Uveal coloboma is a congenital eye anomaly caused by failure of closure of the embryonic fissure. The defect occurs in the optic disc, choroid, ciliary body, and iris along the embryonic fissure. Defects occurring on the lower side of the optic cup are called typical colobomas, while those in other locations (such as macular coloboma) are called atypical colobomas.
Typical iris coloboma results from failure of closure of the optic cup fissure. The optic cup surrounds the tissue that will become the contents of the eye by folding in from above, finally closing on the lower side. Therefore, typical iris coloboma is located inferiorly (slightly inferotemporally) and may be accompanied by ciliary bodycoloboma, choroidal coloboma, and optic nervecoloboma. Iris coloboma can occur alone, but it is often combined with other uveal colobomas.
Currently, there is no treatment that can “cure” iris coloboma itself. The goals of treatment are symptomatic management of photophobia, management and prevention of complications, and optimization of visual function.
0.5 to 0.7 per 10,000 births (genetic epidemiological study 1))
Incidence (population-based, Minnesota, USA)
2.6 per 10,000 births 9)
Bilateral rate
Approximately 50% 1)
Inheritance pattern
Sporadic, autosomal dominant (AD), autosomal recessive (AR), etc., diverse
Associated syndromes
May be found as a symptom of multi-organ malformations such as CHARGE syndrome (CHD7 mutation)
QIs iris coloboma hereditary?
A
The inheritance pattern is diverse; it may occur sporadically or as an autosomal dominant (AD) or recessive (AR) trait with multiple affected family members. It can also appear as a symptom of a multiple malformation syndrome such as CHARGE syndrome (CHD7 mutation, AD). Genetic counseling is recommended if there is a family history or if a syndromic condition is suspected.
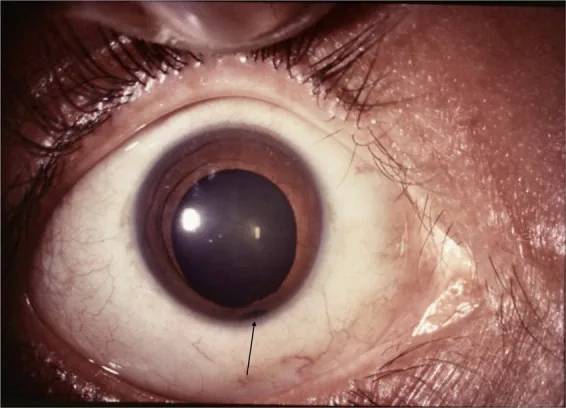
Lingam G, et al. Ocular coloboma-a comprehensive review for the clinician. Eye (Lond). 2021. Figure 2. PMCID: PMC8302742. License: CC BY.
Anterior segment photograph clearly shows an iris defect with a keyhole-shaped notch in the lower part of the pupil. This represents a typical clinical finding of iris coloboma and is suitable for explaining the main symptoms and clinical findings.
Visual acuity: In many cases of isolated iris coloboma, visual acuity is good. If the defect extends to the macula, visual acuity becomes poor.
Photophobia (sensitivity to light): The defect in the iris causes impaired light regulation, leading to photophobia. This can cause significant discomfort in daily life.
Nystagmus: Nystagmus may be present in bilateral cases. It is particularly noticeable in cases with poor visual acuity.
The defect is located inferotemporally, widest at the pupillary margin and narrowing toward the root (keyhole pupil). It is often accompanied by microphthalmia, cataract, and choroidal coloboma.
Appearance: Keyhole-shaped pupil deformity. Widest at the pupillary margin and narrowing toward the root.
Main symptoms: Photophobia due to impaired light regulation. Visual acuity is often good in isolated defects.
Ciliary Body Coloboma
Location: Often continuous with iris coloboma.
Features: Rarely occurs alone. Often continuous with large choroidal coloboma. Epithelium and muscle are absent.
Complications: Weakening of the zonules of Zinn. Reduced lens support.
Choroidal Coloboma
Findings: Observed as a well-demarcated, depressed yellowish-white lesion in the inferior fundus.
Complications: Retinal tear formation at the edge of the defect → high risk of retinal detachment. Involvement of the macula leads to poor visual prognosis.
Optic Nerve Coloboma
Findings: Enlargement and cupping of the optic disc. The defect extends around the disc.
Complications: Visual field defects and optic atrophy. Significant impact on vision.
According to the phenotypic classification by Hornby et al., the extent of coloboma involvement in the posterior segment is a major factor determining visual prognosis; the more the defect extends to the macula, the worse the visual prognosis8).
QHow does iris coloboma affect vision?
A
If iris coloboma occurs alone, vision is often good. However, if choroidal coloboma extends to the macula, vision decreases significantly and the prognosis is poor. Bilateral cases may be accompanied by nystagmus and amblyopia. Regular ophthalmologic follow-up to monitor vision and fundus findings is important.
Around the 6th to 7th week of gestation, closure of the embryonic fissure (optic fissure/choroidal fissure) occurs. Closure begins at the inferior equator and progresses bidirectionally toward the posterior pole and the periphery. Therefore, defects tend to remain in the posterior pole choroid and the inferior iris. If closure is incomplete, defects form in the inferior uvea (iris, ciliary body, choroid) and the optic nerve.
Regarding environmental factors, animal experiments have reported the involvement of teratogenic substances, but established risk factors in humans are limited2).
CHARGE syndrome is a multiple organ malformation syndrome caused by mutations in the CHD7 gene. Its name is derived from the acronym of its main features: Coloboma, Heart defects, Atresia choanae, Retardation of growth/development, Genital anomalies, and Ear anomalies. It is inherited in an autosomal dominant pattern, and coloboma is often the initial clue for diagnosis. Multidisciplinary collaboration is required for systemic management.
Slit-lamp microscopy: Observation of the anterior segment reveals an inferior iris defect (keyhole pupil). This is the main finding for definitive diagnosis.
Dilated fundus examination: Confirms the presence of choroidal coloboma and optic nervecoloboma. Assesses whether the macula is involved.
Differentiation from aniridia is clinically important. The diagnostic criteria for aniridia (Jpn J Ophthalmol 2020) explicitly list iris coloboma as a differential diagnosis4).
PAX6 mutation. Iris is almost completely absent (>2/3). Often associated with keratopathy and macular hypoplasia4). Risk of Wilms tumor (WAGR syndrome) is specific to aniridia and is not usually present in iris coloboma.
Traumatic iris dialysis
History of trauma. Irregular iris tear with the site of injury corresponding to the trauma.
Membranous structure remains in the pupillary area. Iris stroma is not deficient.
QWhen and how is iris coloboma discovered?
A
It is often discovered as a keyhole-shaped pupil during anterior segment examination at birth or in infancy. Diagnosis is confirmed by slit-lamp microscopy, and dilated fundus examination checks for involvement of the choroid and optic nerve. If CHARGE syndrome is suspected, systemic evaluation of the heart, ears, and nose is performed. It may also be found incidentally during school or well-child checkups.
There is no curative treatment for iris coloboma itself. Symptomatic treatment for photophobia, the main symptom, is the starting point of therapy.
Tinted glasses: The most basic measure to compensate for light regulation impairment due to iris coloboma and reduce photophobia. The degree of tint and color filter are selected according to symptoms.
Colored contact lenses with artificial iris (prosthetic CL): Can achieve both cosmetic improvement and photophobia reduction. Optically compensates for the iris defect.
Refractive correction: Correct refractive errors with glasses or regular contact lenses.
Amblyopia prevention: In children, appropriate refractive correction and occlusion of the healthy eye are important to prevent amblyopia and strabismus.
Procedure: Phacoemulsification + IOL implantation. Consider using a capsular tension ring (CTR). Pupil expansion devices (e.g., Malyugin ring) may be necessary.
Options: Consider simultaneous implantation of an artificial iris (e.g., Customflex Artificial Iris) 5). This can improve cosmetic appearance and reduce photophobia.
Glaucoma Treatment
Medical therapy: Use intraocular pressure-lowering eye drops such as prostaglandin analogs, beta-blockers, and carbonic anhydrase inhibitors.
Surgery: Consider trabeculotomy or trabeculectomy (filtering surgery) in cases resistant to medical therapy.
Follow-up: Since glaucoma causes irreversible visual field damage, regular intraocular pressure monitoring and visual field testing are essential.
Retinal Detachment Treatment
Pathology: May be due to retinal tears within or at the edge of a choroidal coloboma, or tears unrelated to the coloboma.
Treatment: Vitrectomy is the standard. Prophylactic laser photocoagulation at the edge of the choroidal coloboma has been reported to be useful 6).
Prognosis: Cases with retinal detachment often have poor outcomes. Early detection and treatment are important.
Regular Follow-up
Target complications: Regular follow-up is essential for the three major complications: glaucoma, cataract, and retinal detachment.
Pediatric management: Regular assessment for amblyopia, strabismus, and ocular motility abnormalities is also important.
Follow-up frequency: Continue ophthalmology visits every 3 to 12 months depending on the condition and age.
QCan iris coloboma be treated with surgery?
A
There is no surgery to cure iris coloboma itself. The goal of treatment is symptomatic relief for photophobia and management of complications. If cataracts are present, phacoemulsification and intraocular lens implantation are performed, but the risk is high due to zonular weakness. Artificial iris (Customflex Artificial Iris) is an effective option for cosmetic improvement and reduction of photophobia. If glaucoma or retinal detachment occurs, respective surgical treatments are performed.
During embryonic eye development, the optic fissure forms after the optic cup. Around the 6th to 7th week of gestation, closure of the optic fissure begins at the inferior equator and proceeds bidirectionally toward the posterior pole and periphery. If closure is incomplete, defects form in the inferior uvea (iris, ciliary body, choroid) and optic nerve.
Closure of the optic fissure requires coordinated regulation of basement membrane remodeling, cell proliferation, and apoptosis7). Any disruption in this complex process can lead to coloboma.
Closure of the optic fissure involves coordinated action of various molecular signals such as SHH (Sonic Hedgehog), PAX2, BMP, and retinoic acid 7). In animal models such as zebrafish and mice, mutations in pax2, shh, and vsx2 reproduce coloboma7). These studies are elucidating the overall molecular mechanism of optic fissure closure.
In choroidal coloboma, histologically, the pigment epithelium and choriocapillaris are absent, and dysplastic neuroretina is present. Degenerated retinal tissue exists at the margin of the defect, posing a risk for retinal tear formation. This histological characteristic forms the pathophysiological basis for the high risk of retinal detachment.
Visual prognosis is often good in isolated iris coloboma, but worsens as choroidal coloboma extends to the posterior pole or macula. Bilateral cases may present with nystagmus and carry a risk of amblyopia. Additionally, retinal detachment occurs in a significant number of cases, due to retinal tears within or along the margin of the choroidal coloboma, as well as tears unrelated to the coloboma. Cases with retinal detachment often have poor prognosis.
Advances in genetic diagnosis: Comprehensive analysis of coloboma-related genes using next-generation sequencing (NGS) panel testing is becoming widespread 2). In collaboration with genetic counseling, the accuracy of family prognosis prediction has improved.
Concept of MAC spectrum: The concept of comprehensively understanding microphthalmia, anophthalmia, and coloboma as an integrated MAC spectrum is advancing 10). Genetic and phenotypic overlaps among these conditions are becoming clearer.
Widespread use of artificial iris: The Customflex Artificial Iris (HumanOptics) received FDA approval in 2018 5) and is now used as an option for cosmetic improvement and photophobia reduction in iris defects. Continued accumulation of usage data in Japan is expected.
Gene therapy: Direct gene therapy for coloboma is still in the basic research stage and has not yet reached clinical application.
iPS cell research: Basic research on retinal regeneration and iris reconstruction using iPS cells is ongoing, and future clinical applications are anticipated.
Morrison D, FitzPatrick D, Hanson I, et al. National study of microphthalmia, anophthalmia, and coloboma (MAC) in Scotland: investigation of genetic aetiology. J Med Genet. 2002;39(1):16-22. PMID: 11826019
Gregory-Evans CY, Williams MJ, Halford S, Gregory-Evans K. Ocular coloboma: a reassessment in the age of molecular neuroscience. J Med Genet. 2004;41(12):881-891. PMID: 15591273
Pagon RA, Graham JM Jr, Zonana J, Yong SL. Coloboma, congenital heart disease, and choanal atresia with multiple anomalies: CHARGE association. J Pediatr. 1981;99(2):223-227. PMID: 6166737
Mayer CS, Laubichler AE, Khoramnia R, et al. Challenges and complication management in novel artificial iris implantation. J Ophthalmol. 2018;2018:3262068. PMID: 30345111. doi:10.1155/2018/3262068.
Gopal L, Badrinath SS, Kumar KS, et al. Optic disc in fundus coloboma. Ophthalmology. 1996;103(12):2120-2127. PMID: 9003347
Patel A, Sowden JC. Genes and pathways in optic fissure closure. Semin Cell Dev Biol. 2019;91:55-65. doi:10.1016/j.semcdb.2017.10.010. PMID:29198497.
Hornby SJ, Adolph S, Gilbert CE, et al. Visual acuity in children with coloboma: clinical features and a new phenotypic classification system. Ophthalmology. 2000;107(3):511-520. PMID: 10711890
Nakamura KM, Diehl NN, Mohney BG. Incidence, ocular findings, and systemic associations of ocular coloboma: a population-based study. Arch Ophthalmol. 2011;129(1):69-74. PMID: 21220631
Skalicky SE, White AJ, Grigg JR, Martin F, Smith J, Jones M, et al. Microphthalmia, anophthalmia, and coloboma and associated ocular and systemic features: understanding the spectrum. JAMA Ophthalmol. 2013;131(12):1517-24. doi:10.1001/jamaophthalmol.2013.5305. PMID:24177921.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.