Acquired retinal arterial macroaneurysm (RAM) is a localized saccular or fusiform dilation of a retinal artery within the third-order branches. It is often observed protruding from the artery at bifurcations or arteriovenous crossings. Exudation or hemorrhage from RAM causes morphological changes and functional impairment. This disease concept was first reported by Robertson in 1973.
The typical size is 100–250 μm 1, 3). About 50% occur in the superotemporal artery and about 45% in the inferotemporal artery; nasal involvement is rare 3). Although more common on the temporal side, it can also occur on the nasal side. Most cases are unilateral and solitary, but bilateral and multiple cases exist. It is common in elderly individuals with a history of hypertension and arteriosclerosis.
RAM occurring on the optic disc is rare, accounting for 3.7–8% of all cases 7, 10). RAM is known to have a tendency for spontaneous regression, which influences treatment decisions.
QHow rare is acquired retinal arterial macroaneurysm?
A
Although relatively rare, the chance of encountering this condition is increasing with the aging population. RAM on the optic disc is even rarer, reported to account for 3.7–8% of all cases 7, 10). In the hemorrhagic type, bleeding or exudation involving the macula can cause severe visual impairment, so early diagnosis and management are important.
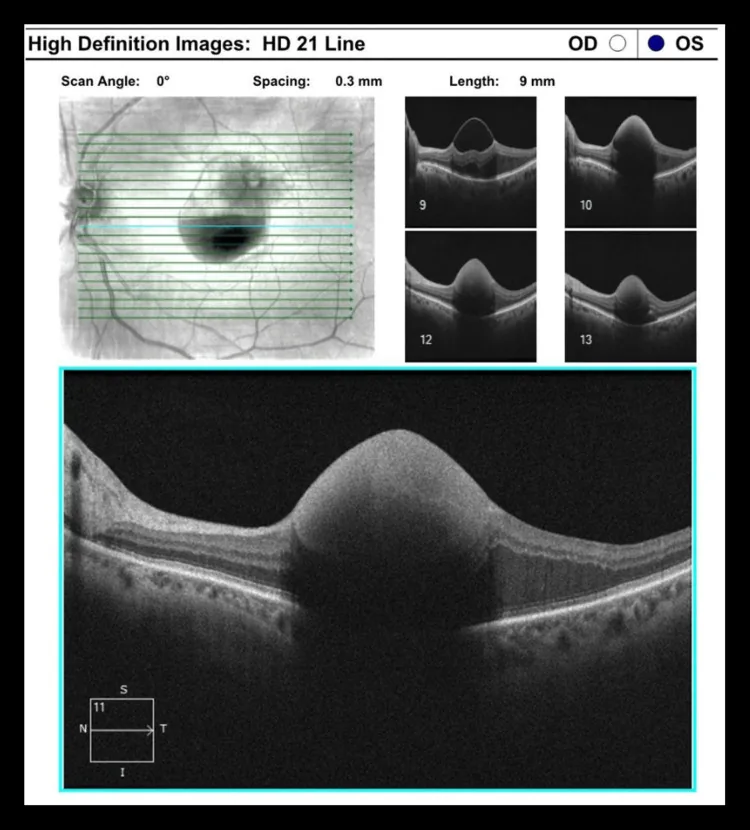
Jemelian A, et al. Outcomes of Combined Therapy With Focal Laser and Intravitreal Bevacizumab for Retinal Arterial Macroaneurysm: A Case Series. Cureus. 2025. Figure 2. PMCID: PMC12034429. License: CC BY.
This is an OCT tomographic image. It corresponds to the dome-shaped hyperreflective lesion discussed in section “2. Main Symptoms and Clinical Findings.”
When exudation or hemorrhage involves the macula, it causes decreased vision and metamorphopsia. If there is no bleeding or exudation, there are no subjective symptoms and it is difficult to detect.
When hemorrhage or exudation extends to the macula, the following symptoms occur:
Decreased vision: Vision loss due to hemorrhage or exudation in the macula. It may be gradual or sudden.
Metamorphopsia (distorted vision): Caused by macular edema or exudation.
Central scotoma: Visual field defect due to damage to the fovea.
RAM is clinically classified into the following three types 3, 9).
Type
Main Symptoms
Typical Findings
Asymptomatic type
None
Incidental finding
Hemorrhagic type
Acute vision loss
Multilayered hemorrhage
Exudative type
Slow vision loss
Hard exudates, edema
Hemorrhage characteristic of RAM is multilayered, involving multiple layers including subretinal, intraretinal, sub-internal limiting membrane (ILM), preretinal, and vitreous 9). This multilayered hemorrhage pattern is one of the characteristic findings of RAM.
On fundus examination, it appears red along the retinal arterioles, white if accompanied by fibrin, and gray-white if fibrotic. The aneurysm may not be identifiable due to hemorrhage or exudation. In the exudative type, circinate retinopathy, retinal edema, and serous retinal detachment are observed, and a ring of hard exudates (circinate retinopathy) may surround the aneurysm.
Multilayered hemorrhage (hemorrhage across multiple layers: subretinal, intraretinal, and vitreous) is a characteristic finding of RAM and an important clue for diagnosis 9). However, when hemorrhage is extensive, the aneurysm itself may be difficult to visualize, making supplementary evaluation with IA, OCT, or OCTA essential for diagnosis 3).
The development of RAM involves multiple risk factors that promote weakening of the blood vessel wall. It is more common in elderly individuals with a history of hypertension and arteriosclerosis. It is thought that loss of the muscular layer of the vessel wall and collagen fibrosis of the media reduce elasticity, leading to dilation due to intraluminal pressure 1, 9).
Major Risk Factors
Hypertension: The greatest risk factor, present in 51–75% of patients. Sustained hypertension promotes hyaline degeneration and arteriosclerosis of the vessel wall 9).
Arteriosclerosis: Weakening of the vessel wall due to hyaline degeneration and collagenization. Long-term vessel wall damage forms the basis for dilation 1, 9).
Aging: Commonly occurs in people aged 60 years and older. Age-related weakening of the vessel wall is a background factor.
Female sex: Women account for 70–78% of patients. The detailed mechanism of the sex difference is unknown 9).
Other Risk Factors
Dyslipidemia: Promotes the progression of arteriosclerosis and worsens vessel wall damage 1, 3).
Cardiovascular disease: An association with coronary artery disease and aortic aneurysm has been reported. RAM may occur as part of systemic vascular disease 9).
Lynch syndrome: Possible increased complexity of the vascular network due to DNA repair gene mutations has been suggested. This is the first reported case of an association with RAM 1).
Valsalva maneuver: Sudden blood pressure fluctuations can trigger RAM rupture. Heavy labor, coughing, and straining during defecation have been reported as triggers 9).
Multimodal imaging is essential for accurate diagnosis of RAM 3). Especially when there is extensive hemorrhage, identification of the aneurysm itself may be difficult with FA alone, and a combination of multiple examinations is necessary.
Fluorescein angiography (FA): In the arterial phase, aneurysmal hyperfluorescence of RAM is observed, and in the late phase, leakage and tissue staining are seen. When hyperfluorescence due to dye leakage or tissue staining is strong, it is judged as a finding indicating increased permeability of the aneurysm wall and activity. It is useful for assessing activity and is the standard diagnostic method.
Indocyanine green angiography (IA): In cases with extensive hemorrhage, IA is superior to FA for detecting RAM 3). Since indocyanine green shows weaker fluorescence leakage from aneurysms than fluorescein, hyperfluorescence on IA indicates higher activity.
Optical Coherence Tomography (OCT): Depicts RAM as a highly reflective spherical structure in the inner retina. It enables confirmation and quantification of retinal edema and serous retinal detachment, and is also useful for stratifying the location of hemorrhage (preretinal or subretinal).
Optical Coherence Tomography Angiography (OCTA): Noninvasively visualizes blood flow signals. It can depict intramural passages due to dissecting changes in the vessel wall 8).
Laser Speckle Flowgraphy (LSFG): A method for noninvasive quantitative assessment of blood flow. The Mean Blur Rate (MBR) value correlates with RAM regression and can be used to monitor treatment progress 5).
Near-Infrared Reflectance Imaging (NIR-R): A case report has detected cuff-type vessel wall thickening 3 years before onset, suggesting its potential as an early detection tool 6).
B-mode Ultrasound: Used when fundus visualization is impossible due to vitreous hemorrhage7, 10). It allows rough evaluation of intraocular lesions.
The treatment strategy for RAM is determined based on the disease type, impact on the macula, and tendency for spontaneous regression. Although spontaneous remission is possible, the degree of visual dysfunction and recovery varies depending on the extent of persistent exudation or hemorrhage affecting the macula.
Observation: Since there is a tendency for spontaneous remission, this applies to cases without macular involvement or asymptomatic cases. Follow-up with regular fundus examinations.
Pharmacotherapy: Carbazochrome (Adona tablets 30 mg) 3 tablets divided into 3 doses. This is an adjunctive treatment aimed at suppressing increased vascular permeability and achieving hemostasis.
Risk factor management: Strict control of blood pressure and lipids is essential for preventing recurrence and controlling disease activity.
Invasive Treatments
Laser photocoagulation: Aimed at promoting wound healing of the permeable or ruptured wall of the aneurysm. The surface of the aneurysm is gently treated to avoid occluding the artery; it is not necessary to repeatedly apply laser until the entire aneurysm shows gray-white coagulation. Typical settings: spot size 300–500 μm, exposure time 0.2–0.3 seconds, power 120 mW or more. A complication is the risk of arterial occlusion.
Intravitreal anti-VEGF injection: Used for exudative RAM. Not covered by insurance in Japan 2, 3, 4).
Vitrectomy: When blood accumulates between the ILM and the nerve fiber layer, vitrectomy with ILM peeling is performed. Persistent vitreous hemorrhage is also an indication for vitrectomy.
Indirect coagulation: A technique that coagulates the retina around the aneurysm to divert leakage away from the macula. Often combined with direct coagulation.
Laser + anti-VEGF combination therapy: In a study of 3 cases, mean central retinal thickness (CRT) decreased by 275.7 μm and visual acuity improved by 0.55 logMAR 4).
Nd:YAG laser: Used for drainage of sub-ILM hemorrhage. Early treatment is recommended 9).
Intravitreal gas injection (pneumatic displacement): Indicated within 2 weeks of subretinal hemorrhage involving the macula. Not indicated if the hemorrhage has already organized. Inject 0.2–0.8 mL of SF6 or C3F8, followed by prone positioning for 1–2 weeks postoperatively. Combination with tPA (tissue plasminogen activator) may enhance displacement of submacular hemorrhage.
Subthreshold laser: Reported to have similar efficacy to conventional laser with fewer complications 9).
QCan it heal on its own?
A
RAM has a tendency to spontaneously regress, and many asymptomatic cases improve with observation alone. However, when hemorrhage or exudation involves the macula, it affects visual prognosis, so active treatment intervention should be considered. The choice between natural course and treatment intervention is made based on a comprehensive assessment of disease type, disease activity, and patient background.
The core pathophysiology of RAM is degeneration of the vessel wall structure and increased intraluminal pressure. Weakening of the vessel wall due to hypertension and arteriosclerosis forms the basis, and leakage due to increased permeability of the arterial wall and hemorrhage due to rupture lead to visual dysfunction.
Vessel wall degeneration process: Hypertension-induced hyaline degeneration and arteriosclerosis damage the muscular layer of the vessel wall, leading to progressive collagen fibrosis of the media 9). As a result, the elasticity of the vessel wall decreases, resistance to intraluminal pressure is lost, and local dilation occurs 1, 9).
Gass hypothesis: Atheromatous emboli damage the vessel wall, causing local ischemia and upregulation of VEGF expression. This promotes increased permeability and vasodilation 2). VEGF induces arterial dilation and increased permeability via endothelial NO production, contributing to the pathology of exudative RAM 3).
Dissection-like changes: Detailed observations using adaptive optics scanning laser ophthalmoscopy (AOSLO), OCT, and OCTA have reported a pathology in which cracks occur in the vessel wall, forming intramural pathways 8). New RAM may form from these intramural pathways in adjacent areas.
Rupture mechanism: Rupture occurs when intraluminal pressure exceeds the threshold of the weakened vessel wall 9). A sudden rise in blood pressure due to Valsalva maneuver (coughing, heavy lifting, straining during defecation, etc.) can trigger rupture 9).
Meng Y et al. reviewed cases of RAM rupture triggered by Valsalva maneuver and discussed the mechanism by which a sudden increase in intra-abdominal pressure causes a rapid rise in venous and arterial pressure, leading to rupture of the fragile vessel wall 9).
Breakdown of the blood-retinal barrier: In exudative RAM, disruption of the blood-retinal barrier underlies macular edema and hard exudates 15).
Characteristics of RAM on the optic disc: Arteries near the optic disc have a large diameter and high blood flow velocity. Therefore, wall stress is high, and vitreous hemorrhage tends to occur early 10).
Microstructural analysis using adaptive optics scanning laser ophthalmoscopy (AOSLO): Detailed observations with AOSLO have visualized the disappearance of pulsation, thrombus formation, and vascular wall fissures in RAM 8). This has revealed a new pathological condition resembling dissecting changes in the vascular wall, deepening the understanding of the pathogenesis.
Longitudinal evaluation using laser speckle flowgraphy (LSFG): It has been reported that as RAM regresses, the mean blur rate (MBR) significantly decreases from 6.8 AU to 1.1 AU 5). Non-invasive blood flow monitoring with LSFG is promising as an objective evaluation tool for treatment efficacy.
Hanazaki H et al. longitudinally evaluated ocular blood flow in treated RAM using LSFG and showed that the decrease in MBR correlated with RAM regression 5).
Early detection using near-infrared reflectance imaging (NIR-R): A case has been reported in which cuff-type vascular wall thickening was detected on NIR-R images three years before RAM became clinically apparent 6). This suggests potential as a predictive factor in hypertensive patients and is expected to be applied as an early screening tool.
Efficacy of combined laser and anti-VEGF therapy: In a series of three cases, treatment combining focal laser photocoagulation and intravitreal bevacizumab resulted in a mean decrease in central retinal thickness (CRT) of 275.7 μm and an improvement in visual acuity of 0.55 logMAR 4). A synergistic effect of vascular stabilization by anti-VEGF and wall repair by laser is suggested, and larger trials are expected.
Subthreshold laser: Compared to conventional threshold laser, sublethal retinal hyperthermia mediated by heat shock proteins is said to achieve equivalent effects while reducing complications 9).
Association between Lynch syndrome and RAM: The onset of RAM in a patient with Lynch syndrome, which involves DNA repair gene mutations, has been reported for the first time 1). It is suggested that DNA repair gene mutations may complicate the vascular network and that increased VEGF-A expression may contribute to the development of RAM.
Need for treatment guidelines: With the diversification of treatment methods, the development of evidence-based clinical practice guidelines is required 9).
Accumulation of cases with multilayered hemorrhage and noninvasive imaging evaluation: In ruptured RAM, cases showing multilayered hemorrhage such as subretinal, intraretinal, and vitreous hemorrhage have been reported 11). In cases complicated by subvitreal hemorrhage, the indication for Nd:YAG laser or vitrectomy is important 12). Near-infrared reflectance videography is used for evaluating the pulsatility of RAM, and OCTA is used for noninvasive evaluation of blood flow within the lesion 13, 14).
QIs anti-VEGF treatment effective for RAM?
A
Case reports and small series have reported the efficacy of intravitreal anti-VEGF injections for exudative RAM 2, 3, 4). Particularly promising results have been obtained when combined with laser therapy 4). However, it is not covered by insurance in Japan 2), and large-scale randomized trials have not yet been conducted. It is necessary to have thorough consultation with the attending physician before use.
Sood S, Friedman S. Retinal Arterial Macroaneurysm in a Patient With Lynch Syndrome. J VitreoRetinal Diseases. 2023;7(3):239-241.
Takamiya M. The Management of Two Cases with Retinal Arterial Macroaneurysm by Anti-Vascular Endothelial Growth Factor. Case reports in ophthalmology. 2024;15(1):490-496. doi:10.1159/000538998. PMID:39015226; PMCID:PMC11249609.
Balas M, Mandell MA, Arjmand P. Juxtafoveal Retinal Arterial Macroaneurysm Diagnosed on Ancillary Imaging. Journal of vitreoretinal diseases. 2024;8(5):609-613. doi:10.1177/24741264241262102. PMID:39318990; PMCID:PMC11418749.
Jemelian A, Enghelberg M. Outcomes of Combined Therapy With Focal Laser and Intravitreal Bevacizumab for Retinal Arterial Macroaneurysm: A Case Series. Cureus. 2025;17(3):e81382. doi:10.7759/cureus.81382. PMID:40291271; PMCID:PMC12034429.
Hanazaki H, Yokota H, Aso H, et al. Evaluation of ocular blood flow over time in a treated retinal arterial macroaneurysm using laser speckle flowgraphy. Am J Ophthalmol Case Rep. 2021;21:101022.
Zienkiewicz A, Francone A, Cirillo MP, Zompa T, Charles M. Near-Infrared Reflectance Imaging to Detect an Incipient Retinal Arterial Macroaneurysm. Case reports in ophthalmology. 2021;12(1):150-153. doi:10.1159/000513344. PMID:33976673; PMCID:PMC8077541.
Takahashi S, Nishida K, Sakaguchi H, Nishida K. A Case of Idiopathic Dense Vitreous Hemorrhage: Suspected Rupture of a Large Retinal Arterial Macroaneurysm on the Optic Disc. Case reports in ophthalmology. 2021;12(2):634-639. doi:10.1159/000511110. PMID:34413754; PMCID:PMC8339441.
Ishikura M, Muraoka Y, Kadomoto S, Nishigori N, Murakami T, Ooto S, et al. Retinal arterial macroaneurysm rupture caused by dissection-like change in the vessel wall. American journal of ophthalmology case reports. 2022;25:101346. doi:10.1016/j.ajoc.2022.101346. PMID:35128170; PMCID:PMC8807975.
Meng Y, Xu Y, Li L, He L, Yi Z, Chen C. Retinal arterial macroaneurysm rupture by Valsalva maneuver: a case report and literature review. BMC ophthalmology. 2022;22(1):461. doi:10.1186/s12886-022-02662-x. PMID:36451117; PMCID:PMC9710132.
Sasajima H, Zako M, Aoyagi A, Ueta Y, Suzuki T. Acute Onset of Dense Vitreous Hemorrhage Associated with Retinal Arterial Macroaneurysm on the Optic Disc. Case reports in ophthalmology. 2022;13(3):763-769. doi:10.1159/000526928. PMID:36845452; PMCID:PMC9944217.
Temkar S, Stephen M, Agarwal D, Deb AK. Multilayered retinal bleed in ruptured retinal artery macroaneurysm. BMJ case reports. 2023;16(4). doi:10.1136/bcr-2023-254669. PMID:37015766; PMCID:PMC10083764.
Mahjoub A, Zaafrane N, Ben Youssef C, Sellem I, Guiga A, Jabri A, et al. Retinal artery macroaneurysm complicated with subhyaloid hemorrhage: two case reports. Annals of medicine and surgery (2012). 2023;85(4):1130-1136. doi:10.1097/MS9.0000000000000361. PMID:37113883; PMCID:PMC10129110.
Abdul-Rahman A, Morgan W, Yu DY. Near infra-red reflectance videography in the evaluation of retinal artery macroaneurysm pulsatility. American journal of ophthalmology case reports. 2022;27:101664. doi:10.1016/j.ajoc.2022.101664. PMID:35938146; PMCID:PMC9352520.
Mohd Lokman M, Catherine Bastion ML, Che Hamzah J. Objective Assessment of Retinal Artery Macroaneurysm With Optical Coherence Tomography Angiography. Cureus. 2022;14(12):e32328. doi:10.7759/cureus.32328. PMID:36628049; PMCID:PMC9825258.
O’Leary F, Campbell M. The blood-retina barrier in health and disease. The FEBS journal. 2023;290(4):878-891. doi:10.1111/febs.16330. PMID:34923749. doi:10.1111/febs.16330. PMID:34923749.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.