Conjunctival epithelial tumors are a general term for tumors arising from the conjunctival epithelium. They are broadly classified into benign tumors (papilloma, epithelial cyst, etc.), precancerous lesions (conjunctival intraepithelial neoplasia, CIN), and malignant tumors (invasive squamous cell carcinoma, SCC).
Severe conjunctival intraepithelial neoplasia (carcinoma in situ): Abnormal growth extends through the full thickness of the epithelium. The basement membrane is intact
Invasive squamous cell carcinoma: Invades the subconjunctival tissue beyond the basement membrane
The incidence of conjunctival squamous cell carcinoma varies greatly by geographic region. It is reported to range from 0.02 to 3.5 per 100,000 people (depending on latitude and UV exposure)1). 75% of patients are male, 75% are aged 60 years or older, and 75% arise from the corneal limbus1).
In a study of 771 non-melanocytic conjunctival tumors by Shields et al., ocular surface squamous neoplasia accounted for 23% (179 cases), making it the most common non-pigmented tumor1). The worldwide age-standardized incidence rate of ocular surface squamous neoplasia is 0.26 per 100,000 per year, with the highest rate in Africa (3.4 per 100,000 per year)1).
The classification of conjunctival epithelial tumors is shown below.
QHow often do conjunctival epithelial tumors occur?
A
The incidence of squamous cell carcinoma varies greatly by region, ranging from 0.02 to 3.5 per 100,000 people1). The age-standardized rate of ocular surface squamous neoplasia worldwide is 0.26 per 100,000 per year, but in Africa it is as high as 3.4 per 100,000 per year1).
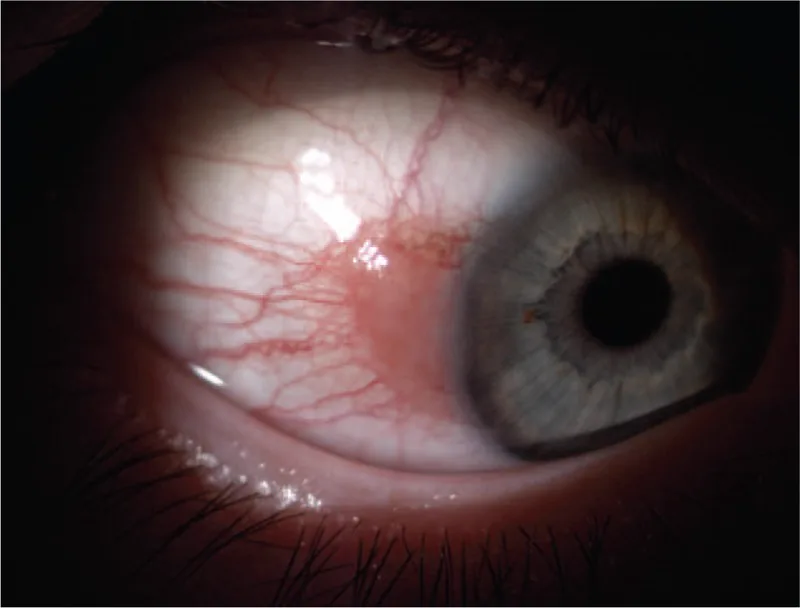
Bolek B, et al. Treatment of conjunctival papilloma with topical interferon alpha-2b - case report. Medicine (Baltimore). 2020. Figure 1. PMCID: PMC7035065. License: CC BY.
A broad-based, pink papillomatous lesion of the limbal conjunctiva before treatment. This corresponds to conjunctival papilloma discussed in the section “2. Main symptoms and clinical findings”.
Redness and foreign body sensation: Most common complaint
Decreased vision: Occurs when the lesion involves the pupillary area
Asymptomatic: May be discovered incidentally
Redness and ocular discomfort: Symptoms of conjunctival squamous cell carcinoma are nonspecific, with visual impairment when the visual axis is involved1)
Conjunctival intraepithelial neoplasia is observed as a sessile, slightly opaque, flat elevated lesion. It appears white to pale red, with characteristic abnormal vascular patterns described as “firework-like”.
Invasive squamous cell carcinoma takes various forms.
Cauliflower-like papillomatous lesion or white elevated lesion with an irregular surface
May be accompanied by leukoplakia on the surface due to hyperkeratosis
Pale red to reddish-pink, gelatinous, irregular appearance
Keratin may adhere to the surface
The morphological variations of the lesion and their clinical significance are shown below.
Gelatinous: The most common form
Leukoplakic: Reflects hyperkeratosis
Papillary/nodular: Associated with a more aggressive pathological grade1)
Nodular ulcerative type: Rare but a strong indicator of invasive tumor1)
Abnormally tortuous and dilated feeding vessels on the tumor: An important finding suggesting malignant growth1)
Elevated lesions tend to have higher malignancy than flat lesions1). Common sites are the interpalpebral fissure and limbus, while the palpebral conjunctiva is less frequently involved1).
Clinical features of benign tumors are as follows:
Childhood papilloma: Granular red appearance, pedunculated or sessile, commonly located in the inferior fornix and bulbar conjunctiva. Associated with human papillomavirus (HPV) types 6 and 11
Adult papilloma: Pale pink, unilateral and solitary, commonly located at the limbus, bulbar conjunctiva, and caruncle. HPV-associated
Ultraviolet exposure: The greatest risk factor. Carcinogenesis mechanism via p53 gene mutation 1)
Human papillomavirus: Types 16 and 18 are implicated 1). Papillomas are associated with HPV types 6/11. However, the association between HPV and ocular surface squamous neoplasia varies by region and is debated 1)
Male sex and older age: Mean age of onset 56 years 1)
Immunodeficiency: High incidence in HIV/AIDS patients. Related to high prevalence in young African women.
Others: Smoking, chemical exposure (petroleum products, beryllium, arsenic, etc.), vitamin A deficiency, ocular surface trauma 1)
Recurrence risk factors: Large tumor size, positive surgical margins, HIV infection, high tumor grade, presence of feeder vessels, high proliferation index 1)
QWhat are the risk factors besides UV?
A
HPV types 16/18, immunodeficiency (HIV/AIDS), xeroderma pigmentosum, smoking, chemical exposure (petroleum products, beryllium, arsenic, etc.), and vitamin A deficiency are listed 1). HIV infection and positive surgical margins are strongly associated with tumor recurrence 1).
Slit-lamp microscopy: Observe the size, borders, color, and surface irregularity of the tumor. Photographic documentation is recommended.
Fluorescein staining: Utilizes increased permeability of abnormal epithelium to clearly delineate the border between lesion and healthy tissue. Useful for preventing oversight of flat or small lesions. Also helps detect flat tumor areas surrounding elevated lesions.
Scleral scattering: Clarifies the extent of flat lesions on the cornea.
Special stains: Rose bengal, lissamine green, and methylene blue are also used to stain necrotic squamous epithelial cells1).
High-resolution optical coherence tomography (HR-OCT): A non-invasive tool. Characterized by a sharp transition between highly reflective thickened epithelium and normal epithelium. Epithelial thickness >140 μm is considered a potential indicator of tumor. Useful for differentiating invasive from non-invasive types1).
In vivo confocal microscopy: Useful for differentiating epithelial from subepithelial lesions1).
Impression cytology and exfoliative cytology: Minimally invasive but limited in assessing depth of invasion1).
Metastasis workup: Palpation of preauricular lymph nodes is basic. For extensive tumors, whole-body evaluation with gallium scintigraphy or FDG-PET is performed.
Clinical differentiation between conjunctival intraepithelial neoplasia and invasive squamous cell carcinoma is difficult, and histopathological examination is always required for definitive diagnosis1).
Excisional biopsy: For limbal tumors less than 4 clock hours or less than 15 mm in basal diameter.
Incisional biopsy: For larger tumors as initial evaluation before extensive surgery.
Histopathological diagnosis is based on 10–20% formalin fixation, paraffin embedding, and HE staining.
QCan conjunctival intraepithelial neoplasia and invasive squamous cell carcinoma be distinguished clinically?
A
Clinical differentiation between conjunctival intraepithelial neoplasia and squamous cell carcinoma is difficult, and histopathological examination is essential for definitive diagnosis. High-resolution optical coherence tomography is useful for distinguishing invasive from non-invasive types1), but the final diagnosis is based on histological examination.
Resect with a safety margin of 2–3 mm from the tumor edge
For cases with unclear margins, confirm negative margins by intraoperative frozen section diagnosis
The tumor can often be peeled from the cornea and sclera with a spatula
To prevent recurrence, apply 0.04% mitomycin C to the resection site or combine with cryocoagulation of the resection margins
When resecting more than half the circumference of the limbus, perform corneal epithelial transplantation (corneal epithelialization/limbal transplantation)
Topical chemotherapy is used as primary or adjuvant therapy. A cycle of “1 week on, 1 week off” is typical.
In Japan, there are reports of tumor cure with low-dose mitomycin C or 5-fluorouracil eye drops. However, some reports indicate that it is only effective for intraepithelial lesions, and long-term recurrence rates and complications have not been fully elucidated.
Interferon alpha-2b is used as eye drops or subconjunctival injection. It has lower toxicity and better tolerability compared to mitomycin C and 5-fluorouracil, but is more costly.
Childhood papilloma: Cryocoagulation plus no-touch excision is recommended. Incomplete resection carries a risk of invasive recurrence. Alternatives include interferon alpha, oral cimetidine, and topical chemotherapy with 0.02% mitomycin C.
Adult papilloma: Surgical excision plus cryocoagulation.
Metastasis is rare and the prognosis for life is good. The local recurrence rate of invasive squamous cell carcinoma is reported as 5%, and the regional lymph node metastasis rate as 2% 1). On the other hand, the mortality rate of untreated squamous cell carcinoma is 8–24%, and orbital invasion occurs in about 10% of cases 1).
QAre there treatments other than surgery?
A
Topical chemotherapy such as mitomycin C, 5-fluorouracil, and interferon alpha-2b is used as primary or adjuvant therapy. However, there are reports of efficacy only for intraepithelial lesions 1), and long-term outcomes and complications are not well established. Radiation therapy is used adjuvantly for unresectable cases or those with eyelid invasion.
The conjunctiva consists of three parts: bulbar conjunctiva, fornix, and palpebral conjunctiva. Special areas include the plica semilunaris (remnant of the nictitating membrane) and the caruncle (conjunctival and skin structures).
Epithelium is non-keratinized, 5 layers. Near the limbus it is columnar, and in the fornix it is squamous.
Goblet cells are present in the inner layer and secrete the mucin layer of tears.
The substantia propria consists of a superficial adenoid layer (develops after 3 months of age) and a deep fibrous layer.
Mucosa-associated lymphoid tissue (MALT): lymphocytes and plasma cells between epithelial cells.
Severe conjunctival intraepithelial neoplasia: The full thickness of the epithelium is replaced by abnormal cells lacking maturation. Epithelial cells show loss of polarity and atypia throughout the full thickness.
The basement membrane remains intact: This is a key difference from invasive squamous cell carcinoma.
Invasive Squamous Cell Carcinoma
Basement membrane breach: Malignant squamous epithelial cells proliferate beyond the basement membrane into the stroma1).
Histological features: Thickened cells with atypia and mitotic figures infiltrate the lamina propria.
Mucoepidermoid carcinoma: An aggressive subtype of squamous cell carcinoma. It occurs more often in older individuals and contains yellow cystic components from mucus-secreting cells1).
Histopathology of benign tumors is as follows:
Papilloma: Papillary projections with vascular cores, acanthotic epithelium with little keratinization
Pseudocarcinomatous hyperplasia: Marked acanthosis, hyperkeratosis, and parakeratosis. No cellular atypia.
The application of bevacizumab and ranibizumab to conjunctival lesions has been reported1).
According to a review by Tsatros et al., studies using ranibizumab (1.25–2.5 mg, subconjunctival injection 1–2 times per month) showed complete regression in 34% and partial regression in 66%, with no recurrence during 6 months of follow-up1). Bevacizumab is promising for conjunctival lesions, but its efficacy for corneal lesions is unclear, and a risk of delayed corneal epithelial healing has been noted. Large-scale studies are needed for both.
External beam radiation therapy (EBRT): Irradiation with proton or electron beams. Useful for avoiding enucleation in cases of large tumors or intraocular invasion1)
Postoperative proton therapy: Reported to reduce recurrence of squamous cell carcinoma1)
Brachytherapy: Sr-90, I-125, Ru-106. Good tumor control has been reported even in cases with positive resection margins1)
According to a review by Tsatros et al., a pilot study combining verteporfin and laser reported 100% tumor regression and no recurrence in conjunctival squamous cell carcinoma1). High cost, need for specialized training, and limited availability are challenges for widespread use.
A case report has shown a remarkable effect of the HPV vaccine on HPV type 16-positive conjunctival intraepithelial neoplasia. Large-scale studies are needed for validation.