Primary acquired melanosis (PAM) is an acquired conjunctival lesion characterized by patchy black-brown pigmentation due to abnormal proliferation of melanocytes. It can occur anywhere on the conjunctiva. Unlike nevus, it is a flat pigmented lesion without elevation.
In addition to primary acquired melanosis without known cause, pigmentation may also occur due to chronic inflammation such as allergic diseases, irritation from cosmetics or chemicals, or after surgery (secondary melanosis). PAM refers to primary lesions without these secondary causes.
QIs PAM cancer?
A
PAM itself is not necessarily malignant. PAM without atypia is benign with low risk of malignant transformation. On the other hand, PAM with atypia is a precancerous lesion that transforms into conjunctival malignant melanoma in about 25-50% of cases. It is important to confirm the presence of atypia by biopsy.
PAM is broadly classified into two groups based on the presence or absence of histological atypia. Recently, it is also called conjunctival melanocytic intraepithelial lesion (C-MIL) and has been reorganized in the WHO classification 3).
PAM classification
Corresponding C-MIL
Risk of malignant transformation
PAM without atypia
Low-grade C-MIL
Low (rarely transforms)
PAM with atypia, mild
Intermediate-grade C-MIL
Moderate
PAM with atypia, severe
High-grade C-MIL / melanoma in situ
Approximately 25–50%
A C-MIN score of 5 or higher is considered melanoma in situ and requires more aggressive treatment2).
It accounts for 11% of all conjunctival lesions2). It most commonly occurs in middle-aged and older Caucasians and is almost always unilateral. Since approximately 60–75% of conjunctival malignant melanomas arise from PAM, it is particularly important as a precancerous lesion. The incidence is lower in East Asians compared to Caucasians.
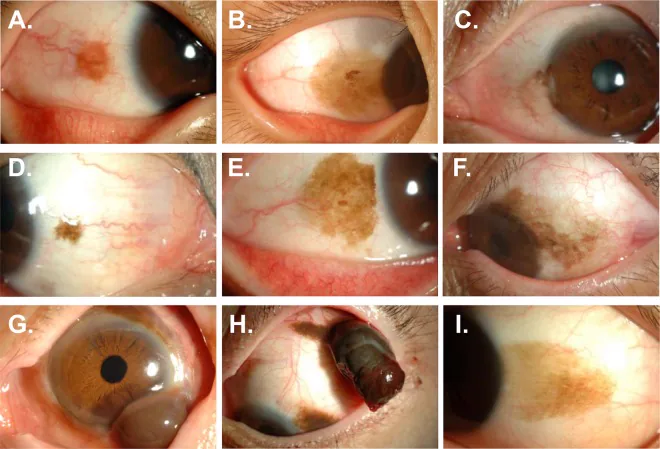
Lee YJ, Lee C, Kim MK, et al. Conjunctival pigmented lesion: Clinicopathological analysis of 85 cases in Korean population. Sci Rep. 2019;9(1):18204. Figure 2. PMID: 31796811; PMCID: PMC6890774; DOI: 10.1038/s41598-019-54786-8. License: CC BY.
Anterior segment photographs of conjunctival pigmented lesions by histological classification. D and E show PAM without atypia (flat, light to dark brown patchy pigmentation), and F shows the clinical appearance of PAM with atypia. These correspond to the morphology and atypia classification of primary acquired melanosis discussed in the section “2. Main symptoms and clinical findings.”
A characteristic course of PAM is the “wax and wane” phenomenon, where pigmentation repeatedly increases and decreases 2). Even if the pigmentation becomes lighter or disappears, the lesion itself has not disappeared. Overlooking this point may lead to the mistaken belief that the condition has healed, resulting in neglect of follow-up.
QDoes lighter pigmentation mean it is cured?
A
No. PAM shows a waxing and waning pattern. Even if the pigmentation becomes lighter, the lesion has not disappeared, and pathological lesions often remain. The same applies after mitomycin C treatment; after pigmentation disappears, mapping biopsy is necessary to confirm eradication.
The direct cause of PAM is not clear, but it is based on abnormal proliferation of melanocytes within the epithelium. Unlike secondary melanosis (described below), it occurs without a specific external cause.
Histological atypia: PAM with atypia is the greatest risk. In particular, high-grade atypia (C-MIN score ≥5) has a high rate of malignant transformation.
Extent of the lesion: More extensive lesions may carry higher risk.
TERT promoter mutation: Detected in moderate to severe atypia of PAM, suggesting features of melanoma in situ 2).
Since the conjunctiva is directly exposed to ultraviolet (UV) light, UV exposure is considered a risk factor. The reason it is more common in Caucasians is that they have less melanin, resulting in a weaker UV filter effect.
First, the morphology, color, borders, and presence of elevation of the lesion are evaluated in detail using a slit-lamp microscope. Eyelid eversion must always be performed to examine the fornix and palpebral conjunctiva.
Since PAM shows “wax and wane,” regular photographic documentation from the initial visit is the basis for follow-up. It objectively tracks changes in pigment distribution.
This is the gold standard for definitive diagnosis of PAM and determining treatment strategy.
QWhat is a map biopsy?
A
A map biopsy is a biopsy technique in which pigmented lesions of the conjunctiva are systematically collected from multiple sites. By mapping the distribution of atypia throughout the lesion, the extent and degree of atypia can be accurately determined. The presence and degree of atypia are the most important factors in deciding the treatment strategy (observation or excision).
PAM without atypia: Minimal melanocyte proliferation in the basal layer of the epithelium
PAM with atypia: Isolated or confluent nests of atypical melanocytes, pagetoid spread, large abnormal cells, prominent nucleoli, high nuclear-to-cytoplasmic ratio, mitotic figures
As an alternative to mitomycin C, topical administration of IFNα-2b is used. Its advantage over MMC is that it does not cause limbal stem cell deficiency.
QIs surgery necessary immediately after a diagnosis of PAM?
A
Not necessarily. For PAM without atypia, regular observation is the basic approach. On the other hand, PAM with atypia is a precancerous lesion, so active treatment such as excision or topical chemotherapy is recommended. The standard procedure is to determine the treatment plan after confirming the presence or absence of atypia by biopsy.
The essence of PAM is abnormal proliferation of melanocytes within the conjunctival epithelium. The stage without invasion into the subepithelial tissue is called “intraepithelial” lesion, and when invasion occurs, it is diagnosed as malignant melanoma.
Malignant transformation from PAM with atypia has been reported to involve TERT promoter mutation (c.-124C>T) 2). This mutation leads to activation of telomerase reverse transcriptase, promoting cell immortalization and malignant transformation. It has also been associated with high tumor mutational burden.
PAM accounts for approximately 60–75% of the origins of conjunctival malignant melanoma. This indicates that if PAM is left untreated or overlooked, it can progress to invasive malignant melanoma, underscoring the importance of early diagnosis and appropriate management.
International standardization of the C-MIL classification system and C-MIN scoring is progressing 3). This is expected to improve diagnostic reproducibility among pathologists and enhance the accuracy of treatment selection based on the degree of atypia.
Non-invasive Assessment Using Immunohistochemistry such as PRAME
Immunohistochemistry panels combining markers such as PRAME, p16, and Ki-67 are enabling reclassification of lesions previously considered “indeterminate” 1). This may allow more accurate determination of the need and timing for biopsy.
Non-invasive monitoring techniques using anterior segment OCT and in vivo confocal microscopy are being developed. They are expected to serve as means to evaluate PAM progression in real time without biopsy.
Eder et al. (2024) showed that in 5 cases of atypical conjunctival melanocytic proliferative lesions that were difficult to evaluate by routine histology, reclassification was possible using a combination of immunohistochemistry panel (PRAME, p16, HMB45, Ki-67, etc.) and FISH analysis 1). The potential of microRNA profiling for differentiating benign from malignant lesions has also been suggested.
Research is advancing on molecular profiling, including TERT promoter mutations, to individually predict the risk of transformation from PAM to melanoma 2). In the future, personalized treatment strategies based on molecular risk assessment are expected to become possible.
Eder A, Milman T, Mudhar HS, et al. Unusual conjunctival melanocytic proliferations: report of five cases and review of the literature. Surv Ophthalmol. 2024; PMC12208716.
Goemaere J, Lauwers N, de Keizer ROB, et al. Bone metastasis in a case of primary acquired melanosis with atypia resulting from conjunctiva melanoma. Am J Ophthalmol Case Rep. 2023;29:101730. doi:10.1016/j.ajoc.2022.101730. PMID:36561878; PMCID:PMC9763362.
Englisch CN, Berger T, Flockerzi F, et al. Conjunctival melanoma with pronounced central corneal invasion: one-year relapse free follow-up. Am J Ophthalmol Case Rep. 2024; PMC11403272.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.