Serpiginous choroiditis (SC) is a bilateral, chronic progressive, recurrent inflammatory disease of unknown cause that affects the retinal pigment epithelium (RPE), choriocapillaris, and choroid1). It is also called geographic choroiditis or helicoid choroiditis. It is classified as a type of white dot syndrome 4).
It is a rare disease accounting for 1.6–5.3% of posterior uveitis in non-tuberculosis-endemic areas 2). According to the Guidelines for the Management of Uveitis (Jpn J Ophthalmol 2019;123(6):635-696), clinical statistics from the Japanese Society for Ocular Inflammation show that it accounts for 0.3% of all uveitis cases7). Onset occurs in the 30s to 50s, with a slight male predominance 4). No clear association with systemic diseases has been confirmed, but cases complicated by autoimmune diseases such as systemic lupus erythematosus, immune thrombocytopenic purpura, and antiphospholipid antibody syndrome have been reported 3).
The main site of the lesion is the choriocapillaris; occlusive vasculitis of the choriocapillaris and secondary endothelial cell damage lead to atrophy of the RPE, outer retina, and choroid2). Central vision is impaired in 20–50% of cases, and the frequency increases with longer follow-up 2). In up to 25% of eyes, final visual acuity is less than 20/200.
QDoes serpiginous choroiditis occur only in one eye?
A
It is often bilateral but progresses asymmetrically. Typically, lesions at different stages of healing are observed in both eyes 1). Unilateral onset has also been rarely reported.
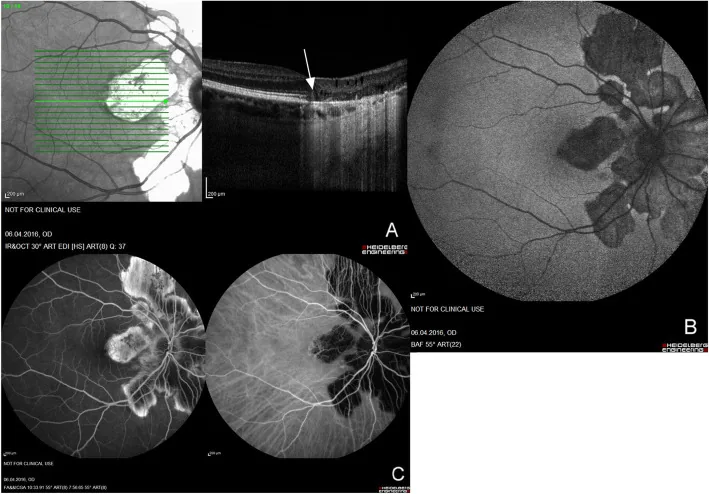
Macedo S, et al. Optical coherence tomography angiography (OCTA) findings in Serpiginous Choroiditis. BMC Ophthalmol. 2020. Figure 1. PMCID: PMC7325353. License: CC BY.
Fundus autofluorescence, fluorescein angiography, and OCT show serpentine chorioretinal lesions extending centrifugally from the optic disc. Representative clinical and imaging findings of serpiginous choroiditis are shown.
The typical fundus finding of serpiginous choroiditis is a gray-yellow chorioretinal lesion that spreads centrifugally in a serpentine pattern from the peripapillary area. 80% of cases present with the peripapillary type 1).
Active Phase
Gray-yellow subretinal lesions: Ill-defined lesions appearing around the optic disc or in the macula.
Active leading edge: An active area showing serpentine progression at the margin of the lesion.
Anterior chamber inflammation: May be accompanied by mild anterior chamber cells 1). Vitritis and vasculitis are usually mild or absent.
Scar Phase
Chorioretinal atrophic patch: Atrophy of the RPE and choriocapillaris allows visualization of the large choroidal vessels. Pigmentation may be present.
Recurrent lesions: New active lesions appear at the margins of existing atrophic patches or in distant areas.
Serpiginous progression: Repeated recurrences lead to irregular atrophic and pigmented lesions spreading in the posterior pole. Lesions may extend beyond the vascular arcades to the equator.
Subtypes of serpiginous choroiditis include macular serpiginous choroiditis and ampiginous choroiditis. The macular type spares the peripapillary area, originates from the macula, has a high risk of choroidal neovascularization, and carries a poor visual prognosis 2). Ampiginous choroiditis shares features of both acute posterior multifocal placoid pigment epitheliopathy (APMPPE) and serpiginous choroiditis, presenting with multiple placoid lesions scattered in the posterior pole 4). The uveitis treatment guidelines describe the abrupt appearance of large (one to several times the optic disc diameter) yellowish-white exudative lesions near the optic disc7).
The interval between recurrences ranges from 3 months to 4 years 2). Active lesions resolve within a few weeks, but signs of activity may persist for 1 to 9 months 2).
The exact etiology of serpiginous choroiditis is unknown, but an immunogenic mechanism is strongly suspected 1). This hypothesis is supported by its response to corticosteroids and immunosuppressive agents, as well as reported associations with HLA-B7 and HLA-A2 3).
Proposed etiologies and associated factors are as follows:
Autoimmune theory: An association with retinal S-antigen has been suggested. Associations with genetic predispositions such as HLA-B7, HLA-A2, HLA-B8, and HLA-Dw3 have been reported, but a consistent correlation has not been established 3).
Infectious triggers: Infections such as Mycobacterium tuberculosis, Treponema pallidum, and herpes viruses have been reported as possible immunological triggers 1)7). Some cases develop following viral prodromal symptoms.
Onset after COVID-19 infection: New-onset macular SC following SARS-CoV-2 infection has been reported 1). It has been suggested that post-infection elevation of inflammatory cytokines may induce autoimmune/autoinflammatory dysregulation.
Association with gastrointestinal diseases: Cases have been reported in the setting of ulcerative colitis and Clostridium difficile infection 3). It has been suggested that gut microbiota dysbiosis may trigger autoimmune reactions.
QIs serpiginous choroiditis hereditary?
A
It is not a clearly hereditary disease. However, associations with genetic predispositions such as HLA-B7 have been reported, and it has been suggested that there may be individual differences in immunological susceptibility 3).
The diagnosis of serpiginous choroiditis is based on characteristic fundus findings and multimodal imaging. Exclusion of infectious diseases is extremely important.
Using a slit-lamp microscope and indirect ophthalmoscope, gray-yellow geographic lesions extending from the peripapillary area and atrophic scars are observed. Anterior chamber cells are mild, and vitreitis is usually minimal 1).
Hyperautofluorescent border and hypoautofluorescent halo
Fluorescein angiography (FA): Active lesions show early hypofluorescence and late hyperfluorescence (leakage). Scarred lesions exhibit hyperfluorescence as window defects.
Indocyanine green angiography (ICGA): Active lesions show hypofluorescence from early to late phases, reflecting choroidal circulatory disturbance1)4).
Fundus autofluorescence (FAF): A minimally invasive test useful for monitoring disease activity. Active lesions show a hypoautofluorescent halo surrounding a hyperautofluorescent border1). Inactive lesions exhibit homogeneous hypoautofluorescence.
Optical coherence tomography (OCT): Active phase shows RPE irregularity, outer layer disruption, and subretinal fluid1)3). Choroidal thickness increases during acute inflammation and thins after resolution1).
Exclusion of tuberculosis is the highest priority. Especially in patients from endemic areas, tuberculosis testing including interferon-gamma release assay (IGRA) and tuberculin skin test is mandatory5).
The following tests are performed to exclude other diseases:
The main diseases that require differentiation from serpiginous choroiditis are as follows.
Tuberculous serpiginous-like choroiditis (SLC): Differentiation is most important because immunosuppressive drugs can worsen tuberculosis. SLC often presents with multiple, scattered lesions that are not adjacent to the optic disc, and even in eyes with macular involvement, there is a tendency to spare the fovea. It is frequently accompanied by vitritis 5).
Multifocal choroiditis (MFC): Characterized by scattered small chorioretinal lesions and vitritis 4).
Toxoplasmosis: Presents with active lesions adjacent to pre-existing scars, accompanied by focal vitritis.
QWhat is the difference from tuberculous serpiginous-like choroiditis?
A
Tuberculous serpiginous-like choroiditis (SLC) presents with multiple, scattered lesions and vitritis, with a tendency to spare the fovea. Serpiginous choroiditis extends continuously from the peripapillary area and has minimal vitritis. In SLC, anti-tuberculosis therapy is essential, and immunosuppressive therapy alone cannot prevent recurrence 5).
There are no randomized controlled trials on the treatment of serpiginous choroiditis, and no established standard therapy exists. Due to the rarity of the disease, treatment is based on case series and expert consensus 2).
Oral corticosteroids or posterior subtenon injection of triamcinolone acetonide (MacuAid) are used. Although there are occasional reports of immunosuppressive drug use overseas, objective assessment of treatment efficacy is difficult due to the relapsing-remitting nature, and they are often ineffective for recurrences.
Calcineurin inhibitors: Cyclosporine A. Triple therapy with azathioprine, cyclosporine, and prednisolone has been reported, but long-term remission maintenance is difficult2).
Alkylating agents: Chlorambucil and cyclophosphamide. Considered the most potent and effective drug group for treating serpiginous choroiditis2).
Biologics: Anti-TNFα agents such as adalimumab and infliximab are used in refractory cases. Efficacy of adalimumab has been reported3)7).
Cases with tuberculosis infection: Anti-tuberculosis treatment (4-drug combination for 2 months + 2-drug combination for 6–12 months) is required7).
In an expert consensus survey, the first-choice immunosuppressants for serpiginous choroiditis were methotrexate (38.0%), mycophenolate mofetil (27.6%), and azathioprine (23.1%), and the most recommended biologic was adalimumab (91.0%)6).
In 17 patients with serpiginous choroiditis treated with chlorambucil, dose adjustment targeting a white blood cell count of 3,000–4,500 cells/μL showed good tolerability and relapse prevention2). Recommended dose is ≤0.2 mg/kg/day, total dose ≤2.2 g.
In a series of 4 cases by Maleki et al., in refractory cases resistant to chlorambucil and systemic steroids, addition of dexamethasone intravitreal implant allowed steroid discontinuation and continuation of chlorambucil, achieving remission for ≥48 months2). The key to success was stabilizing white blood cell count at a toxic level (3,000–4,500 cells/μL).
Choroidal neovascularization (CNV) occurs in up to 35% of cases. Intravitreal injections of anti-VEGF drugs (bevacizumab, ranibizumab) are performed 2). The risk of developing CNV is particularly high in macular-type SC 2).
QCan serpiginous choroiditis be cured?
A
In some patients, long-term remission (“cure”) has been reported with alkylating agents 2). However, it is often a chronic disease with relapses and remissions, requiring long-term immunosuppressive therapy and follow-up.
The core pathology of serpiginous choroiditis is occlusive vasculitis at the level of the choriocapillaris2). Histologically, lymphocytic infiltration is observed in the choroid, and occasionally perivascular lymphocytic aggregates are seen 2)3). Granuloma formation is not observed 3).
The pathophysiological course is understood as follows:
Occlusion of the choriocapillaris: Immune-mediated vasculitis occludes the choriocapillaris, causing local ischemia. This is visualized as areas of reduced blood flow on OCTA1)4).
Damage to the RPE and outer retina: Secondary to choriocapillaris ischemia, degeneration and atrophy of the RPE and outer retina progress 4).
Spread and expansion of inflammation: Lesions extend in a serpentine manner from the edge of active lesions. Recurrences occur at the margins of existing atrophic patches or at distant sites.
Fluctuation in choroidal thickness: Choroidal thickness increases during the acute inflammatory phase and thins after inflammation subsides. In one case, thickness varied from 342 μm at initial visit to 378 μm after 1 month and 233 μm after 4 months 1).
The pathology of serpiginous choroiditis is histologically similar to birdshot chorioretinopathy2). Both diseases are characterized by lymphocytic infiltration of the choroid and are thought to share a common immune-mediated mechanism.
In cases complicated with ulcerative colitis, T-cell-driven inflammation is noted as a common pathological basis 3). It is speculated that autoantibodies from the intestinal mucosa may cross-react with choroidal antigens, and that changes in the gut microbiota may disrupt the balance between regulatory T cells and effector T cells 3).
A case of macular serpiginous choroiditis occurring one month after COVID-19 infection has been reported 1). High-reflective foci in the choroid were observed, thought to be accumulations of activated microglia or damaged RPE cells. It is suggested that SARS-CoV-2 may act as an inflammatory trigger in susceptible hosts, inducing autoimmune dysregulation.
7. Latest Research and Future Perspectives (Research-stage Reports)
Multiple cases of onset or recurrence of serpiginous choroiditis and ampiginous choroiditis after COVID-19 infection have been reported 1).
A case of recurrence of serpiginous choroiditis one month after COVID-19 infection has been reported 1). Additionally, two patients in their 20s developed bilateral ampiginous choroiditis about one week after COVID-19 infection. These findings suggest that SARS-CoV-2 may act as an inflammatory trigger for choroidal inflammation, but a causal relationship has not been proven.
Chlorambucil Combination Regimen for Refractory Cases
Maleki et al. (2021) studied four cases resistant to standard combination therapy with chlorambucil and steroids, and reported that adding dexamethasone intravitreal implant or infliximab and discontinuing steroids stabilized white blood cell control with chlorambucil and achieved long-term remission 2). They proposed the hypothesis that systemic steroids attenuate the effect of chlorambucil, and switching to local steroids may be key to treatment success.
Adalimumab, an anti-TNFα antibody, is being investigated as a steroid-sparing therapy for serpiginous choroiditis.
In a patient with serpiginous choroiditis complicated by ulcerative colitis, introduction of adalimumab resulted in maintenance of remission for both serpiginous choroiditis and ulcerative colitis for 5 months 3). However, there are also reports of disease progression under adalimumab, so its efficacy is not established.
Seddigh S, Pinto A, Zaki AM, Gupta RR. Serpiginous Choroiditis After COVID-19 Infection. Journal of vitreoretinal diseases. 2025;9(2):246-252. doi:10.1177/24741264241297936. PMID:39554631; PMCID:PMC11562243.
Maleki A, Maldonado Cerda A, Garcia CM, et al. Chlorambucil combination therapy in refractory serpiginous choroiditis: a cure? Am J Ophthalmol Case Rep. 2021;21:101014. doi:10.1016/j.ajoc.2021.101014. PMID:33615036; PMCID:PMC7881218.
Pollmann AS, Mishra AV, Betsch DM, Francisconi CLM. Serpiginous Choroiditis Presenting in Association With Clostridium difficile Infection and Ulcerative Colitis. Journal of vitreoretinal diseases. 2021;5(2):177-181. doi:10.1177/2474126420946922. PMID:37009076; PMCID:PMC9979053.
Testi I, Modugno RL, Pavesio C. Multimodal imaging supporting the pathophysiology of white dot syndromes. Journal of ophthalmic inflammation and infection. 2021;11(1):32. doi:10.1186/s12348-021-00261-3. PMID:34529201; PMCID:PMC8446150.
Agrawal R, Gunasekeran DV, Grant R, et al. Consensus on the management of tubercular uveitis: Collaborative Ocular Tuberculosis Study (COTS) group. Ophthalmology. 2021;128:266-276.
Niederer RL, Al-Janabi A, Engelbrecht C, et al. Immunomodulatory therapy prescribing practices for non-infectious uveitis: a survey of international experts. Br J Ophthalmol. 2024;108:482-489.