Idiopathic multifocal choroiditis (IMFC) is a spontaneously occurring inflammatory disease that presents with multiple lesions in the retina and choroid. It involves recurrent episodes of inflammation and can occur bilaterally, either simultaneously or sequentially.
In 1984, Deutsch and Tessler reported 28 cases as “pseudo-POHS.” In 1986, Morgan and Shatz described 11 cases as “recurrent multifocal choroiditis,” noting vitreous inflammation as a feature not seen in POHS patients. IMFC is a distinct disease differentiated from PIC (punctate inner choroidopathy), multifocal choroiditis with panuveitis (MFCwP), and progressive subretinal fibrosis and uveitis syndrome.
Both MFC and PIC are subtypes of white dot syndromes (WDS), a group of inflammatory diseases primarily affecting the outer retina, choriocapillaris, and choroid1). It has been suggested that MFC and PIC may represent a spectrum of the same disease 1).
QHow are POHS and IMFC different?
A
The main difference is the presence or absence of vitritis. POHS does not involve vitritis, whereas IMFC typically shows vitritis in one or both eyes. Additionally, mild anterior chamber inflammation may be present in IMFC.
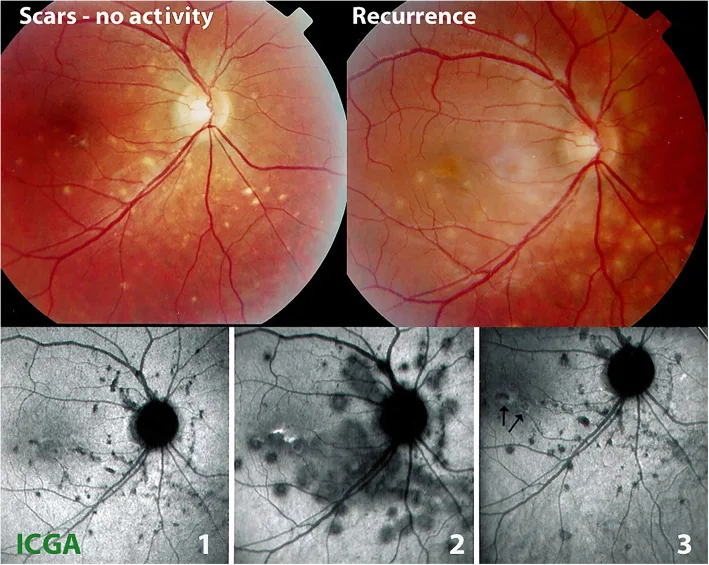
Papasavvas I, et al. Idiopathic multifocal choroiditis (MFC): aggressive and prolonged therapy with multiple immunosuppressive agents is needed to halt the progression of active disease. An offbeat review and a case series. J Ophthalmic Inflamm Infect. 2022. Figure 2. PMCID: PMC8743334. License: CC BY.
Fundus photographs (top row) of multifocal choroiditis (MFC) show yellow punched-out lesions in the quiescent phase on the left and new edematous lesions during recurrence on the right. The ICGA images (bottom row) show the quiescent phase (1), active phase (2), and post-treatment course (3). These correspond to the choroidal atrophic lesions discussed in the section “2. Main Symptoms and Clinical Findings.”
The etiology of IMFC is unknown. There is a hypothesis that a preceding infection stimulates an immune response, but no specific pathogen has been identified.
Epidemiological features:
More common in white women.
Mean age at onset 30 years (range: 6–69 years).
Most patients are myopic.
Affects healthy individuals without known systemic or ocular diseases.
Genetic predisposition:
Idiopathic multifocal choroiditis is associated with haplotypes of IL-10 and tumor necrosis factor (TNF).
Pathophysiological hypothesis:
Inflammatory lesions begin at the level of the retinal pigment epithelium and choriocapillaris. Antigen sensitization may occur in the photoreceptors and retinal pigment epithelium due to exogenous antigens, potentially compromising the integrity of Bruch’s membrane. This creates space for the development of choroidal neovascular membranes, which can occur in up to 60% of patients.
Idiopathic multifocal choroiditis is a clinical diagnosis and a diagnosis of exclusion. It is essential to rule out infectious, malignant, and systemic diseases.
In tuberculosis-endemic regions (e.g., India), up to 40% of multifocal choroiditis may be associated with ocular tuberculosis2), and may be observed as inflammatory lesions beneath the retinal pigment epithelium on optical coherence tomography2).
QHow is idiopathic multifocal choroiditis differentiated from tuberculosis?
A
Multimodal imaging is useful for differentiation. In tuberculous multifocal choroiditis, optical coherence tomography may show disruption of the external limiting membrane and focal loss of the ellipsoid zone overlying inflammatory lesions of the retinal pigment epithelium2). Evaluation combines QuantiFERON-TB Gold testing and imaging.
Treatment is selected based on the degree of inflammation, active lesions, complications, and visual impairment. Indications for treatment include cystoid macular edema, dense vitritis, or choroidal neovascular membrane.
Inflammatory lesions begin at the level of the retinal pigment epithelium and choriocapillaris, and it is hypothesized that antigen sensitization occurs in the retinal pigment epithelium in response to foreign antigens.
Idiopathic multifocal choroiditis and punctate inner choroidopathy both involve the outer retina, choriocapillaris, and choroid, and may represent a spectrum of the same disease 1). Multifocal choroiditis is a chronic, bilateral, recurrent inflammatory disease characterized by posterior lesions with anterior uveitis and vitritis, whereas punctate inner choroidopathy differs in that it does not involve vitritis or anterior segment inflammation 1).
OCT angiography findings show distinct areas of decreased blood flow at the level of the choriocapillaris corresponding to active inflammatory lesions, supporting the possibility that outer retinal changes are secondary to primary choroidal involvement 1).
Inflammation disrupts the integrity of Bruch’s membrane, which serves as a foothold for the development of choroidal neovascular membranes. In idiopathic multifocal choroiditis, choroidal neovascularization can occur in up to 60% of patients.
Genetic factors such as associations with haplotypes of IL-10 and tumor necrosis factor have been reported, but the exact mechanism remains unclear.
7. Latest research and future perspectives (research-stage reports)
OCT angiography shows distinct areas of decreased blood flow in the choriocapillaris of punctate inner choroidopathy and multifocal choroiditis lesions, corresponding to active inflammatory lesions 1). It is also applied to monitor choroidal vascular changes after treatment.
OCT angiography has been shown to delineate areas of decreased choriocapillaris blood flow corresponding to retinal pigment epithelial elevations on optical coherence tomography and hypofluorescent spots on indocyanine green angiography, deepening pathophysiological understanding 1).
Multimodal imaging has led to the concept that multifocal choroiditis with panuveitis and punctate inner choroidopathy are part of the same disease spectrum. More precise classification and development of personalized treatments are progressing. 1)
Testi I, Modugno RL, Pavesio C. Multimodal imaging supporting the pathophysiology of white dot syndromes. Journal of ophthalmic inflammation and infection. 2021;11(1):32. doi:10.1186/s12348-021-00261-3. PMID:34529201; PMCID:PMC8446150.
Kaza H, Gala JM, Rani PK. Subfoveal retinal pigment epithelium inflammatory lesion presenting as a sign of reactivation of tubercular multifocal choroiditis. BMJ case reports. 2021;14(5). doi:10.1136/bcr-2020-240280. PMID:34031072; PMCID:PMC8149327.
Branford JA, et al. Practice patterns of systemic immunomodulatory drug treatment for non-infectious uveitis: an international study. Br J Ophthalmol. 2025;109:482-489.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.