
Traumatic Mydriasis (Sphincter Pupillae Rupture)
Key Points at a Glance
Section titled “Key Points at a Glance”1. What is Traumatic Mydriasis (Pupillary Sphincter Tear)?
Section titled “1. What is Traumatic Mydriasis (Pupillary Sphincter Tear)?”Traumatic mydriasis is a condition in which the pupillary sphincter is torn by blunt force, resulting in a dilated pupil.
The pupillary sphincter is a smooth muscle that runs circularly along the pupillary margin of the iris and is responsible for constricting the pupil under parasympathetic control. In blunt trauma, this sphincter is physically torn, causing pupillary dilation. Depending on the severity, the condition ranges from transient dysfunction to permanent rupture.
Blunt trauma to the iris and pupil can cause a spectrum of conditions. In the mildest form, only traumatic iritis (microscopic tissue damage with blood-aqueous barrier disruption and inflammatory cell infiltration into the anterior chamber) occurs. When the pupillary sphincter is damaged, traumatic mydriasis (varying degrees of pupillary dilation) develops. More severe cases lead to iridodialysis (tear at the iris root causing pupil distortion), and the most severe cases result in angle recession or cyclodialysis. Traumatic mydriasis lies in the middle of this spectrum and often coexists with other iris injuries.
It occurs as a complication of blunt ocular trauma (ball injuries, fists, traffic accidents, falls, etc.), but detailed epidemiological data on its incidence are not available. Sports injuries (baseball, tennis, soccer, etc.), occupational accidents, and falls in daily life are typical mechanisms of injury.
In many cases, it resolves spontaneously within hours to a few weeks at the latest. However, if the damage is severe, the dilated state may persist. There is no radical treatment for traumatic mydriasis itself; for residual mydriasis, symptomatic treatment (reading glasses, sunglasses, iris-print contact lenses) or pupilloplasty may be considered.
2. Main Symptoms and Clinical Findings
Section titled “2. Main Symptoms and Clinical Findings”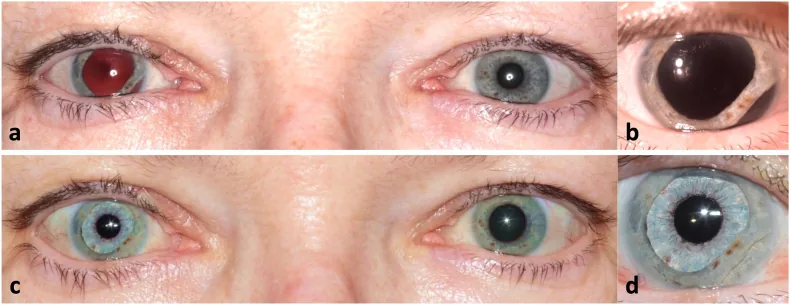
Subjective Symptoms
Section titled “Subjective Symptoms”In traumatic mydriasis, the main subjective symptoms are decreased near vision due to accommodative dysfunction and photophobia.
In the mydriatic state, a large amount of light enters the eye through the pupil, causing the sensation of glare (photophobia). Additionally, damage to the ciliary muscle or impairment of accommodative function makes it difficult to focus on near objects (accommodative dysfunction). This is perceived as decreased near vision.
Depending on the severity of the injury, complications such as hyphema (traumatic hyphema), traumatic iritis, iridodialysis, angle recession, lens subluxation, or dislocation may occur. These complications add further impairment to visual function.
Objective Findings
Section titled “Objective Findings”Slit-lamp examination reveals notched irregularity of the pupillary margin due to rupture of the pupillary sphincter. The dilated pupil is not round but shows irregular shape corresponding to the site of rupture, which is characteristic.
Both the light reflex and near reflex are diminished or absent. Because the sphincter is physically torn, the pupil does not constrict sufficiently even when parasympathetic constriction signals are transmitted.
| Finding | Characteristic |
|---|---|
| Pupil size | Dilated (often irregular/non-circular) |
| Light reflex | Diminished to absent |
| Near reflex | Decreased to absent |
| Pupillary margin | Notched irregularity (site of sphincter rupture) |
| Pilocarpine (1%) instillation response | No response to decreased response |
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”Types of Blunt Trauma
Section titled “Types of Blunt Trauma”Traumatic mydriasis is caused by a direct blow to the eye from blunt force. Common causes include:
- Sports injuries: Direct impact from high-speed objects such as baseballs, tennis balls, golf balls, or soccer balls
- Assault: Blows to the face or eye from a fist
- Traffic accidents: Collision with airbags or interior structures of a vehicle
- Falls: Impact of the face against the floor or ground
- Occupational injuries: Collision with tools or machinery
Associated Injuries
Section titled “Associated Injuries”In blunt trauma, damage to the pupillary sphincter is often accompanied by injury to multiple intraocular structures. Common associated injuries include hyphema, traumatic iritis, iridodialysis, angle recession, and lens damage (subluxation, traumatic cataract). It is necessary to systematically check for these.
4. Diagnosis and Examination Methods
Section titled “4. Diagnosis and Examination Methods”Examination Procedure
Section titled “Examination Procedure”The diagnosis of traumatic mydriasis is made by a combination of history taking, visual acuity testing, pupillary examination, and slit-lamp examination.
The most important items to check are the presence or absence of ptosis and ocular motility disorders. This is directly linked to differentiation from mydriasis due to oculomotor nerve palsy associated with head trauma, so it must be evaluated at the initial visit.
The standard examination procedure is as follows.
- Measurement of pupil diameter with the naked eye: Compare the pupil diameters of both eyes and check for irregular shape.
- Check light reflex and near response with a penlight: In traumatic mydriasis, both are diminished or absent.
- Swinging flashlight test: Check for the presence of a relative afferent pupillary defect (RAPD).
- Instillation of 1% pilocarpine hydrochloride (1% Sanpilo®): If the pupil does not constrict or the response is diminished after instillation, sphincter damage can be confirmed. A normal sphincter constricts in response to a cholinergic agent.
- Slit-lamp microscopy: Check for notched irregularity of the pupillary margin, and associated conditions such as hyphema, iritis, and iridodialysis.
The presence or absence of ptosis and ocular motility disorders is the key to differentiation. Oculomotor nerve palsy involves ptosis (drooping upper eyelid) and ocular motility disorders (limitation of adduction, elevation, and depression) in addition to mydriasis. Traumatic mydriasis generally does not involve ptosis or ocular motility disorders. If head trauma is present, neuro-ophthalmological evaluation should be prioritized.
In traumatic mydriasis, the pupillary sphincter is physically torn, so even if the parasympathetic nerve is stimulated with a cholinergic agent (pilocarpine), the sphincter cannot contract. In contrast, in Adie’s pupil, the structure of the sphincter itself is preserved, and even a lower concentration (0.1%) of pilocarpine causes miosis as a hypersensitivity reaction (cholinergic supersensitivity). This difference is useful for differential diagnosis.
Differential Diagnosis
Section titled “Differential Diagnosis”| Disease | Key Differentiating Points |
|---|---|
| Oculomotor nerve palsy | Accompanied by ptosis and ocular movement disorders (limitation of adduction, elevation, and depression). History of head trauma or cerebrovascular disease is important. |
| Adie’s pupil | Sluggish light reflex (tonic pupil). Shows miosis due to cholinergic supersensitivity with 0.1% pilocarpine eye drops. No history of trauma. |
| Pharmacologic mydriasis | Clear history of use or exposure to mydriatic agents (atropine, cyclopentolate, phenylephrine, etc.). |
5. Standard Treatment
Section titled “5. Standard Treatment”Treatment of Traumatic Mydriasis Itself
Section titled “Treatment of Traumatic Mydriasis Itself”There is no effective curative treatment for traumatic mydriasis itself. Since it is a structural injury with physical rupture of the sphincter, it is difficult to restore with pharmacotherapy.
The basic treatment strategy consists of the following two points.
- Symptom relief through symptomatic treatment
- Treatment of complications
Symptomatic treatment
Section titled “Symptomatic treatment”Symptomatic treatment is provided for each of the two main symptoms: decreased near vision due to accommodative dysfunction and photophobia.
Management of decreased near vision: Prescribe reading glasses to compensate for reduced accommodative function. The lens power is adjusted according to the degree of accommodative impairment.
Management of photophobia: Use tinted glasses to limit excessive light entry. Additionally, for cosmetic concerns, prescribing iris-colored contact lenses can artificially reduce the pupillary opening, potentially alleviating photophobia and improving appearance.
Treatment of complications
Section titled “Treatment of complications”If complications are present, treat each accordingly.
Traumatic iritis: Use steroid eye drops (e.g., fluorometholone 0.1–1%) and mydriatics (e.g., atropine 0.5–1% for cycloplegia). Adjust the frequency of instillation according to the degree of inflammation.
Hyphema: The mainstay is rest and head positioning (see the section on traumatic hyphema).
Lens subluxation or traumatic cataract: Choose observation or surgical treatment depending on severity.
Surgical options for residual mydriasis
Section titled “Surgical options for residual mydriasis”If mydriasis persists and causes significant photophobia or visual impairment, consider surgical pupilloplasty.
Pupilloplasty: Intraocular iris suturing techniques such as the Siepser slip-knot method, single-pass four-throw (SFT) method, and iris cerclage are used to constrict the pupil. Typically, 10-0 polypropylene suture is passed at about 8 points approximately 0.5 mm inside the pupillary margin, aiming for a target pupil diameter of 3.5–4.5 mm [³]. The Siepser slip-knot method has been reported to show the most significant visual improvement in traumatic mydriasis cases [⁴], and comparative studies have shown that the SFT method achieves comparable anatomical and visual outcomes to traditional multiple-knot techniques in a shorter time (approximately 22 minutes vs. 30 minutes) [⁵]. Recently, a novel iridoplasty method combining U-shaped sutures and Siepser slip-knot has also been reported [⁶]. Minimizing damage to the corneal endothelium is a common technical challenge.
Iris-claw intraocular lens (IOL): Although clinical experience is accumulating abroad, it is currently not approved in Japan. In cases of severe traumatic mydriasis complicated by traumatic cataract, it is expected to be a future treatment option.
6. Pathophysiology and Detailed Mechanisms
Section titled “6. Pathophysiology and Detailed Mechanisms”Intraocular Biomechanics from Blunt Force
Section titled “Intraocular Biomechanics from Blunt Force”When blunt force is applied to the eye, the following mechanical cascade occurs.
External force causes a rapid increase in anterior chamber pressure. This leads to stretching of the limbus and rapid movement of aqueous humor posteriorly and toward the angle. This sudden aqueous flow, along with direct stretching and shearing forces on the iris and ciliary body, results in rupture of the pupillary sphincter muscle.
In ball injuries, the ocular wall deforms, exerting combined forces of stretching and detachment on the iris and ciliary body attached to the inner surface. This mechanical stress causes microstructural damage, disruption of the blood-aqueous barrier, and migration of inflammatory cells into the anterior chamber (traumatic iritis). Simultaneously, the pupillary sphincter is damaged, leading to varying degrees of pupillary dilation (traumatic mydriasis).
Recent pathophysiological hypotheses, in addition to the traditional model of equatorial expansion due to anteroposterior compression (Duke-Elder’s classical theory), suggest that the rapid fluid flow through the pupil during corneal deformation exerts horizontal mechanical stretching forces that rupture the pupillary sphincter [¹].
Continuum of Tissue Damage
Section titled “Continuum of Tissue Damage”Traumatic iris and pupillary disorders form a continuous spectrum depending on injury severity.
- Mild: Traumatic iritis only. Temporary disruption of the blood-aqueous barrier. No sphincter damage.
- Moderate: Traumatic mydriasis. Partial to complete rupture of the sphincter. Irregular and dilated pupil.
- Severe: Iridodialysis. Tear at the iris root. Associated with pupillary deviation (see section on iridodialysis).
- Very severe: Angle recession and cyclodialysis. Structural destruction of the trabecular meshwork and ciliary body. Risk of secondary glaucoma.
Mechanism of Accommodation Dysfunction
Section titled “Mechanism of Accommodation Dysfunction”Accommodative disorders associated with traumatic mydriasis result from damage or inflammation of the ciliary muscle itself, or from temporary disruption of neural transmission to the ciliary muscle. The ciliary body adjusts the thickness of the lens; during near vision, the ciliary muscle contracts to thicken the lens. When this function is impaired, focusing on near objects becomes difficult.
Sphincter Rupture and Drug Responsiveness
Section titled “Sphincter Rupture and Drug Responsiveness”A normal sphincter constricts in response to parasympathomimetic drugs (e.g., pilocarpine). In traumatic mydriasis, because the sphincter is physically torn, sufficient miosis cannot be achieved even with cholinergic agents. The finding that 1% pilocarpine eye drops produce no or markedly reduced miosis serves as functional evidence of this structural rupture and has diagnostic significance.
Prognosis and Recovery Process
Section titled “Prognosis and Recovery Process”Visual prognosis is generally good. Most cases recover within hours to a few weeks at most, but if the sphincter rupture is severe, the mydriatic state may persist. Persistent mydriasis leads to continued photophobia and accommodative dysfunction, as well as cosmetic issues (irregular pupil shape). However, even in long-standing cases, improvement in pupillary response and accommodative function has been reported several years after injury, so symptoms are not necessarily permanent [²].
7. Latest Research and Future Perspectives
Section titled “7. Latest Research and Future Perspectives”Technological Advances in Pupilloplasty
Innovations in intraocular iris suturing techniques are enabling less invasive and more precise pupil reduction. The combination of ultra-small curved needles (1.5 mm) and specialized needle holders minimizes damage to the corneal endothelium. Several surgical methods, such as the Siepser method and the SFT method, have been reported, and selecting the appropriate technique according to the case morphology is important.
Artificial Iris
Experience with artificial iris devices for severe iris damage or aniridia is accumulating abroad. Inserting a silicone artificial iris into the eye can reduce photophobia and provide cosmetic improvement. Although not yet approved in Japan, it is one of the options expected to be introduced in the future.
Application of Iris-Claw IOLs
For cases of traumatic mydriasis complicated by traumatic cataract, simultaneous cataract surgery and miosis using an iris-claw intraocular lens have been reported overseas. Although currently not approved in Japan, this approach is attracting attention as a comprehensive surgical solution for complex anterior segment trauma.
8. References
Section titled “8. References”- Pujari A, Agarwal D, Behera AK, Bhaskaran K, Sharma N. Pathomechanism of iris sphincter tear. Med Hypotheses. 2019;122:147-149. doi:10.1016/j.mehy.2018.11.013. PMID: 30593400.
- Thuma TBT, Bello NR, Rapuano CJ, Wasserman BN. Resolution of traumatic mydriasis and accommodative dysfunction eight years after sweetgum ball ocular injury. Am J Ophthalmol Case Rep. 2022;26:101552. doi:10.1016/j.ajoc.2022.101552. PMID: 35509280; PMCID: PMC9058597.
- Lumi X, Lumi A, Petrovic Pajic S. Iris cerclage pupilloplasty and IOL implantation for traumatic mydriasis and aphakia after the blunt trauma of the eye. Indian J Ophthalmol. 2021;69(5):1314-1317. doi:10.4103/ijo.IJO_1913_20. PMID: 33913887; PMCID: PMC8186584.
- Nowomiejska K, Haszcz D, Adamczyk K, Brzozowska A, Bonfiglio V, Toro MD, Rejdak R. Visual Outcomes of Pupilloplasty in Ocular Trauma and Iatrogenic Damage. J Clin Med. 2022;11(11):3177. doi:10.3390/jcm11113177. PMID: 35683581; PMCID: PMC9181509.
- Shen C, Liu L, Su N, Cui L, Zhao X, Li M, Zhong H. Single-pass four-throw versus traditional knotting pupilloplasty for traumatic mydriasis combined with lens dislocation. BMC Ophthalmol. 2023;23:13. doi:10.1186/s12886-023-02773-z. PMID: 36624415; PMCID: PMC9830823.
- Karabaş VL, Seyyar SA, Onder Tokuc E, Şahin Ö. A novel iridoplasty suture technique to repair iris defects and traumatic mydriasis. Indian J Ophthalmol. 2023;71(5):2254-2256. doi:10.4103/ijo.IJO_1910_22. PMID: 37202963; PMCID: PMC10391397.