Herpes zoster uveitis (HZU) is anterior or posterior uveitis caused by reactivation of varicella-zoster virus (VZV). Anterior uveitis (iridocyclitis) is the main focus, while posterior uveitis (ARN, PORN) is detailed in separate disease entries.
After primary varicella (chickenpox) in childhood, VZV establishes latency in the dorsal root ganglia (spinal dorsal root ganglia and trigeminal ganglion = Gasserian ganglion). Upon reactivation, it causes ocular symptoms along the first division of the trigeminal nerve (ophthalmic nerve). When accompanied by skin lesions, it is called herpes zoster ophthalmicus (HZO); when ocular inflammation occurs without skin lesions, it is called zoster sine herpete.
Age at onset is usually 50 years or older, with no gender difference.
Herpetic iritis (HSV and VZV combined) accounts for 3.6–4.2% of all uveitis cases2).
Immunocompromised individuals (HIV-infected patients or those using immunosuppressants) are more likely to develop the disease even at a younger age. It has been reported that 43% of anterior uveitis cases in HIV-infected patients are caused by VZV1).
QWhat is the difference between herpes zoster uveitis and herpes simplex uveitis?
A
VZV uveitis tends to become more chronic than HSV uveitis and often involves recurrent intraocular pressure elevation during relapses. It is also frequently accompanied by cutaneous herpes zoster rash, and sectoral iris atrophy is more pronounced. A characteristic of HZU is that when severe, it can progress to posterior uveitis such as acute retinal necrosis (ARN) and progressive outer retinal necrosis (PORN).
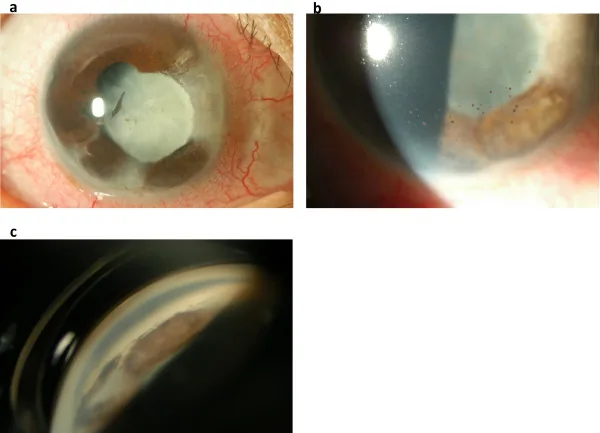
Okunuki Y, et al. A case of herpes zoster uveitis with severe hyphema. BMC Ophthalmol. 2014. Figure 2. PMCID: PMC4046036. License: CC BY.
Anterior segment and gonioscopy images show sectoral iris atrophy, posterior synechiae, pigmented keratic precipitates on the corneal endothelium, and extensive peripheral anterior synechiae in the angle. These are representative inflammatory findings seen in herpes zoster uveitis.
Onset presents with redness, eye pain, and blurred vision. When intraocular pressure elevation is significant, headache and nausea may occur. If posterior lesions are predominant, sudden vision loss and floaters occur.
As a prodromal phase, cutaneous hyperesthesia and tingling sensation of herpes zoster precede the appearance of dermatomal rash along the ophthalmic branch of the trigeminal nerve a few days later.
Mutton-fat KP: Unilateral mutton-fat keratic precipitates and intense anterior chamber inflammation are the main features.
Sectoral or patchy iris atrophy: Secondary to occlusive vasculitis due to chronic uveitis. Caused by partial ischemia from occlusion of blood flow to the iris from the posterior ciliary arteries, observed as transillumination defects on slit-lamp retro-illumination. In the chronic phase, paralytic mydriasis occurs.
High intraocular pressure: Caused by trabeculitis or obstruction of the trabecular meshwork by inflammatory cells. Many patients experience recurrent episodes of elevated intraocular pressure.
Corneal findings: Diverse manifestations including corneal hypoesthesia, pseudodendritic lesions, corneal edema, corneal endotheliitis, and neurotrophic keratitis. May lead to decreased corneal endothelial cell density.
Progressive outer retinal necrosis (PORN): Occurs in immunocompromised individuals. Multifocal deep retinal opacities in the posterior pole and mid-periphery that rapidly enlarge.
Vitritis: Present when the posterior segment is involved.
Hutchinson’s sign:
Presence of herpes zoster rash on the tip of the nose. Important as a predictor of intraocular inflammation. Indicates involvement of the nasociliary branch of the trigeminal nerve.
QCan uveitis occur without skin rash?
A
It can occur. In “zoster sine herpete,” intraocular inflammation occurs without skin rash. Therefore, even without skin symptoms, HZU should be suspected, and tests such as aqueous humor PCR may be necessary.
VZV is a DNA virus with the smallest DNA molecular weight among herpesviruses (approximately 80×10^6). After chickenpox in childhood, it remains latent in the dorsal root ganglia (trigeminal ganglion, Gasserian ganglion) and reactivates with aging or immunosuppression.
Risk factors for reactivation:
Aging (risk increases markedly especially after age 60)
Immunosuppression (HIV infection, use of immunosuppressants, malignant tumors, chemotherapy)
HIV-infected individuals (in patients with CD4 200–349/mm³, herpes zoster is often a major clinical finding 1))
Mental and physical stress
Direct trauma
QIs HIV testing necessary for young patients who develop herpes zoster uveitis?
A
In cases of herpes zoster occurring before age 50, there is a possibility of immunodeficiency such as HIV infection, and active HIV testing is recommended. In HIV-positive patients, 43% of anterior uveitis is reported to be due to VZV 1), and diagnosis and management of the underlying disease are important alongside ophthalmologic treatment.
Clinical diagnosis is often based on the presence or history of HZO. When associated with ophthalmic herpes zoster in the first division of the trigeminal nerve, clinical diagnosis is possible, but in zoster sine herpete without rash, definitive diagnosis requires demonstration of VZV in the aqueous humor by PCR or calculation of antibody ratio 2).
Performed when diagnosis is uncertain or treatment is unresponsive. High sensitivity and specificity.
Goldmann-Witmer coefficient (Q value)
Q<1: No intraocular infection / 1≤Q<6: Suspected intraocular infection / 6≤Q: Intraocular infection present2). Note false negatives within 10 days of onset.
Multiplex PCR (advanced medical care)
Enables comprehensive detection of multiple herpes viruses2).
Serum VZV antibody
Limited value due to high prevalence in the general population.
HIV test
Actively performed for herpes zoster in patients under 50 years old.
For VZV-related posterior uveitis (suspected ARN or PORN), empirical treatment should be initiated without waiting for test results. If meningitis is suspected, promptly perform brain MRI and lumbar puncture.
Iris atrophy and heterochromia due to VZV reactivation can resemble FHI and lead to misdiagnosis. Key findings that exclude FHI include vitritis, fine stellate keratic precipitates, low flare values (laser flare photometry <20 ph/ms), no posterior synechiae, and differences in iris texture1). Absence of these findings does not support a diagnosis of FHI.
Combination of antiviral drugs and sufficient steroid eye drops, pupil management, and intraocular pressure management are performed. Antiviral drugs are started from eye ointment, and oral administration is added if the effect is insufficient. It often recurs and relapses, and it is necessary to explain to the patient that treatment will be long-term 2).
Prednisolone acetate 1% or betamethasone 0.1% 4 to 8 times daily (adjusted according to inflammation severity). Tapering should be gradual, and long-term low-dose maintenance may be necessary to prevent recurrence. The use of systemic steroids is controversial and requires caution in immunocompromised states.
Aqueous humor suppressants (beta-blockers, carbonic anhydrase inhibitors) should be actively used. Prostaglandin-related drugs are generally avoided due to the risk of VZV reactivation. In cases with recurrent intraocular pressure spikes, a combination of multiple pressure-lowering agents may be required.
Intravenous systemic antiviral therapy (inpatient management) is necessary. Ganciclovir and foscarnet have higher intraocular bioavailability than acyclovir. Intravitreal antiviral injection may be required in some cases 2).
QCan herpes zoster uveitis occur even after vaccination?
A
Vaccination is not completely preventive but reduces the incidence by about 50%. It is recommended especially for high-risk individuals aged 50 and older. If herpes zoster occurs after vaccination, early initiation of antiviral therapy is important.
VZV latently infects the dorsal root ganglia, and upon reactivation, it travels via the trigeminal nerve axonal flow to form lesions in the cornea and conjunctiva, also spreading intraocularly.
Intraocular mechanisms:
Trabeculitis: Direct invasion of the trabecular meshwork by VZV-infected cells and accumulation of inflammatory cells lead to elevated intraocular pressure. This pattern of elevated pressure, as opposed to decreased pressure due to ciliary body hyposecretion, is characteristic of herpetic ocular hypertension.
Occlusive vasculitis (anterior segment ischemia): Inflammatory occlusion of iris vessels is the main mechanism of sectoral iris atrophy. Partial ischemia of the iris occurs due to occlusive vasculitis of the posterior ciliary arteries. Sectoral atrophy is a finding specific to VZV and is more prominent than in HSV uveitis.
Perineural invasion: Viral invasion of the ciliary nerves causes dysfunction of the iris sphincter muscle (paralytic mydriasis). Ischemic atrophy and neuropathy of the iris sphincter form the basis of paralytic mydriasis.
In acute retinal necrosis (ARN), necrotizing retinitis starting from the peripheral retina progresses to optic neuritis, vasculitis, and retinal detachment. In PORN, VZV primarily affects the outer retina in immunocompromised patients, leading to rapid spread of necrosis and a very poor prognosis.
Confirmation by clinical case:
Papasavas et al. (2021) reported a case of a 45-year-old HIV-positive patient (CD4 332/mm³) in whom VZV uveitis with iris heterochromia was misdiagnosed as FHI1). After discontinuation of steroid eye drops for 10 days, mutton-fat KP, posterior synechiae, and increased flare (20→51.4 ph/ms) appeared, leading to the diagnosis of VZV uveitis. After continuing dual therapy with antivirals and steroids, treatment was adjusted upon initiation of antiretroviral therapy (ART) and recovery of CD4 count. This case demonstrates that LFP value is an important objective indicator in differentiating from FHI.
Some authors suggest that early vitrectomy (pars plana vitrectomy) combined with intravitreal antiviral injection and laser photocoagulation reduces the subsequent incidence of retinal detachment, but this remains controversial. For retinal detachment after acute retinal necrosis, vitrectomy with silicone oil tamponade is required, and long-term management is necessary.
Objective Inflammation Assessment Using Laser Flare Photometry
In addition to qualitative inflammation assessment by slit-lamp examination, quantification of aqueous flare using laser flare photometry (LFP) has been shown to be useful for objective monitoring of HZU 1). Changes in LFP values are used to evaluate treatment response and for differential diagnosis (FHI differentiation).
Papasavvas I, Jeannin B, Herbort CP.. When HIV Immunodeficiency and Heterochromia Confuse the Issue: Recurrent Zoster Uveitis Mistaken for Fuchs’ Uveitis. J Ophthalmic Vis Res. 2021;16(2):295-299. doi:10.18502/jovr.v16i2.9094. PMID:34055267; PMCID:PMC8126730.