Retinal artery occlusion is a disease that causes severe visual dysfunction due to retinal ischemia and necrosis from occlusion of the retinal artery. It is classified into the following three types based on the occlusion site:
Central retinal artery occlusion (CRAO): Occlusion of the central retinal artery. This is the most severe type, and visual outcome is poor, often resulting in counting fingers or worse.
Branch retinal artery occlusion (BRAO): Occlusion of a branch. Visual prognosis varies greatly depending on the occlusion site. It accounts for approximately 38% of all retinal artery occlusions5).
Cilioretinal artery occlusion: Occlusion of the ciliary artery.
In BRAO, the degree of macular involvement greatly affects visual acuity. If the macula is not affected, visual acuity does not decrease, but the visual field corresponding to the occluded area is lost. When occlusion occurs in the nasal artery or in the peripheral temporal area, there are often no subjective symptoms. On the other hand, even with occlusion of an arteriole that only shows cotton-wool spots, a scotoma may be noticed if it is near the macula.
BRAO is classified into two subtypes based on the persistence of occlusion.
Permanent BRAO: The occlusion persists, and retinal ischemic changes become fixed.
Transient BRAO: The occlusion resolves spontaneously, and retinal findings subside. It may present as amaurosis fugax.
Retinal artery occlusion is a highly urgent disease where very early intervention determines visual prognosis. The incidence of CRAO is estimated at about 1 per 100,000 per year, or 1 per 10,000 outpatients. The average age of onset for CRAO is early 60s, more common in men, and often occurs in one eye. 1–2% may occur in both eyes, and bilateral involvement should raise suspicion for giant cell arteritis (GCA) 5). The incidence in Japan is slightly lower than in Western countries.
Asymptomatic retinal emboli are found in about 1.4% of the general population aged 49 years and older (Blue Mountains Eye Study) 5).
In the 2013 AHA/ASA (American Heart Association/American Stroke Association) revised definition of stroke, retinal ischemia was explicitly classified as a type of CNS (central nervous system) infarction 5). About 30% of CRAO patients and about 25% of BRAO patients have concurrent cerebral infarction within one week of onset. The stroke risk in symptomatic RAO patients is highest from 2 weeks before to 1 month after onset 5).
QIs branch retinal artery occlusion related to stroke?
A
BRAO may present as an ocular manifestation of stroke, and about 25% of BRAO patients have concurrent cerebral infarction within one week of onset. The AHA/ASA includes retinal ischemia as CNS infarction, and after onset, systemic evaluation in collaboration with neurology and cardiology is essential. Rapid search for embolic sources such as carotid ultrasound and echocardiography is necessary.
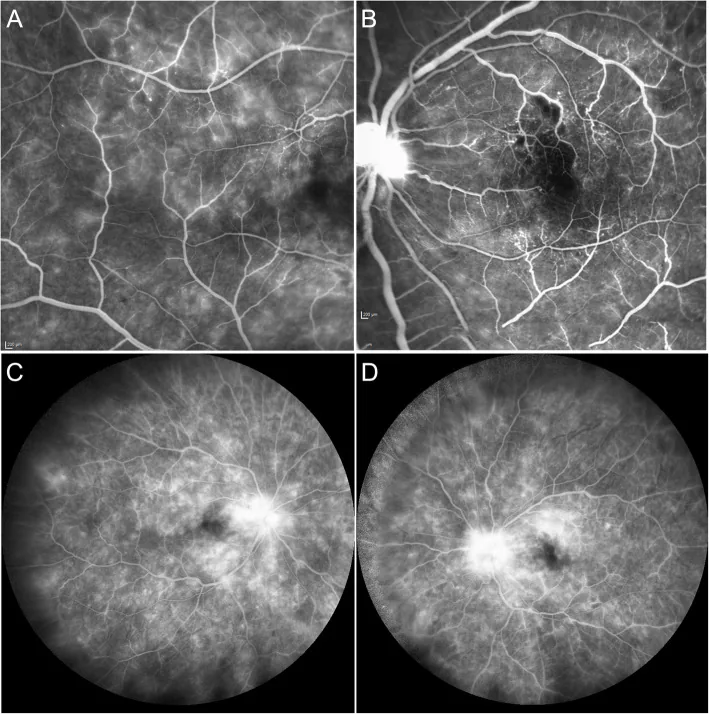
González DP, et al. Occlusive retinal vasculopathy with macular branch retinal artery occlusion as a leading sign of atypical hemolytic uremic syndrome - a case report. BMC Ophthalmol. 2021. Figure 2. PMCID: PMC7847162. License: CC BY.
Fluorescein angiography shows capillary leakage and telangiectasia temporal to the right macula (a), ischemic hypofluorescence due to branch retinal artery occlusion superior to the left macula (b), and late-phase capillary leakage and optic disc staining (c-d). These correspond to the hypofluorescent areas discussed in the section “2. Main Symptoms and Clinical Findings.”
BRAO typically presents with painless acute visual field loss.
Painless acute visual field loss: Sudden, painless visual field loss is the most characteristic symptom.
Monocular visual field defect: Visual field loss corresponding to the territory of the occluded branch.
Decreased visual acuity: Prominent when the branch to the macula is occluded. Occlusion of nasal branches or peripheral temporal branches may preserve visual acuity, and many cases are asymptomatic.
Perception of scotoma: Even in arteriolar occlusion with only cotton wool spots, a scotoma may be perceived if near the macula.
Prodromal symptoms: Some cases develop after repeated episodes of amaurosis fugax.
As examples, a 49-year-old woman developed acute painless visual field defect while taking phentermine, but corrected visual acuity remained 20/201). In a 22-year-old man, a curtain-like superior visual field defect occurred after laser pointer exposure3). A 61-year-old man developed a superior visual field defect during percutaneous transluminal coronary angioplasty (PTCA), and visual acuity decreased to 6/362).
Clinical Findings (Findings Confirmed by Physician Examination)
Retinal whitening: Narrowing of the occluded artery and retinal opacity in its territory, due to ischemic cell swelling.
Cotton wool spots: White lesions reflecting microinfarction of the nerve fiber layer.
Retinal emboli: Emboli are visible in the fundus in 62% of cases, of which 98% are located temporally5). Cholesterol emboli (Hollenhorst plaque) are the most common5).
Resolution of opacity: Retinal opacity resolves after 4–6 weeks, similar to CRAO, and retinal thickness transitions from thickening to thinning. Although the fundus appears normal on ophthalmoscopy, visual field defects in the occluded area persist. This “normal appearance with residual dysfunction” is an important point for patient explanation.
Beading and fragmentation: Characteristic findings of slow-moving microcolumns of blood in the occluded artery.
OCT findings (temporal changes): In the acute phase, the inner retinal layers (from nerve fiber layer to inner nuclear layer) in the occluded area become thickened and hyperreflective (due to intracellular edema). Even after retinal opacity decreases a few days after onset, OCT often shows persistent hyperreflectivity of the inner layers. After several months, the inner retinal layers in the occluded area become thin, but the outer retinal layer structure is preserved. In the chronic phase, OCT may show retrograde atrophy involving not only the inner layers but also the outer layers, making layer structure difficult to identify. The p-MLM (paracentral middle layers maculopathy) sign reflects rapid swelling of bipolar cell synapses2).
OCTA findings: Perfusion deficits in the superficial retinal capillaries are visualized. In permanent BRAO, nonperfusion of the superficial retina has been reported to persist even 9 years after occlusion1).
Fluorescein angiography (FA): Delayed filling of the occluded artery and corresponding vein is observed. The arm-to-retina circulation time is normally about 12 seconds, but during occlusion it often exceeds 30 seconds 3). Irregularities of the vessel wall and leakage of fluorescein are also observed.
Electroretinography (ERG): The a-wave is normal because photoreceptors survive via choroidal nutrition, but the b-wave is reduced or absent due to damage to bipolar cells and Müller cells, showing a negative-type ERG. A normal a-wave indicates photoreceptor survival, and a reduced b-wave indicates dysfunction of the inner nuclear layer (bipolar cells and Müller cells), used to assess the depth of retinal ischemia.
The visual prognosis of BRAO is shown in the table below 5).
Classification
Initial visit 20/40 or better
Follow-up 20/40 or better
Permanent BRAO
74%
89%
Transient BRAO
94%
100%
QDoes vision return in BRAO?
A
80% of BRAO cases ultimately maintain a corrected visual acuity of 0.5 or better. In permanent BRAO, 89% maintain 20/40 or better at follow-up 5). In transient BRAO, 100% achieve 20/40 or better. However, if the branch to the macula is occluded, the visual prognosis may be poor. Patients should be informed that visual field defects often persist even after the opacity resolves.
The majority of BRAO cases are embolic. It tends to occur in elderly individuals with systemic diseases such as hypertension, arteriosclerosis, and diabetes. Atheromas of the internal carotid artery or intracardiac thrombi formed by heart disease become emboli. Vasculitis, infection, trauma, and vasospasm can also be causes. In young patients, abnormalities of the blood coagulation system, heart disease, congenital anomalies, and retinal vasculitis are often observed.
The main types and origins of emboli are shown below.
Cases have been reported as thromboembolism due to PTCA2) and as plaque dislodgement during neuroendovascular treatment4). Retinal artery occlusion due to cosmetic skin filler injections (e.g., hyaluronic acid) is increasing and attracting attention5).
Vasospasm: Migraine, cocaine, sildenafil use, etc. can cause vasospasm and lead to BRAO.
Vasculitis: Behçet’s disease, giant cell arteritis (GCA), etc. In patients aged 50 years or older, GCA should be actively considered 5). Arteritic CRAO accounts for about 4% of CRAO patients and has the worst prognosis. When GCA is suspected, check for symptoms such as headache, scalp tenderness, and jaw claudication, and promptly measure erythrocyte sedimentation rate and CRP.
Coagulation abnormalities: Antiphospholipid antibody syndrome, thrombophilia, etc. In young patients, a thorough evaluation of the coagulation system is particularly important.
Susac syndrome: An autoimmune disease characterized by the triad of encephalopathy, sensorineural hearing loss, and BRAO 5).
Drug-induced: An association with the sympathomimetic agent phentermine (37.5 mg/day) has been reported 1).
Laser pointer injury: The world’s first case of BRAO caused by a 3-second exposure to a blue laser with a wavelength of 450–495 nm was reported 3).
Hypertension: The most important modifiable risk factor 5)
Dyslipidemia: About 60% of patients have at least one undiagnosed vascular risk factor, with dyslipidemia being the most common
Low HDL cholesterol: An independent risk factor 5)
Diabetes mellitus
Smoking
Atrial fibrillation5)
High BMI
Obstructive sleep apnea syndrome
QCan BRAO occur even while taking medication?
A
Phentermine (an appetite suppressant) has been reported to induce BRAO by causing vasoconstriction and vasospasm through its norepinephrine reuptake inhibition effect1). Cocaine, sildenafil, and filler injections can also be causes5). It is important to inform your ophthalmologist and internist of any pre-existing conditions and medications you are taking.
The diagnosis of BRAO is based on fundus findings and combines multiple imaging tests and systemic evaluation. It is highly urgent, and the time required for diagnosis should be minimized.
Non-perfusion areas of superficial retinal capillaries (non-invasive)
Ophthalmoscopy: Confirms retinal whitening in the distribution of the occluded artery, narrowing and white sheathing of the occluded artery, cotton-wool spots, and visualization of emboli. Blood may not be visible within the vessel.
OCT: Evaluates the transition from acute inner layer thickening and hyperreflectivity (intracellular edema) to chronic inner layer thinning (ischemic atrophy). In the acute phase, paracentral acute middle maculopathy (PAMM) may be observed 5). Retinal and choroidal thinning occurs within weeks. Preservation of the outer layers is an important sign of photoreceptor survival.
OCTA: Non-invasively visualizes non-perfusion areas of superficial retinal capillaries 1, 4). Perfusion deficits may persist in the chronic phase 1).
Fluorescein angiography (FA): Evaluates delayed filling or filling defects of the occluded artery, irregular vessel walls, fluorescein leakage, and prolonged retinal circulation time 3). The arm-to-retina circulation time is normally about 12 seconds but is often prolonged to 30 seconds or more.
Visual field testing: Confirms visual field defects corresponding to the occluded area.
Electroretinography (ERG): Assesses inner retinal ischemia via a negative-type ERG pattern with normal a-wave and reduced b-wave. Normal a-wave indicates photoreceptor survival, while reduced b-wave indicates damage to bipolar cells and Müller cells.
Acute symptomatic RAO warrants immediate referral to a stroke center 5). CRAO, BRAO, and transient monocular vision loss share risk factors (atherosclerosis, carotid artery disease, atrial fibrillation, valvular heart disease, etc.) with cerebral infarction. When encountered, prompt evaluation for cerebral infarction and its risk should be performed.
Carotid ultrasound: Evaluation of stenosis and plaque. For symptomatic carotid stenosis (50–99%), carotid endarterectomy shows better outcomes than medical therapy 5).
Echocardiography and electrocardiography: Search for cardiac embolic sources and detection of atrial fibrillation.
Blood tests: Erythrocyte sedimentation rate and CRP (to rule out giant cell arteritis), complete blood count and coagulation studies (to rule out hematologic disorders). In patients aged 50 years or older, GCA should be actively considered 5). If GCA is strongly suspected, urgent systemic steroid therapy should be considered 5).
MRI/CT: Evaluation of asymptomatic cerebral infarction.
On the other hand, for asymptomatic BRAO or incidentally discovered retinal emboli, there is currently no evidence supporting urgent stroke evaluation 5).
Irreversible retinal changes begin approximately 100 minutes after arterial occlusion. For CRAO, treatment immediately after onset is preferable, but active treatment should be considered even within one day of onset. For BRAO with visual impairment in the early stage, treatment similar to CRAO is performed.
Vasodilators
Amyl nitrite: Crush a 0.25 mL vial, absorb into a cover, and inhale through the nostrils (caution for hypotension; off-label use).
Carbogen inhalation: Inhalation of a mixture of 95% oxygen and 5% CO₂.
Pharmacotherapy
Urokinase: Initial daily dose of 60,000 to 240,000 units, then gradually reduced over approximately 7 days. Caution for cerebral hemorrhage and systemic bleeding tendency.
Diamox injection: 500 mg intravenous injection once daily (off-label use). Lowers intraocular pressure to promote retinal artery dilation.
Ovalmon tablets: 5 μg × 6 tablets, divided into three doses after meals (for blood flow improvement).
Systemic Evaluation and Management
Search for embolic source: Carotid ultrasound, echocardiography, and coagulation tests are performed urgently.
Referral to stroke center: Acute symptomatic RAO is highly associated with stroke, and immediate referral is recommended5).
Antiplatelet therapy: Recommended according to AHA stroke guidelines if no contraindications.
In the acute phase, the following treatments are performed depending on symptoms.
Ocular massage / anterior chamber paracentesis: Intermittent pressure on the eye lowers intraocular pressure and promotes peripheral migration of the embolus. Anterior chamber paracentesis (removing 0.1–0.4 mL with a 27G needle) is also performed to lower intraocular pressure. However, note that conservative treatments (ocular massage, anterior chamber paracentesis, carbogen) have not been proven to be significantly effective5).
Stellate ganglion block: May be performed to improve ocular blood flow.
Amyl nitrite inhalation: Crush a 0.25 mL vial and inhale. It aims to improve retinal blood flow through vasodilation (off-label use).
Acetazolamide (Diamox) intravenous injection: 500 mg IV. As a carbonic anhydrase inhibitor, it lowers intraocular pressure and promotes retinal artery dilation (off-label use).
Urokinase intravenous injection: Initial daily dose 60,000–240,000 units, then gradually reduced over about 7 days. Caution is needed for cerebral hemorrhage and systemic bleeding tendency.
Opalmon tablets (limaprost alfadex): 5 μg × 6 tablets, divided into three doses after meals. A prostaglandin E₁ derivative, it aims to improve peripheral blood flow.
If vasospasm is the cause, calcium channel blockers may be effective2).
t-PA preparations specifically adsorb to thrombi and act, making them superior in both efficacy and side effects. Currently, t-PA therapy is considered one of the best treatments for acute CRAO. Alteplase (Activacin®) is approved for cerebral infarction and myocardial infarction but is not approved for CRAO. Intravenous therapy is performed at multiple facilities after obtaining approval for off-label use.
The natural recovery rate of visual acuity in CRAO is 10–20%, but it is reported to increase to around 40% with early thrombolytic therapy. A meta-analysis has shown that intravenous (IV) tPA administration within 4.5 hours of onset may be associated with improved outcomes 5).
On the other hand, the EAGLE study (RCT) found no significant difference in visual improvement between intra-arterial (IA) tPA and conservative treatment, and safety concerns regarding intracranial hemorrhage (ICH) were raised 4). Currently, evidence for intra-arterial and intravenous fibrinolytic therapy for BRAO/CRAO is considered insufficient 5).
Hyperbaric oxygen therapy has been suggested to have mild effects in some small retrospective studies, but a Cochrane review concluded that the evidence is uncertain 5).
Monitoring for neovascularization: Iris neovascularization and retinal neovascularization may occur after occlusion. In CRAO, iris neovascularization occurs in up to 20% of cases, typically appearing 30–60 days after onset 5). Watch for the development of neovascular glaucoma (NVG), and panretinal photocoagulation (PRP) is indicated 5). Regular ophthalmic examinations are important for about 4 months after onset.
Systemic management: Control of risk factors for systemic atherosclerosis (hypertension, dyslipidemia, obesity, obstructive sleep apnea syndrome) is important. Dietary therapy, regular exercise, and smoking cessation are also recommended.
80% of BRAO patients ultimately maintain a corrected visual acuity of 0.5 or better. In permanent BRAO, 89% maintain 20/40 or better at follow-up 5). In transient BRAO, 100% achieve 20/40 or better.
Visual outcomes in CRAO are poor, with only about 18% of CRAO patients experiencing spontaneous visual recovery. Retinal opacification resolves after 4–6 weeks, but visual function does not recover unless early treatment is effective. In BRAO, even if the occluded vessel recanalizes, visual field defects usually persist, but visual acuity itself may be preserved if the macula is not affected.
QHow soon should one seek medical attention after onset?
A
Ischemic changes in the retina begin to become irreversible approximately 100 minutes after arterial occlusion. A general guideline is to actively attempt treatment within one day of onset, but earlier treatment leads to better prognosis. In CRAO, the rate of visual improvement is high if treatment is initiated within 100 minutes. Additionally, because the risk of stroke is high (about 25% in BRAO patients), it is important to immediately visit an ophthalmologist or emergency department and coordinate with a neurologist after symptom onset.
The retinal artery supplies the inner two-thirds of the retina (from the nerve fiber layer to the inner nuclear layer). Photoreceptors in the outer retina receive nutrition from the choroidal vessels and survive. In BRAO, only the inner retina in the territory of the occluded branch becomes ischemic, while the outer layer is preserved by oxygen and nutrients from the choroid. The ERG finding of preserved a-wave (photoreceptor survival) and reduced b-wave (bipolar cell and Müller cell dysfunction) directly reflects this anatomical characteristic.
The cilioretinal artery, a branch of the short posterior ciliary artery, is present in about 32% of all eyes and supplies the retina near the papillomacular bundle. Even if CRAO occurs, if the cilioretinal artery is preserved, retinal function near the papillomacular bundle may be maintained, and central vision may be preserved.
The most common cause of RAO is thromboembolism, which often occurs at the narrowest part of the central retinal artery lumen, i.e., where it penetrates the dural sheath of the optic nerve. Emboli originate from plaques in the carotid artery or heart.
Hollenhorst plaques consist of cholesterol crystals that break off from atherosclerotic plaques in the carotid artery or aortic arch and become lodged at bifurcations of the retinal artery 5). The occluded artery may become markedly narrowed and white, with no blood visible inside the vessel.
Severe retinal damage occurs approximately 100 minutes after arterial occlusion. In the hyperacute phase (up to 2 hours), the fundus may appear nearly normal, but OCT shows the beginning of inner layer hyperreflectivity. In the acute phase (2 hours to several days), retinal whitening becomes clear, with arterial narrowing and OCT inner layer thickening and hyperreflectivity prominent. In the subacute phase (1 to 6 weeks), opacity subsides, and iris or retinal neovascularization may appear. In the chronic phase (after 6 weeks), inner layer thinning and retrograde atrophy extending to the outer layer occur, along with optic disc pallor. In chronic hypertension, the time to irreversible change may be extended up to 240 minutes according to some reports 4, 2).
Sano et al. (2025) retrospectively investigated the effect of early PGE₁ administration in CRAO patients within 24 hours of onset at Tokushima Red Cross Hospital6). In the PGE₁ group (n=4), alprostadil alfadex 40 μg was dissolved in 250 mL saline and infused at 125 mL/h twice daily (80 μg/day) for 5 days, followed by oral limaprost alfadex 10 μg three times daily (30 μg/day) for at least 1 month. Compared to the conventional treatment group (n=6), the PGE₁ group had significantly better best-corrected visual acuity (BCVA) at 1 month. Baseline maximum retinal thickness (MRT) showed a negative correlation with 1-month BCVA, suggesting it may be a prognostic predictor. No adverse events were observed in either group6).
PGE₁ is thought to have neuroprotective effects through vasodilation and reduction of oxidative stress and inflammation. Although the sample size is small and a prospective RCT is needed, these findings are noteworthy given the lack of proven efficacy of existing treatments.
Since the 2013 AHA/ASA revised definition recognized retinal ischemia as CNS infarction5), momentum has increased for applying stroke protocols to acute RAO. Immediate referral to a stroke center and establishment of systemic management systems analogous to cerebral infarction are being promoted.
Meta-analyses have reported that IV tPA administration within 4.5 hours of onset may be associated with improved visual recovery rates, but the EAGLE study did not show efficacy of IA tPA and raised safety concerns4), and sufficient RCT evidence for IV tPA is lacking5).
Advances in OCTA technology have made it possible to track superficial retinal perfusion deficits for more than 9 years after onset 1). Research is investigating whether acute-phase perfusion deficit patterns may serve as predictors of long-term prognosis.
The “spot sign” for detecting calcific emboli on orbital ultrasound has been reported with a sensitivity of 83% and specificity of 100% 4), and is attracting attention as a non-invasive adjunct for acute-phase diagnosis.
Although some small retrospective studies suggest efficacy, a Cochrane review concluded that the evidence for interventions in non-arteritic CRAO overall is uncertain 5).
PGE₁ Therapy
Report from Japan: In CRAO, PGE₁ (alprostadil 80 μg/day × 5 days) significantly improved BCVA at 1 month 6).
Prognosis prediction: Baseline MRT (maximum retinal thickness) was negatively correlated with visual acuity at 1 month. No adverse events.
Current Status of tPA
EAGLE trial: IA tPA showed no visual improvement compared to conservative treatment and carried a risk of ICH 4).
IV tPA: Meta-analysis suggests potential for improved visual recovery rates within 4.5 hours of onset, but RCT evidence is insufficient 5).
Liu J, Rosenfeld PJ, Dubovy SR. Branch retinal artery occlusion in a 49-year-old woman taking phentermine. Am J Ophthalmol Case Rep. 2024;35:102013. doi:10.1016/j.ajoc.2024.102013. PMID:38884112; PMCID:PMC11179534.
Zokri MF, Othman O. A Case Series of Retinal Artery Occlusion: When Time Is of the Essence. Cureus. 2024;16(5):e60520. doi:10.7759/cureus.60520. PMID:38883137; PMCID:PMC11180524.
Gebara A, Vofo BN, Jaouni T. Branch retinal artery occlusion from laser pointer misuse. American journal of ophthalmology case reports. 2024;36:102118. doi:10.1016/j.ajoc.2024.102118. PMID:39156905; PMCID:PMC11327539.
Dalzotto K, Richards P, Boulter TD, Kay M, Mititelu M. Complications of Intra-Arterial tPA for Iatrogenic Branch Retinal Artery Occlusion: A Case Report through Multimodal Imaging and Literature Review. Medicina (Kaunas, Lithuania). 2021;57(9). doi:10.3390/medicina57090963. PMID:34577886; PMCID:PMC8464858.
Kovach JL, Bailey ST, Kim SJ, Lim JI, Vemulakonda GA, Ying GS, et al. Retinal and Ophthalmic Artery Occlusions Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P270-P302. doi:10.1016/j.ophtha.2024.12.024. PMID:39918522.
Sano H, Yanai R, Kondo H, Mitamura Y. Early prostaglandin E(1) treatment improves visual outcomes in central retinal artery occlusion: a retrospective study. Frontiers in ophthalmology. 2025;5:1665519. doi:10.3389/fopht.2025.1665519. PMID:40909332; PMCID:PMC12404978.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.