Conjunctival melanocytic tumors are a collective term for benign and malignant neoplasms arising from melanocytes of the conjunctiva. They are mainly classified into three categories.
Nevus: A congenital benign tumor. It is the most common conjunctival melanocytic tumor, with an overall risk of malignant transformation of about 1%.
Primary acquired melanosis: An acquired pigmented lesion that develops after middle age. It is divided into those without atypia (benign) and those with atypia (precancerous). Recently, it is also called conjunctival melanocytic intraepithelial lesion (C-MIL)4), and a C-MIN score of 5 or higher is considered melanoma in situ8).
Conjunctival melanoma (malignant melanoma): A malignant tumor accounting for approximately 2% of all ocular tumors and 5–7% of all ocular melanomas 1, 4, 5, 6).
The global incidence of conjunctival melanoma is approximately 0.3–0.8 per million per year, with the highest rates in Northern Europe and North America. Incidence has been increasing over the past 50 years. An estimated 130 new cases occur annually in the United States and about 320 in Europe. The age-adjusted incidence in Asians is low at 0.15 per million per year 2), with the highest occurrence in Whites (91.2%) and only 2.4% in Afro-Caribbean populations.
The mean age at onset is 55–65 years, and cases under 20 years of age are extremely rare 5). Pediatric cases account for only 1% of all conjunctival melanomas 9). Primary acquired melanosis accounts for 11% of all conjunctival lesions 8) and is the most common origin of melanoma (approximately 60–75%).
Conjunctival melanoma is the only mucosal melanoma for which an association with ultraviolet exposure has been suggested, because the bulbar conjunctiva is directly exposed to UV radiation 6). The fact that melanin filters UVB radiation by about twofold is thought to explain the lower incidence in people of color.
QHow common are conjunctival melanocytic tumors?
A
The incidence of conjunctival melanoma is 0.3–0.8 per million per year, making it a relatively rare disease, but it has been increasing over the past 50 years. On the other hand, nevi are the most common conjunctival melanocytic tumors and are almost always benign.
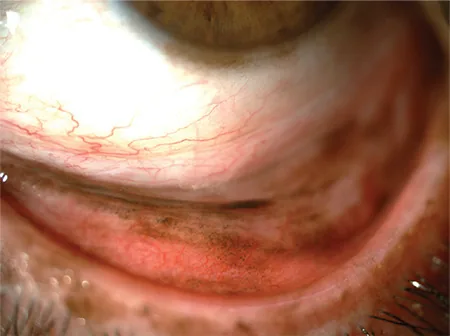
Koç İ, et al. Current Management of Conjunctival Melanoma Part 1: Clinical Features, Diagnosis and Histopathology. Turk J Ophthalmol. 2020. Figure 2. PMCID: PMC7610047. License: CC BY.
When the lower eyelid is everted, diffuse PAM is observed especially in the tarsal conjunctiva, and pigmentation of the corneal limbus is also visible. This corresponds to primary acquired melanosis discussed in the section “2. Main symptoms and clinical findings.”
Location: Most commonly on the bulbar conjunctiva near the limbus in the interpalpebral fissure.
Cysts: Usually accompanied by conjunctival inclusion cysts (detectable by slit lamp, ultrasound, or anterior segment optical coherence tomography). The presence of cysts is an important finding suggestive of benignity.
Course: Long-standing (congenital). May change in color and size during puberty due to hormonal changes. Rapid changes in adulthood raise suspicion of malignancy.
Corneal invasion: Rare.
Primary Acquired Melanosis
Patient background: Middle-aged to elderly, predominantly Caucasian, almost always unilateral.
Appearance: Flat pigmented lesion ranging from light brown to dark brown. May exhibit various shades of color.
Distribution: Can occur in any part of the conjunctiva. Continuous or discontinuous. May be hidden in the fornix or palpebral conjunctiva, so eyelid eversion is important for evaluation.
Course: May show wax and wane. Loss of pigmentation does not indicate regression of primary acquired melanosis8).
Conjunctival Melanoma
Predilection site: About 90% occur on the bulbar conjunctiva, with 63% localized in the temporal quadrant 4, 6).
Appearance: Pigmented (70%) or non-pigmented (30%) 5). Non-pigmented lesions are pink to red masses and may be misdiagnosed as squamous cell carcinoma.
Characteristic findings: Nodular or flat. Often accompanied by feeder vessels. Adhesion to the sclera. The average distance from the tumor to the corneal limbus is 2 mm, and 61% reach the limbus4).
QAre all pigmented conjunctival lesions malignant?
A
No. Among pigmented conjunctival lesions, benign nevi are the most common, and the overall risk of malignant transformation is only about 1%. The location of the lesion, presence of cysts, time of onset, and pattern of change are important for differentiating benign from malignant, and if suspicious changes occur, consultation with a specialist is recommended.
Lymphatic spread is the main route of metastasis. Temporal conjunctival lesions tend to metastasize to the preauricular lymph nodes, while nasal conjunctival lesions tend to metastasize to the submandibular lymph nodes. Distant metastases (hematogenous) occur in the brain, lungs, liver, skin, adrenal glands, heart, peritoneum, pancreas, intestines, kidneys, bones, spleen, etc.6, 1) Lymph node metastases are found in 15–41% of cases at a mean of 2.3 years after diagnosis, and systemic metastases occur in 9–25% at 3 years. Even when lymph node metastases are not detected, distant hematogenous organ metastases occur in 38% of cases8).
QWhat is the most important factor determining the prognosis of conjunctival melanoma?
A
Major poor prognostic factors include tumor thickness (especially >2 mm), lesion location (caruncle has the worst prognosis), AJCC stage, nodular morphology, lymphatic invasion, and orbital invasion. Completeness of resection also greatly affects prognosis; approximately 49.3% of cases with incomplete resection recur.
Immunohistochemistry is essential for definitive diagnosis and differentiation between benign and malignant lesions. The WHO 5th edition has adopted immunohistochemistry of melanocytic markers as the preferred diagnostic criterion8).
There are lesions that cannot be clearly classified as benign or malignant7).
Deep penetrating nevus (DPN): Activation of WNT/β-catenin pathway, BRAF V600E mutation positive in all cases, NRAS mutation negative, PRAME negative, low Ki-67. Female:male = 1.3:1, mean age 25 years. No reports of recurrence or metastasis after excision.
Nevoid melanoma: Morphologically resembles a nevus but exhibits malignant behavior. Shows loss of p16, PRAME positivity, high Ki-67. Associated with BAP1 inactivation. Management follows melanoma guidelines.
Usually only observation with photographic documentation. If enlargement or color change occurs, consider excision. However, changes during puberty are often due to hormonal changes, inflammation, or cyst enlargement; rapid changes in adulthood are indicators of malignancy.
Biopsy: Carefully perform incisional/excisional/map biopsy for suspicious lesions
Surgery: Add cryotherapy to the excision margins depending on the clinically suspicious area
Topical chemotherapy: Consider topical administration of mitomycin C or interferon alpha-2b for histologically proven primary acquired melanosis with atypia
Mitomycin C 0.02%: Multiple sessions of 5 times/day for 1 week8)
Only intraepithelial lesions are eligible (inappropriate for invasive melanoma)
Follow-up management note: Even if pigmentation disappears due to the “wax and wane” of primary acquired melanosis, the lesion may not have resolved. After mitomycin C treatment, mapping biopsy should confirm eradication of primary acquired melanosis8).
Orbital exenteration: Indicated for extensive/recurrent cases. For reconstruction after resection, free radial forearm flap, temporoparietal fascial flap, anterolateral thigh flap, etc. are used2).
Enucleation: Indicated for cases with intraocular extension.
QWhat is the "no-touch technique" in conjunctival melanoma surgery?
A
To prevent tumor cell seeding (local recurrence or metastasis due to seeding), this technique involves resecting the tumor without directly touching it with instruments during surgery, and in a dry environment without using irrigation fluid (BSS). By ensuring a 3–5 mm safety margin and resecting the entire tumor en bloc, the risk of recurrence due to incomplete resection is reduced.
Conjunctival melanoma is genetically similar to cutaneous melanoma rather than uveal melanoma. The major UV-related driver mutations are BRAF, NF1, and RAS. Markers of uveal melanoma (BAP1, GNAQ, GNA11, SF3B1) have been confirmed to be negative in conjunctival melanoma1).
The TERT c.-124C>T mutation affects telomerase reverse transcriptase and has been reported to be associated with metastatic conjunctival melanoma1, 8, 6). It is also detected in moderate to severe atypia of primary acquired melanosis, suggesting a nature of melanoma in situ8). It has also been shown to be associated with high tumor mutational burden6).
Chou et al. (2023) analyzed the molecular profile of a T3c conjunctival melanoma case in a 94-year-old male. They identified NF1 mutations (c.4339C>T, VAF 31.5%; c.5606T>A, VAF 32.0%) and a TERT promoter mutation (c.-124C>T, VAF 31.4%), while BRAF, NRAS, and cKIT were all negative. The combination of NF1 mutation and NRAS negativity is considered a contributing factor to the relatively favorable course without metastasis1).
High PD-L1 expression and the presence of a transcriptional subtype rich in immune-related genes have been confirmed, providing a rationale for the use of immune checkpoint inhibitors. Data on BRAF inhibitors, MEK inhibitors, and PD-L1 inhibitors are promising but currently limited.
7. Latest research and future perspectives (research-stage reports)
PD-1 inhibitors (pembrolizumab, nivolumab) are being tested for metastatic conjunctival melanoma5). Reports of neoadjuvant (preoperative) immune checkpoint inhibitors also exist 4).
In a case of bone metastasis from primary acquired melanosis reported by Goemaere et al. (2023), nivolumab and spinal radiation therapy were administered, followed by paclitaxel + carboplatin, and eventually transitioned to palliative care 8). A standard systemic therapy regimen for metastatic conjunctival melanoma has not yet been established.
The use of BRAF inhibitors for BRAF mutation-positive cases is being attempted. The possibility of synergistic effects by simultaneously targeting the MAPK and AKT pathways is also under investigation 5).
The use of immunohistochemical panels (PRAME, p16, HMB45, Ki-67, beta-catenin, Cyclin D1) is enabling reclassification of lesions previously considered “indeterminate” 7).
Eder et al. (2024) confirmed BRAF V600E positivity in all 34 DPN cases and NRAS Q61R negativity in all cases by FISH analysis. Additionally, the potential of microRNA profiling for differentiating benign from malignant lesions has been suggested 7, 8). FISH analysis evaluates RREB1 (6p25), CCND1 (11q13), MYB (6q23), and MYC (8q24).
Vishnevskia-Dai et al. (2023) reported a case of amelanotic de novo melanoma (8 mm × 2.5 mm) arising from the nasal bulbar conjunctiva in a 7-year-old boy. No-touch technique with 4 mm margins, cryocoagulation, and amniotic membrane transplantation were performed, resulting in a recurrence-free period of 73 months 9). In pediatric cases, histological differentiation from Spitz nevus is particularly important.
Long-term outcomes of amniotic membrane transplantation
QCan immunotherapy be used for conjunctival melanoma?
A
Based on genetic similarities with cutaneous melanoma (BRAF, NF1, NRAS mutations, high PD-L1 expression), PD-1 inhibitors (pembrolizumab, nivolumab, etc.) and BRAF inhibitors are being attempted in metastatic cases. However, large-scale clinical trials have not been conducted, and evidence is currently limited; a standard regimen has not been established.
Chou LT, Lozeau DF, Boyle NS. A rare case of a long-standing, extensive and invasive conjunctival melanoma without systemic metastasis. Am J Ophthalmol Case Rep. 2023; PMC10121375.
Tan JA, Khoo ET, Al-Chalabi MMM, Mohd Zainal H, Wan Sulaiman WA. Orbital Exenteration and Reconstruction Using a Free Radial Forearm Flap in Conjunctival Melanoma: Old but Gold. Cureus. 2023;15(7):e42572. doi:10.7759/cureus.42572. PMID:37637587. PMCID:PMC10460132.
Montazer F, Heshmati SM, Asgari S, et al. Conjunctival melanoma: a case presentation. Iran J Pathol. 2023; PMC10646746.
Englisch CN, Berger T, Flockerzi F, et al. Conjunctival melanoma with pronounced central corneal invasion: one-year relapse free follow-up. Am J Ophthalmol Case Rep. 2024; PMC11403272.
Menna F, Tschopp M, Meyer P, et al. A case of conjunctival melanoma presenting as a squamous cell carcinoma. Case Rep Ophthalmol. 2024; PMC11509494.
Okongwu CC, Adewara BA, Olaofe OO, Soremekun AI, Ayodele SO, Abdullahi YO, et al. Malignant melanoma of the conjunctiva metastasizing to the submandibular gland: a case report and review of the literature. BMC Ophthalmol. 2025;25(1):130. doi:10.1186/s12886-025-03949-5. PMID:40082862. PMCID:PMC11905526.
Eder A, Milman T, Mudhar HS, et al. Unusual conjunctival melanocytic proliferations: report of five cases and review of the literature. Surv Ophthalmol. 2024; PMC12208716.
Goemaere J, Lauwers N, de Keizer ROB, et al. Bone metastasis in a case of primary acquired melanosis with atypia resulting from conjunctiva melanoma. Am J Ophthalmol Case Rep. 2023;29:101730. doi:10.1016/j.ajoc.2022.101730. PMID:36561878; PMCID:PMC9763362.
Vishnevskia-Dai V, Davidy T, Zloto O. Amelanotic conjunctival melanoma in a child. Am J Ophthalmol Case Rep. 2023; PMC9792290.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.