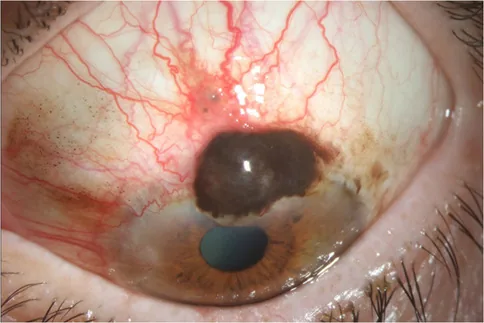
Basal Cell Carcinoma
Location/Morphology: Predilection for lower eyelid, nodular or ulcerative type.
Color: Often accompanied by melanin pigmentation.
Metastasis: Low-grade malignancy that does not metastasize distantly.

Sentinel lymph node biopsy is a procedure to confirm the presence of malignant cells in draining lymph nodes and identify potential systemic micrometastases.
The concept of sentinel lymph node biopsy has evolved in stages.
All malignant tumors of the ocular adnexa except basal cell carcinoma have a tendency to metastasize to regional lymph nodes. The frequency of regional lymph node metastasis by tumor type is as follows:
A large Indian study (536 cases) reported a tumor composition significantly different from Western countries: sebaceous carcinoma 53%, basal cell carcinoma 24%, squamous cell carcinoma 18%. Sebaceous carcinoma had a recurrence rate of 21%, regional lymph node metastasis 16%, systemic metastasis 13%, and metastasis-related death 9% 2).
A positive sentinel lymph node indicates micrometastatic disease, influences AJCC TNM staging, and directly affects prognosis and treatment strategy. The status of the sentinel lymph node is considered the most important prognostic factor for survival and recurrence in patients with cutaneous melanoma.
Basal cell carcinoma is a low-grade tumor that rarely metastasizes distantly, and the likelihood of lymphatic spread is extremely low. Therefore, performing sentinel lymph node biopsy is considered to provide no clinical benefit.
Characteristic clinical findings by tumor type are shown below.
Basal Cell Carcinoma
Location/Morphology: Predilection for lower eyelid, nodular or ulcerative type.
Color: Often accompanied by melanin pigmentation.
Metastasis: Low-grade malignancy that does not metastasize distantly.
Sebaceous Carcinoma
Location: Predilection for upper eyelid. Originates from Meibomian glands, Zeis glands, or sebaceous glands of the caruncle.
Morphology: Yellowish nodular tumor.
Features: May exhibit pagetoid spread (sheet-like proliferation of tumor cells within the conjunctival epithelium of the eyelid and eyeball).
Squamous cell carcinoma
Location: Commonly occurs on the conjunctival surface.
Morphology: Flat reddish tumor with fireworks-like tumor vessels, whitish due to keratinization.
Merkel cell carcinoma
Morphology: Dome-shaped red nodule on the eyelid skin, with dilated tumor vessels and smooth surface.
Features: Rapid growth and high tendency for metastasis.
Positive sentinel lymph node indicates micrometastasis, often without clinically evident enlarged lymph nodes. Conjunctival melanoma is highly invasive and may have micrometastasis at diagnosis.
Lymphatic metastasis of ocular adnexal tumors: All malignant ocular adnexal tumors except basal cell carcinoma have a tendency for lymph node metastasis.
Risk factors for sentinel lymph node biopsy indication by tumor type are shown below.
| Tumor type | Indication criteria/risk factors for sentinel lymph node biopsy |
|---|---|
| Conjunctival/eyelid melanoma | Thickness ≥1 mm, or histological ulceration |
| Cutaneous melanoma | Thickness ≥1 mm, or ulceration/mitotic figures >1/mm², Clark level IV or higher |
| Sebaceous carcinoma | Width ≥10 mm (T2b or higher); size >15 mm increases metastasis risk |
| Squamous cell carcinoma | Width >20 mm, local recurrence, perineural invasion |
| Merkel cell carcinoma | Any size carries risk of metastasis |
| Basal cell carcinoma | Not indicated due to low metastatic potential |
Tumor size exceeding 15 mm is associated with an increased risk of regional lymph node metastasis. A width of ≥10 mm (stage T2b or higher) is considered an indication for SLNB.
Before performing sentinel lymph node biopsy, imaging studies such as ultrasound or CT must be negative. Patients with confirmed disseminated disease are not candidates for sentinel lymph node biopsy.
The excised sentinel lymph node is sectioned into 1–2 mm slices using the bread-loaf method.
Immunohistochemistry markers used by tumor type are shown below.
| Tumor type | Immunohistochemistry markers |
|---|---|
| Melanoma | S100, HMB45, etc. |
| Sebaceous carcinoma | Adipophilin, etc. |
| Squamous cell carcinoma | Pan-cytokeratin, etc. |
| Merkel cell carcinoma | Cytokeratin 20, etc. |
In preoperative evaluation of sebaceous carcinoma, it is necessary to check for metastatic lesions in advance using head and neck CT or MRI.
The American Academy of Ophthalmology Consensus Paper (2020) reported a false-negative rate of 4.6% based on a review of 27 studies. The false-negative rate is inversely correlated with the surgeon’s experience and is showing an improving trend. One institution has reported a false-negative rate of zero over the past 15 years.
The indications for sentinel lymph node biopsy vary depending on tumor type and stage (see “Causes and Risk Factors” for details).
For pagetoid spread (tumor extension into the conjunctival epithelium), topical antineoplastic eye drops are used. All are off-label uses.
If a positive sentinel lymph node is confirmed, a more extensive lymph node dissection (radical lymphadenectomy) is performed. Additionally, adjuvant therapy (radiotherapy, chemotherapy, immunotherapy, etc.) is considered. The specific treatment plan depends on the tumor type and stage.
Certain malignant tumors preferentially and sequentially metastasize via the lymphatic system before hematogenous spread. The sentinel lymph node is the first lymph node to receive lymphatic drainage from the primary tumor, reflecting the earliest presence of metastasis.
Periocular lymphatic drainage varies by region and shows significant individual differences.
In a retrospective study of 536 cases in India by Kaliki et al. (2019), sebaceous carcinoma had a 5-year estimated regional lymph node metastasis rate of 42.55%, a 5-year systemic metastasis rate of 35.74%, and a 5-year metastasis-related mortality rate of 24.88%. Compared with basal cell carcinoma and squamous cell carcinoma, sebaceous carcinoma had significantly higher rates of local invasion (13%), regional lymph node metastasis (16%), and systemic metastasis (13%) 2).
In a review article on conjunctival malignant melanoma by Mirzayev et al. (2024), distant metastasis to the liver, lungs, and brain was reported in 11–42% of cases. Sentinel lymph node biopsy is considered particularly useful for tumors with thickness >2 mm and diameter >10 mm 1).
In the largest study by Esmaeli et al. (2017), 51 patients with ocular adnexal melanoma were evaluated. The sentinel lymph node biopsy positivity rate was 20%, with eyelid margin/eyelid skin melanoma (30%) higher than conjunctival tumors (13%). Three false-negative cases were reported.
In the American Academy of Ophthalmology consensus paper (2020), a review of 27 studies reported a mean sentinel lymph node positivity rate of 16.8% and a false-negative rate of 4.6%. The false-negative rate was inversely correlated with surgeon experience, and one institution reported a zero false-negative rate over the past 15 years.
More accurate identification of sentinel lymph nodes using SPECT/CT is being studied. Compared with conventional lymphoscintigraphy, it may allow more precise anatomical localization of sentinel lymph nodes.
As an alternative to technetium-99m, indocyanine green-guided sentinel lymph node biopsy has been investigated in a few studies. Currently, technetium-99m remains the standard tracer.
In a review by Mirzayev et al. (2024), anti-BRAF/anti-MEK/anti-PD-L1 therapy is considered promising for conjunctival melanoma, but the data available at present are limited 1).