulations, color vision testing was removed from the mandatory items of school periodic health examinations. In response to an increase in cases where individuals grew up without awareness of their color vision deficiency and faced difficulties at the stage of career choice, the Ministry of Education, Culture, Sports, Science and Technology issued a notice in 2014 recommending color vision testing in schools (on a voluntary basis) 4).
It is recommended that children undergo detailed type determination by an ophthalmologist around the fourth grade of elementary school (a period of physical and psychological stability). Accurately understanding one’s own color vision characteristics before career choice is important to support appropriate career selection.
For patients with congenital color vision deficiency (especially young children), the explanation is mainly given to guardians. Since color vision deficiency is innate, it must be kept in mind that even if the patient misidentifies colors, it is never a “mistake” for them. The most important thing is to fully consider the color vision deficiency in future educational and career choices, and to prevent difficulties arising from the condition.
Certain occupations and licenses (e.g., aircraft pilots, train drivers, ship operators, police officers, Self-Defense Forces personnel) may have restrictions related to color vision. It is important to specifically confirm the job content and restriction status and provide individual advice.
The perspective of color universal design, which utilizes information other than color (such as shape, position, brightness, labels, and texture), is also useful in patient guidance.
Spread of digital/computerized color vision tests:
Standardization of color vision tests on tablets and monitors is progressing. Computerized tests such as the Cambridge Colour Test (CCT) allow quantitative assessment of congenital and acquired color vision deficiencies and reduce examiner-dependent variability 5). However, proper display calibration is a prerequisite for test accuracy.
Spread of color universal design:
Applications in public signage, educational materials, web design, and medical documents are advancing. Information transmission design that does not rely solely on color improves information access for people with color vision diversity.
Collaboration with genetic diagnosis:
Research on molecular biological definitive diagnosis by L/M gene analysis is progressing. The correspondence between phenotype evaluation by anomaloscope and genotype is being refined, and future clinical application is expected.