Radiation cataract is caused by ocular radiation exposure. Even low-dose exposure increases the long-term risk of cataract, and exposure in emergency workers at nuclear power plant accidents, occupational exposure in healthcare workers, and medical exposure from CT scans, etc., also pose a long-term risk of cataract.
Radiation retinopathy (RR) is a chronic progressive occlusive retinal microvascular disorder that develops when the retina is included in the radiation field during radiotherapy for intraocular tumors, orbital or paranasal sinus tumors, intracranial diseases, etc. A meta-analysis reported that the prevalence of RR after radiotherapy for brain and head and neck tumors is approximately 6%, and that of optic neuropathy is approximately 2% 3). The overall incidence including late-onset cases is reported to be approximately 17% 4).
The incidence by irradiation site is as follows:
Irradiation site
Incidence
Orbit
85.7%
Paranasal sinus
45.4%
Nasopharynx
36.4%
Brain
3.1%
Radiation optic neuropathy rarely occurs after radiotherapy for paranasal sinus tumors or lesions at the base of the skull. The predilection site is the optic chiasm or its vicinity.
QDoes everyone who receives radiotherapy develop ocular disorders?
A
The incidence varies greatly depending on the irradiation site, dose, fractionation, and comorbidities. The overall incidence of radiation retinopathy has been reported to be 17% 4), meaning not all patients develop it. Radiation cataract poses a long-term risk even at low doses, so regular ophthalmic check-ups are important for those with a history of radiation exposure.
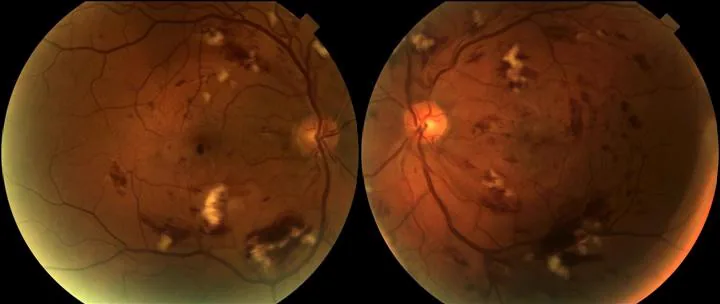
Gupta A, et al. Radiation Retinopathy: Case report and review. BMC Ophthalmol. 2007;7:6. Figure 2. PMCID: PMC1855313. License: CC BY 2.0.
Color fundus photographs of both eyes showing extensive retinal ischemic changes, retinal hemorrhages, cotton-wool spots, and hard exudates as early findings of radiation retinopathy. These correspond to the fundus findings of radiation retinopathy discussed in section “2. Main Symptoms and Clinical Findings.”
Radiation-induced lens opacities begin as polychromatic fine punctate opacities and vacuoles in the central posterior subcapsular area. These changes gradually enlarge, becoming plaque-like and granular opacities. At the same time, water clefts, which are dissections of the Y-shaped suture, may occur. As it progresses, a doughnut-shaped posterior subcapsular opacity with a relatively clear center appears. Further progression leads to a disc-shaped opacity consisting of two layers of membranous opacity (anterior and posterior), resulting in significant visual impairment.
Fundus findings resemble diabetic retinopathy, starting with microaneurysms, retinal hemorrhages, and hard exudates, followed by the appearance of cotton-wool spots. As it progresses, retinal neovascularization develops, leading to vitreous hemorrhage. Macular edema and occlusion of perifoveal capillaries cause vision loss. Once it develops, progression is faster than in diabetic retinopathy.
Radiation retinopathy is broadly classified into non-proliferative and proliferative types.
Non-proliferative RR
Microaneurysms: Scattered retinal capillary aneurysms. Important as an early finding.
Telangiectasia: Irregular vascular dilation and tortuosity. Clearly delineated on fluorescein angiography (FA).
Retinal hemorrhages: Scattered dot and flame-shaped hemorrhages.
Hard exudates: Yellow-white infiltrates due to lipid deposition.
Macular edema (ME): The finding most affecting visual prognosis. Appears as cystoid or diffuse edema on OCT.
Proliferative RR
Retinal neovascularization (NV): Abnormal vessels induced in ischemic areas. Cause of vitreous hemorrhage.
Neovascular glaucoma (NVG): Refractory glaucoma due to neovascular infiltration of the iris and angle. The enucleation rate due to NVG is reported to be 1–12% 5).
As a late-onset special finding, an onion ring sign (onion ring-like appearance) due to cholesterol crystals within cyst cavities has been confirmed on OCT in a case that developed 17 years later, and is attracting attention as a marker of treatment resistance in the chronic phase 6).
In a case where RR localized to the superior retina developed 16 months after 30 Gy whole-brain irradiation, the lesion distribution matched the 30 Gy isodose line of the radiation field, confirming that even at low doses, the onset pattern corresponds to the radiation field 7).
Onset ranges from 3 months to several years after irradiation, with progressive vision loss. The mechanism is ischemic optic neuropathy due to endothelial damage, and final visual acuity is no light perception in about half of cases, indicating a poor visual prognosis.
QWhen does radiation retinopathy typically develop?
A
Onset often occurs six months or more after irradiation, especially 2–3 years later. The median time to diagnosis has been reported as 39 months after irradiation3), but late-onset cases up to 17 years later also exist4). Long-term regular fundus examinations are necessary after irradiation.
In 2011, the ICRP (International Commission on Radiological Protection) revised the threshold and recommended that the total dose threshold for cataracts causing vision loss be 0.5 Gy or less for all exposure conditions. For occupational exposure, the limit for eye exposure was revised from 150 mSv per year to an average of 20 mSv over 5 years, with no single year exceeding 50 mSv.
The dose threshold is generally considered to be 35 Gy4). Irradiation exceeding 45 Gy increases the likelihood of onset, and exceeding 50 Gy particularly raises the risk3). However, late-onset radiation retinopathy has also been observed after stereotactic fractionated external beam irradiation of 20–40 Gy8), so caution is needed even at doses below the threshold.
Risk Factor
Details
Total Dose
>35 Gy (threshold)4), high risk above 45 Gy
Fraction Dose
High fractionated irradiation
Irradiation Site
Orbit or near optic chiasm3)
Diabetes
Exacerbates microvascular fragility
Combined chemotherapy
Increased sensitivity
Proliferative RR is reported to occur in 3–25% of all RR cases 5). Irradiation near the optic chiasm has been reported to show a significant correlation (p=0.009) with the development of RR 3).
A single dose of 2 Gy or less and a total dose of 50 Gy or less are considered relatively safe. Recently, Gamma Knife treatment has become mainstream, and the incidence of radiation optic neuropathy has been significantly reduced.
QDoes having diabetes increase the risk of radiation damage?
A
Diabetes is an important risk factor for radiation retinopathy. The microvascular fragility caused by diabetes acts synergistically with radiation-induced endothelial damage, potentially leading to disease onset even at lower doses. Along with maintaining blood sugar control, more frequent eye examinations are recommended after radiation therapy.
A detailed history of exposure (dose, type, timing) is important. Posterior subcapsular opacities are confirmed using a slit-lamp microscope. Low-dose radiation exposure should be considered to accelerate age-related changes in the lens. Since age-related cataracts also produce vacuoles, posterior subcapsular opacities, water clefts, and superficial cortical opacities, it is not easy to determine whether opacities in an aged lens are due to radiation exposure. Confirming the exposure history is key to differentiation.
FA is the basic examination for diagnosis and staging of RR. In the early stage, increased permeability of retinal capillaries is observed, and as the disease progresses, capillaries become occluded. Arterioles also become occluded, leading to extensive enlargement of retinal avascular areas and the development of retinal neovascularization. The Amoaku FA classification (Grade 1–4) is widely used 1).
OCT is used for quantitative assessment of ME according to the Horgan classification (Grade 1–5), and OCT detection is possible at 4 months after plaque brachytherapy1). OCTA can noninvasively visualize capillary dropout, nonperfusion areas, and changes in the FAZ, and is useful for early detection 1).
Visual acuity testing, visual field testing, and OCT evaluation of the optic nerve are performed. Optic disc atrophy and progression of visual field defects are followed over time.
Because the fundus findings resemble diabetic retinopathy, differential diagnosis is necessary. Confirming the history of radiation exposure generally makes differentiation easy.
Retinal vein occlusion: Mainly hemorrhage and edema along the occluded vein. Without a history of radiation exposure, differentiation is easy.
QWhat is the difference from diabetic retinopathy?
A
Fundus findings (microaneurysms, hemorrhages, exudates, neovascularization) are similar in both. The most important differentiating point is the presence or absence of radiation exposure history. Also, radiation retinopathy, once it develops, progresses faster than diabetic retinopathy, and its time course of half a year to several years after irradiation is characteristic. Management is particularly difficult when both diseases coexist.
In typical posterior subcapsular cataract, when the opacity diameter exceeds 2 mm, visual function declines and surgery becomes necessary. Cataract surgery can be expected to improve vision.
For prevention, protective glasses made of lead glass or lead acrylic are extremely useful for healthcare workers and those engaged in radiation work.
Anti-VEGF drugs are currently the first-line treatment for RR. The drugs used are bevacizumab (IVB), ranibizumab, and aflibercept1). Use of high-dose ranibizumab 2 mg has also been reported 1).
Prophylactic anti-VEGF administration is performed to suppress the onset of RR after radiotherapy. A meta-analysis of 4 studies involving 2109 patients showed the following results 2).
Poor vision (visual acuity equivalent to <20/200) reduced by 50% (OR 0.50)
The recommended protocol is IVB 1.25–1.5 mg administered every 4 months for 24 months 2). A report on prophylactic anti-VEGF administration over 48 months showed significant improvement in best-corrected visual acuity: 0.54 logMAR (prophylaxis group) vs. 2.00 logMAR (control group) 5). Note that intravitreal injection of VEGF inhibitors is not covered by insurance for radiation retinopathy.
In a meta-analysis of 4 studies involving 2109 patients by Victor et al. (2023), prophylactic IVB was confirmed to significantly reduce ME by 50% and RON by 38% after plaque brachytherapy2).
Laser photocoagulation
Laser photocoagulation is applied to avascular areas of the retina to prevent retinal neovascularization and neovascular glaucoma. Panretinal photocoagulation (PRP) is performed for proliferative RR, with a reported regression rate of 66% 5). Focal laser is used adjunctively for ME.
Topical steroid administration
Triamcinolone (TA), dexamethasone intravitreal implant (DEX), and fluocinolone acetonide (FA) are used as adjunctive therapy when anti-VEGF therapy is resistant 5). Intravitreal injection of triamcinolone is considered effective in transiently reducing macular edema and improving visual acuity, but it is not covered by insurance.
Management of proliferative RR
Vitrectomy is performed for vitreous hemorrhage. Vitrectomy is also indicated for tractional retinal detachment. NVG may require filtering surgery or cyclophotocoagulation. There is no effective way to stop progression, and the prognosis is often poor.
There is essentially no curative treatment. For early cases without optic atrophy, systemic steroids, anticoagulation therapy such as heparin, and hyperbaric oxygen therapy may be somewhat useful. Evidence for all of these is limited, and decisions must be made on a case-by-case basis.
QHow long should anti-VEGF injections be continued?
A
For prophylactic administration, a protocol of every 4 months for 24 months is recommended2). For therapeutic administration, the duration varies depending on disease activity. In treatment-resistant chronic cases, more than 72 injections may be required6).
The lens is a highly radiosensitive tissue. When lens epithelial cells in the germinal zone (equator), which have high proliferative capacity, are exposed to radiation, free radicals are produced intracellularly, causing DNA damage. This leads to structural changes in crystallin, a lens protein, and degeneration of epithelial cells and nucleated lens fibers, which migrate posteriorly and become displaced to the central posterior capsule, resulting in opacification. This is the cause of the characteristic opacity pattern clinically observed as posterior subcapsular cataract.
The central mechanism of radiation-induced retinal damage is selective loss of retinal vascular endothelial cells. Retinal vascular endothelial cells with high proliferative capacity are most susceptible, and choroidal vascular endothelium is also damaged. Endothelial cells are particularly sensitive to radiation, and capillary walls collapse due to DNA damage and apoptosis.
The progression of the pathology follows the following stages:
Endothelial cell injury stage: Progresses immediately after irradiation. DNA double-strand breaks and apoptosis of endothelial cells occur, leading to loss of vascular wall integrity.
Capillary occlusion and ischemia stage: Loss of endothelial cells leads to capillary occlusion and expansion of retinal ischemic areas. Early FA shows increased permeability, but as it progresses, occlusion becomes predominant. Arterioles also become occluded, and retinal avascular areas expand extensively.
VEGF production and neovascularization stage: VEGF is overproduced in ischemic retina, inducing proliferation of fragile new blood vessels.
Accumulation of advanced glycation end products (AGEs), pericyte loss, and basement membrane thickening are also thought to contribute to endothelial damage. This mechanism is similar to that of diabetic retinopathy and explains why the risk of radiation retinopathy increases in patients with diabetes. There is a latent period of at least six months, especially 2–3 years, from irradiation to clinical onset. This reflects the time required for endothelial cell damage to accumulate and capillary occlusion to become clinically apparent.
The main mechanism is ischemic optic neuropathy caused by damage to the vascular endothelium. After radiation therapy for sinus tumors or lesions at the base of the skull, the optic chiasm or the optic nerves before and after it undergo ischemic changes, leading to progressive vision loss.
7. Latest Research and Future Prospects (Investigational Reports)
The meta-analysis by Victor et al. (2023) is the largest current evidence showing the efficacy of prophylactic anti-VEGF administration, but most of the included studies are observational, and further validation through randomized controlled trials (RCTs) is needed 2). Standardization of optimal dosing intervals, agents, and treatment duration also remains a future challenge.
Early Detection Using OCTA (Optical Coherence Tomography Angiography)
OCTA can quantitatively assess capillary dropout, FAZ enlargement, and decreased capillary density without contrast agents. It can detect non-perfusion areas from early stages after radiation therapy, and its application for screening and monitoring of radiation retinopathy (RR) is advancing 1).
Kayabai et al. (2025) reported a case of a 53-year-old man 19 years after radiation therapy for intraocular tumor 6). The onion ring sign (multilayered deposition of cholesterol crystals within cyst cavities) observed on OCT is attracting attention as an imaging marker for chronic, treatment-resistant radiation retinopathy, and a long course requiring more than 72 intravitreal injections was documented.
The application of next-generation anti-VEGF agents such as brolucizumab and faricimab (angiopoietin/VEGF dual-target) for RR is being investigated 5). They are expected as alternative options in cases resistant to existing drugs.
Risk Assessment After Proton and Heavy Ion Therapy
In addition to conventional X-rays and gamma rays, risk assessment for radiation retinopathy after proton and heavy ion (carbon ion) therapy is being advanced. Even with highly dose-concentrated particle therapy, RR can occur if the retina is included in the radiation field, so retinal dose evaluation during treatment planning and post-treatment monitoring are challenges.
Combined Management with Radiation Optic Neuropathy (RON)
RR and radiation optic neuropathy (RON) may occur simultaneously from the same radiation field. The incidence of RON after EBRT is reported to be approximately 2% 3), and in cases where RR and RON coexist, visual dysfunction becomes more severe. Therefore, regular evaluation of the optic nerve using visual field testing and OCT in addition to fundus examination is an important research topic.
Sahoo NK, Ranjan R, Tyagi M, Agrawal H, Reddy S. Radiation Retinopathy: Detection and Management Strategies. Clin Ophthalmol. 2021;15:3797-3809. doi:10.2147/OPTH.S219268.
Victor AA, Andayani G, Djatikusumo A, Yudantha AR, Hutapea MM, Gunardi TH, Soetjoadi H. Efficacy of Prophylactic Anti-VEGF in Preventing Radiation Retinopathy: A Systematic Review and Meta-Analysis. Clin Ophthalmol. 2023;17:2997-3009. doi:10.2147/OPTH.S433531.
Kinaci-Tas B, Wilschut JA, Kilic E, et al. The incidence of radiation-induced optic neuropathy and retinopathy in patients treated with external beam radiation therapy: a systematic review and meta-analysis. Cancers. 2023;15:1999.
Chakraborty K, Jain S, Tripathy K, et al. Bilateral radiation retinopathy 17 years following radiotherapy for nasopharyngeal carcinoma: A diagnostic and therapeutic challenge during COVID-19 lockdown. Indian J Ophthalmol. 2023;71(1):303-305. doi:10.4103/ijo.IJO_1526_22.
Mularska W, Nowak-Gospodarowicz I, Golik B, et al. Radiation retinopathy after plaque brachytherapy for uveal melanoma—pathogenesis, diagnosis, and management. J Contemp Brachytherapy. 2023;15:372-382.
Kayabai M, Ilhan S, Celik E, et al. Onion ring sign as a biomarker of chronic treatment-resistant radiation retinopathy. Cureus. 2025;17(11):e97758.
Chan L, Eftekari SC, Nguyen QT, et al. Radiation retinopathy after whole-brain radiotherapy: a case report and literature review. Adv Radiat Oncol. 2021;6:100706.
Trikha R, Morse LS, Zawadzki RJ, et al. Ten-year follow-up of eyes treated with stereotactic fractionated external beam radiation for neovascular age-related macular degeneration. Retina. 2011;31(7):1303-1315. doi:10.1097/IAE.0b013e318203ee46.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.