Angle-closure glaucoma (ACG) is a group of diseases in which aqueous humor outflow is obstructed due to appositional or synechial closure of the anterior chamber angle, leading to elevated intraocular pressure and optic nerve damage1)2). Both primary and secondary types can present with acute attacks or a chronic course.
The prevalence increases after age 401)4). In the Tajimi Study, the prevalence of PACG was 0.6%, while in the Kumejima Study it was 2.2%, showing regional differences. The prevalence is particularly high in East Asian and Inuit populations4). It is more common in women4).
QWhy does the prevalence of primary angle-closure glaucoma vary by region?
A
The prevalence of primary angle-closure glaucoma varies greatly among races and ethnic groups4). The highest prevalence has been reported in East Asian and Inuit populations4). This is thought to be due to racial differences in anatomical features such as axial length, anterior chamber depth, lens thickness, and corneal curvature. Even within Japan, there are regional differences, with about a 3.7-fold difference between Tajimi (0.6%) and Kumejima (2.2%).
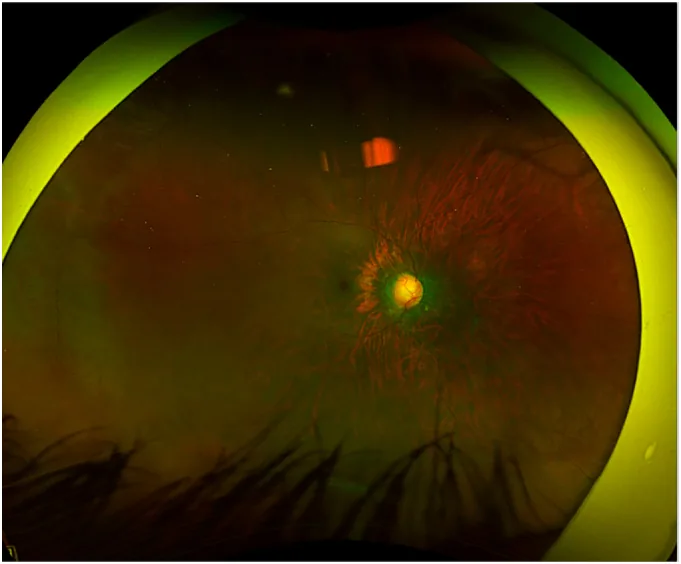
Bamefleh DA, et al. Bleb morphology following mitomycin-C sponge versus subconjunctival injection in deep sclerectomy for pediatric congenital glaucoma: A case report. Int J Surg Case Rep. 2025. Figure 1. PMCID: PMC12510068. License: CC BY.
A wide-angle fundus photograph of the right eye showing optic disc cupping due to progression of glaucoma, seen before a repeat deep sclerectomy. This corresponds to the optic disc cupping discussed in section “2. Main Symptoms and Clinical Findings.”
In cases of only anatomically narrow angles or chronic angle closure, there are usually no symptoms. Visual acuity loss and visual field defects are only noticed at the end stage.
Acute angle-closure attacks present with dramatic symptoms1)2). Visual acuity loss, blurred vision, and iridescent vision (halos around lights) occur1)2). It is accompanied by severe eye pain and headache, and may cause vagal symptoms such as nausea and vomiting1)2).
Secondary causes are diverse1)2). They are broadly divided into mechanisms that push the iris forward from behind (e.g., lens swelling, lens dislocation, ciliochoroidal effusion, aqueous misdirection, posterior segment tumors) and those that pull the iris into contact with the trabecular meshwork (e.g., contraction of inflammatory membranes, ICE syndrome, fibrous proliferation).
In drug-induced ACG, sulfonamide drugs such as topiramate cause ciliochoroidal effusion, leading to anterior rotation of the ciliary body and forward movement of the iris-lens diaphragm, resulting in angle closure6)7)8). Acetazolamide has also been reported to cause a similar idiosyncratic reaction10).
QHow does topiramate-induced angle-closure glaucoma develop?
A
Topiramate causes ciliochoroidal effusion, leading to anterior rotation of the ciliary body and forward movement of the iris-lens diaphragm, resulting in bilateral acute angle closure 6)7)8). It often occurs within two weeks of starting the medication, but can also occur after discontinuation 6). UBM shows anterior rotation of the ciliary body and choroidal effusion 8). Treatment includes discontinuation of topiramate, atropine eye drops, steroid eye drops, and intraocular pressure-lowering medications 6)7). Laser iridotomy is ineffective, and miotics are contraindicated as they worsen the condition.
Gonioscopy is the gold standard for diagnosing ACG 1)2). Indentation gonioscopy is used to differentiate appositional closure from synechial closure. In primary ACG, PAS tends to form superiorly, while in secondary inflammatory ACG, PAS tends to form inferiorly.
UBM (ultrasound biomicroscopy) can evaluate the morphology and position of the ciliary body and the presence of choroidal effusion, and is useful for investigating the cause of secondary ACG 8)10). Anterior segment OCT is used for objective quantitative assessment of angle structures.
The van Herick method for assessing anterior chamber depth is a simple screening method for narrow angles 1). If the ratio of corneal thickness to peripheral anterior chamber depth is less than 1/4, gonioscopy should be performed 1).
If drug-induced ACG is suspected, UBM and B-scan should be performed to confirm ciliochoroidal effusion 6)8)10). If retinitis pigmentosa is suspected, full-field electroretinography should be performed 5). In ARB (autosomal recessive bestrophinopathy), EOG shows characteristic loss of light rise 9).
LPI is the first-line treatment effective for relieving pupillary block1)2). It is performed when the cornea is sufficiently clear1). Laser irradiation through an opaque cornea carries a risk of bullous keratopathy1). If primary angle-closure glaucoma/primary angle closure is diagnosed in one eye, prophylactic LPI is performed on the fellow eye1).
Lens extraction fundamentally resolves pupillary block1). It achieves angle widening and intraocular pressure reduction1). If peripheral anterior synechiae (PAS) are extensive, the intraocular pressure-lowering effect is limited1).
For plateau iris, LPI alone is insufficient; laser iridoplasty (laser peripheral iridoplasty) is used to contract the iris root1). Lens extraction to widen the angle is also effective1).
In secondary ACG, treatment of the underlying cause is the highest priority 1)2). For drug-induced cases, discontinuation of the causative drug is most important, along with cycloplegia using atropine eye drops and anti-inflammatory therapy with steroids 6)7)8). Miotics are contraindicated because they promote forward movement of the lens. In malignant glaucoma, atropine eye drops and vitrectomy are the mainstays of treatment 1).
QWhat is the effect of lens extraction on primary angle closure glaucoma?
A
Lens extraction is effective for fundamentally resolving pupillary block1). Removing the lens deepens the anterior chamber and widens the angle. In cases with cataract surgery indication, a two-in-one effect can be expected. However, if extensive PAS has formed, the intraocular pressure-lowering effect is limited, and combined goniosynechialysis is recommended 1). Lens extraction in the acute phase carries high complication risk and should be performed by an experienced surgeon 1).
Most primary angle closure glaucoma is due to relative pupillary block1)2)3). Increased resistance to aqueous humor flow from the posterior chamber to the anterior chamber causes the iris to bow forward and obstruct the trabecular meshwork1). The risk of pupillary block is greatest during moderate pupillary dilation 3).
The pathogenesis of primary angle closure involves multiple mechanisms 1): (1) relative pupillary block, (2) plateau iris, (3) lens factors (increased lens thickness with age), and (4) retrolenticular factors (ciliary body, choroid, vitreous) 1).
In plateau iris configuration, anteriorly positioned ciliary processes push the iris root forward, causing angle closure despite normal central anterior chamber depth 1).
Pupillary block type: Forward pushing of the iris due to lens intumescence, lens dislocation, or microspherophakia2)3). Absolute pupillary block due to posterior synechiae 2)
Ciliochoroidal type: Ciliochoroidal effusion and anterior rotation of the ciliary body caused by medications (topiramate) 6)7)8). Pushing due to posterior segment tumors or serous retinal detachment
Aqueous misdirection type: Forward displacement of the vitreous leads to overall shallowing of the anterior chamber. Also called malignant glaucoma1)
Pulling Mechanism
Contraction of inflammatory membranes: PAS formation associated with uveitis. Contraction of fibrovascular membranes due to iris neovascularization2)
ICE syndrome: Trabecular meshwork obstruction due to abnormal proliferation of corneal endothelium1)
Trauma/surgery-related: Epithelial ingrowth, fibrous proliferation, iris incarceration into the wound 2)
Lu et al. reported three young patients with retinitis pigmentosa (RP) who developed PACG5). The risk of developing ACG is 3.64 times higher in RP patients compared to the general population 5). Short axial length, increased lens thickness, and zonular weakness are anatomical predispositions for ACG 5). A novel mutation in the ZNF408 gene was identified in RP patients with PACG5). Regular gonioscopy and intraocular pressure monitoring are recommended for RP patients 5).
Multiple case reports of topiramate-induced ACG have been accumulated 6)7)8). Typical cases present bilaterally 1–2 weeks after starting the medication, with ciliochoroidal effusion and subsequent anterior rotation of the ciliary body as the mechanism 8). Tyagi et al. reported two cases presenting with uveitis with hypopyon and choroidal detachment, demonstrating that topiramate can cause severe intraocular inflammation 7). It has been reported that onset can occur even after discontinuation 6).
In a literature review by Kaisari et al., 23 cases of acetazolamide-induced myopia have been reported since 1956 10). Onset occurs at a median of 24 hours after a median dose of 500 mg, and about one-third are complicated by angle closure 10). This reaction is a dose-independent idiosyncratic reaction and can occur even with the first dose 10). Complete recovery occurs at a median of 5 days after drug discontinuation and cycloplegic therapy 10).
More than 50% of autosomal recessive bestrophinopathy (ARB) cases are complicated by angle-closure glaucoma9). Raja et al. reported a 38-year-old woman with ARB-associated ACG and advanced optic neuropathy, in whom intraocular pressure control was difficult with LPI alone, so micropulse transscleral cyclophotocoagulation was performed 9).
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Gedde SJ, Chen PP, Muir KW, Vinod K, Lind JT, Wright MM, et al. Primary Angle-Closure Disease Preferred Practice Pattern®. Ophthalmology. 2021;128(1):P30-P70. doi:10.1016/j.ophtha.2020.10.021. PMID:34933744.
Lu Z, Wang L, Ying X, et al. Bilateral angle closure glaucoma with retinitis pigmentosa in young patients: case series. BMC Ophthalmology. 2023;23:458. doi:10.1186/s12886-023-03190-y.
Alzendi NA, Badawi AH, Alhazzaa B, Alshahrani A, Owaidhah O. Topiramate-induced angle closure glaucoma: Two unique case reports. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2020;34(3):202-204. doi:10.4103/SJOPT.SJOPT_9_20. PMID:34085015; PMCID:PMC8081079.
Tyagi M, Behera S, Senthil S, Pappuru RR, Ambiya V, Dikshit S. Topiramate induced bilateral hypopyonuveitis and choroidal detachment: a report of two cases and review of literature. BMC ophthalmology. 2021;21(1):287. doi:10.1186/s12886-021-02050-x. PMID:34315425; PMCID:PMC8314555.
AlNaqeeb O, Aljohani S, Alshehri A. Topiramate-induced acute bilateral angle closure glaucoma confirmed by ultrasound biomicroscopy. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2020;34(4):316-318. doi:10.4103/1319-4534.322600. PMID:34527882; PMCID:PMC8409355.
Raja V, Manthravadi SK, Anjanamurthy R. Angle-closure glaucoma associated with autosomal recessive bestrophinopathy. Indian journal of ophthalmology. 2022;70(7):2657-2658. doi:10.4103/ijo.IJO_2411_21. PMID:35791192; PMCID:PMC9426077.
Kaisari E, Abouzeid H, Magnin L, Boeuf M, Gkaragkani E, Schalenbourg A, et al. Acute Myopic Shift after a Single Dose of Acetazolamide: A Case Report and Review of the Literature. Klinische Monatsblatter fur Augenheilkunde. 2024;241(4):554-558. doi:10.1055/a-2244-6160. PMID:38653306; PMCID:PMC11038821.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.