Pharmacologic dilation of the pupil is a condition in which exogenous drugs cause unilateral or bilateral mydriasis. The pupillary light reflex and near reflex are impaired or absent.
The most common mechanism is anticholinergic mydriasis, caused by blockade of muscarinic receptors in the iris sphincter muscle. Sympathomimetic stimulation (adrenergic mydriasis) can also cause dilation, but in that case the light and near reflexes are relatively preserved, which is an important difference from anticholinergic mydriasis.
Normal pupil diameter indoors averages about 4 mm, but varies widely from 2 to 6 mm. About 20% of normal individuals have physiologic anisocoria (difference of 0.5–1.0 mm or less), so mild pupillary asymmetry alone should not be considered pathologic.
QIs a single dilated pupil always abnormal?
A
Approximately 20% of normal individuals have physiologic anisocoria (a difference of 1.0 mm or less between the two pupils), and if there are no other abnormal findings, it is of low pathological significance. However, if accompanied by ptosis, eye movement disorder, or headache, oculomotor nerve palsy should be suspected and emergency treatment is required. For details, see the section “Diagnosis and Examination Methods”.
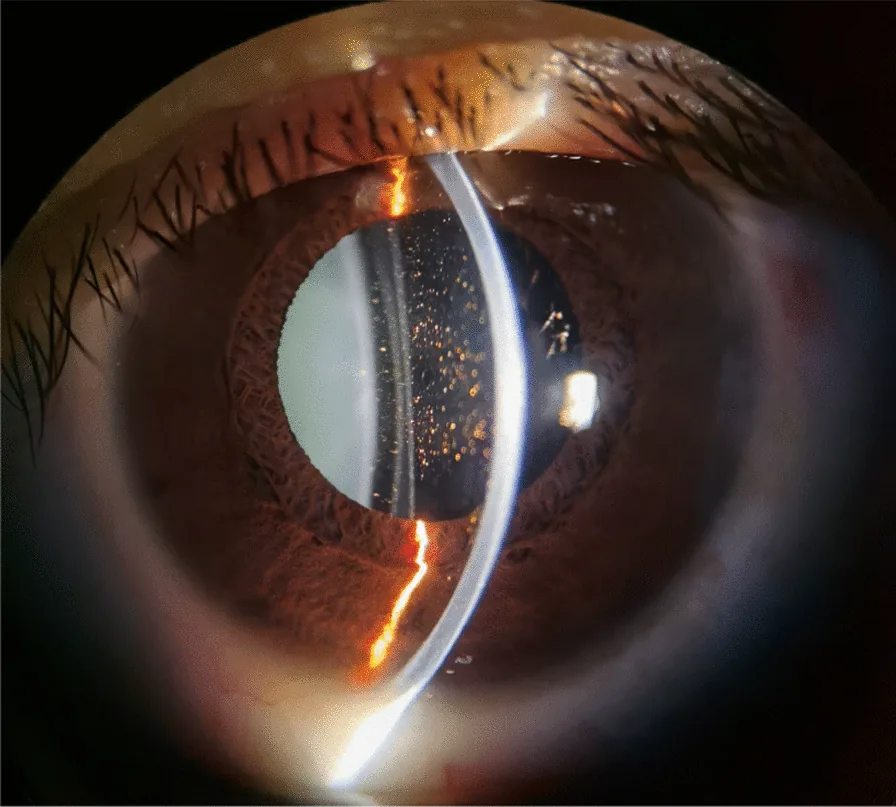
Urrets-Zavalia syndrome following implantable collamer lens (ICL) implantation: a case report and review of the literature. J Med Case Rep. 2025 May 12; 19:219. Figure 1. PMCID: PMC12070703. License: CC BY.
One day after the left eye surgery, the pupil dilated and fixed, with more pigments in the anterior chamber
Blurred vision (hazy vision): If accompanied by cycloplegia, difficulty in near vision and eye strain may also occur.
Often asymptomatic: Some patients only notice mydriasis when pointed out by others.
In cases of systemic anticholinergic poisoning: Accompanied by systemic symptoms such as palpitations, shortness of breath, constipation, urinary retention, memory impairment, and visual hallucinations.
Clinical Findings (Findings Confirmed by Physician Examination)
Knowing the maximum time to achieve mydriasis and the duration of effect for each mydriatic is directly linked to explaining to patients when their pupils will return to normal.
Touching the eyes with fingers after handling anticholinergic drugs (healthcare workers, scopolamine patch users)
Leakage into the eyes from poorly fitting nebulizer treatment masks
Mild mydriasis due to d-chlorpheniramine maleate (over-the-counter cold and allergy medications)
QCan systemic side effects occur after instilling mydriatic eye drops?
A
Atropine may cause increased blood pressure, palpitations, dry mouth, facial flushing, hallucinations, and agitation. In infants and young children, systemic absorption can easily lead to atropine poisoning symptoms such as facial flushing, dry mouth, and tachycardia, so caution is necessary. Cyclopentolate has been reported to cause transient neuropsychiatric symptoms such as dizziness, ataxia, disorientation, drowsiness, and hallucinations.
Obtain a detailed history of the use of mydriatic eye drops, nasal sprays, scopolamine patches, and anticholinergic drugs. When considering drug intoxication, keep in mind the presence of the blood-aqueous barrier and the special characteristics of intraocular migration due to binding with melanin pigment.
Check for anisocoria: Observe in both bright and dark rooms. In the affected eye with mydriasis, anisocoria becomes more apparent under bright light.
Check pupillary light reflex: In a semi-dark room, shine a penlight and observe the direct reflex (constriction of the illuminated eye) and the indirect reflex (constriction of the non-illuminated eye). Assess the speed and extent of the response.
Check near response: Present a target about 30 cm in front of the eyes and observe whether constriction occurs along with convergence.
Check for ptosis and limitation of eye movement: These are essential for differentiating from oculomotor nerve palsy.
Pilocarpine Eye Drop Test (Stepwise Pharmacological Diagnosis)
Pilocarpine is a drug that directly stimulates cholinergic receptors of the sphincter pupillae muscle to induce miosis. Perform the test stepwise in the following order.
If miosis occurs, suspect tonic pupil (Adie pupil). Denervation supersensitivity causes miosis even at low concentrations that normally do not produce a response.
Step 2: If no miosis with low concentration, instill 1% pilocarpine
Miosis present → Possible compressive lesion of the third cranial nerve (oculomotor nerve). Urgently rule out posterior communicating artery aneurysm with high-resolution CTA or MRI/MRA.
No miosis (and both light reflex and near reflex are absent) → Diagnose pharmacologic pupil.
Exception: Mydriasis due to botulinum toxin poisoning will constrict with 1% pilocarpine in step 2. Because the inhibition is presynaptic, the receptor side is normal. Be careful not to confuse this with pharmacologic pupil.
QWhat is the most important cause to consider when the pupil remains dilated and does not return to normal?
A
Oculomotor nerve palsy with mydriasis, particularly due to an aneurysm at the junction of the internal carotid artery and posterior communicating artery, is a highly urgent cause. If accompanied by ptosis or limitation of eye movement, it may be life-threatening, and urgent evaluation with high-resolution CTA or MRI/MRA is necessary.
If anticholinergic or adrenergic mydriasis is diagnosed, the pupil and visual acuity (accommodation) will recover naturally as the effect of the causative agent wears off. Reassuring the patient by explaining this is the starting point of treatment. For specific duration of effect, refer to the table in the section Characteristics of Mydriatic Agents.
After discontinuing the causative agent, perform regular follow-up to confirm recovery to baseline.
If mydriasis persists after a sufficient washout period, reassess other causes (e.g., oculomotor nerve palsy, tonic pupil).
QWhen can I drive after using mydriatic eye drops?
A
The duration of mydriasis varies greatly by drug. For tropicamide, it is about 5–8 hours; for phenylephrine, about 5 hours; but for atropine, mydriasis can persist for up to 10 days, so driving should be avoided until the effect has completely resolved.
The iris muscles consist of two types of smooth muscle.
Sphincter pupillae: Innervated by the oculomotor nerve (parasympathetic). Contraction causes miosis.
Dilator pupillae: Innervated by the sympathetic nervous system. Contraction causes mydriasis.
Parasympatholytic drugs (anticholinergics) relax the sphincter pupillae, causing mydriasis. Sympathomimetic drugs contract the dilator pupillae, but their effect is weaker than that of parasympatholytics.
Retinal photoreceptors → retinal ganglion cells → optic nerve → optic chiasm → leaves the visual pathway just before the lateral geniculate body → pretectal area → Edinger-Westphal (EW) nucleus → oculomotor nerve → cavernous sinus → orbit → ciliary ganglion → short ciliary nerves → intraocular (iris sphincter muscle).
95% of the parasympathetic fibers from the EW nucleus go to the ciliary muscle (accommodation), and only 5% go to the pupillary sphincter (light reflex). This ratio is also involved in the pathogenesis of light-near dissociation in Adie’s pupil.
Anticholinergic mydriasis: Blocks muscarinic acetylcholine receptors on the iris sphincter. Atropine has a high affinity for melanin pigment, so it takes time to take effect, but once it does, it lasts a long time.
Adrenergic mydriasis: Sustained contraction due to overstimulation of α1 receptors on the iris dilator muscle. Cocaine inhibits norepinephrine reuptake, and amphetamine promotes norepinephrine release, causing mydriasis.
Botulinum toxin-induced mydriasis: Presynaptic inhibition of acetylcholine release from short ciliary nerve terminals. Since the receptors themselves are normal, miosis can be achieved with 1% pilocarpine eye drops.
Special characteristics of intraocular drug penetration
Blood-aqueous barrier and blood-retinal barrier: Some drugs have limited intraocular penetration.
Binding to melanin pigment: Drugs such as atropine bind strongly to melanin, delaying the onset of action but increasing its duration.
Corneal barrier: The corneal epithelium and endothelium are hydrophilic, while the stroma is hydrophobic, forming the major barrier to intraocular penetration of eye drops. Once passed, the drug remains in the eye for a long time.
Hong D, Tripathy K. Tropicamide. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024. PMID: 31082113 / Bookshelf ID: NBK541069
Payne WN, Blair K, Barrett MJ. Anisocoria. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. Bookshelf ID: NBK470384
Yoo YJ, Hwang JM, Yang HK. Dilute pilocarpine test for diagnosis of Adie’s tonic pupil. Sci Rep. 2021;11(1):10089. doi:10.1038/s41598-021-89148-w. PMID: 33980910 / PMCID: PMC8115311
Joo JH. Anisocoria after scopolamine transdermal patch contamination: A case report. Medicine (Baltimore). 2021;100(46):e27887. doi:10.1097/MD.0000000000027887. PMID: 34797334 / PMCID: PMC8601308
Yang MC, Lin KY. Drug-induced Acute Angle-closure Glaucoma: A Review. J Curr Glaucoma Pract. 2019;13(3):104-109. doi:10.5005/jp-journals-10078-1261. PMID: 32435123 / PMCID: PMC7221246
Friedman DS, Chang DS, Jiang Y, et al. Acute Angle-Closure Attacks Are Uncommon in Primary Angle-Closure Suspects after Pharmacologic Mydriasis: The Zhongshan Angle-Closure Prevention Trial. Ophthalmol Glaucoma. 2022;5(6):581-586. doi:10.1016/j.ogla.2022.04.003. PMID: 35568336
Deeks ED. Tropicamide/Phenylephrine/Lidocaine Intracameral Injection: A Review in Cataract Surgery. Clin Drug Investig. 2019;39(11):1133-1139. doi:10.1007/s40261-019-00843-z. PMID: 31471864
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.