“Low vision” refers to visual function or vision that causes some difficulty in growth, development, or daily and social life, and is interpreted as including blindness.
“Low vision care” is a general term for supportive actions that aim to solve problems in daily life, education, occupation, sports, cultural activities, etc., caused by visual impairment including blindness, using various methods.
“Rehabilitation” refers to restoring lost functions and abilities due to disability as much as possible to the original state, and enabling the person to return to social life as much as possible. Generally, this concept targets adults whose various functions have developed.
“Medical treatment and education” is defined as a regional network of medical care, education, welfare, and health services. Medical professionals such as doctors, nurses, orthoptists, clinical psychologists, and social workers collaborate closely with childcare, education, welfare, and health personnel to nurture the growth of visually impaired children.
The classification of visual impairment according to the WHO definition is as follows.
Blindness: Corrected visual acuity in the better eye less than 0.05 (or visual field within 10 degrees)
Low vision: Corrected visual acuity 0.05 or more but less than 0.3
The degree of visual impairment is divided into two categories based on its impact on daily life. Severe (visual acuity less than 0.02) is a condition where vision is almost unusable and is also called blindness. Mild (visual acuity 0.02 or more to less than 0.3) is a condition where vision can be used and corresponds to amblyopia in a narrow sense.
The estimated number of visually impaired children (under 18 years old) is about 20,000, and about 5,000 hold a physical disability certificate (survey by Nakae et al., 2006). According to a survey (reported in 2010) targeting students at national schools for the blind (15 years old or younger, 3,746 students), the causes of visual impairment were congenital anomalies 57.1% (most common), retinopathy of prematurity (oxygen toxicity) 17.6% (second), unknown 9.0%, systemic diseases 6.3%, and tumors 5.9%. Congenital anomalies include familial exudative vitreoretinopathy, microphthalmia, optic nerve hypoplasia, retinoschisis, and albinism. About 90% of childhood visual impairment develops before the age of one.
The Japan Ophthalmologists Association has organized the importance of life training, skill acquisition, and employment support in parallel with treatment, and positions low vision care as part of primary eye care 2). Smart Site is a framework of regional collaboration leaflets that introduce consultation services according to concerns, and is used as an entry point from ophthalmology to local support organizations 1).
QHow is low vision care different from rehabilitation?
A
Low vision care is a general term for support activities targeting all visually impaired individuals, including those who are blind, and is not limited by age. Rehabilitation is a concept aimed at restoring lost functions and social reintegration for adults. For children (especially 0–3 years old), the concept of “habilitation” is used, where medical, educational, welfare, and health services collaborate as a community network.
Symptoms of visual impairment vary greatly depending on the site of the lesion.
Central Visual Field Defect
Inability to return a smile: Cannot recognize facial expressions from the front.
Difficulty with eye contact: Gaze does not align with the position of the hands.
Lack of interest in letters: Shows behavior of not being interested in letters.
Facial orientation: Turns the face to the left or right to try to look straight ahead.
Peripheral visual field loss
Inattention to nearby objects: tripping, bumping into things.
Difficulty throwing a ball: can play soccer but is not good at throwing a ball.
Discomfort in dark places: behavior changes significantly with changes in brightness.
Photophobia (glare): sensitivity to light outdoors.
In adults with low vision, the main difficulties are reading, moving around, working, filling out documents, and obtaining information. The first step in consultation is to organize the types of difficulties, medical situation (disease name, visual acuity, visual field, whether progressive), possession of a disability certificate, and life situations.
QCan a person with relatively preserved visual acuity still be a candidate for low vision care?
A
Yes. According to the WHO definition, low vision is corrected visual acuity of 0.05 or more but less than 0.3, so even those with “some vision” are candidates. Also, cases with only visual field loss and relatively preserved visual acuity (e.g., end-stage glaucoma) are candidates for low vision care. Utilizing remaining visual function is the starting point of support.
Visual function is established through the input, integration, and output pathways, from the eye through the visual pathway to the occipital visual cortex. Visual development is generally complete by around age 8, with the most critical period being from 0 to 3 years. Appropriate habilitation during this period can promote visual development. For early-onset visual impairment, early intervention directly impacts prognosis.
Functional vision assessment, which observes the distance at which a person watches TV, the distance at which they can recognize family members, changes in behavior due to brightness, and the presence of photophobia outdoors, is important for determining the direction of daily living support.
MNREAD-J is a Japanese version of a reading efficiency assessment that measures three indicators: maximum reading speed, critical print size, and reading acuity. As a general standard, a reading speed of 200 characters per minute is considered a target for first-grade elementary school students. It can objectively evaluate the suitability of reading aids and the need for educational support.
In patients with macular dysfunction, a retinal area other than the fovea (PRL) is used for fixation. Identifying the PRL and performing fixation training using it can enhance the effectiveness of rehabilitation.
QWhat is MNREAD-J?
A
It is a Japanese version of a reading efficiency assessment that measures three things: maximum reading speed, critical print size, and reading acuity. For first-grade elementary school students, 200 characters per minute is one standard. It is used to objectively evaluate the suitability of prescribing magnifiers or video magnifiers and the need for educational accommodations.
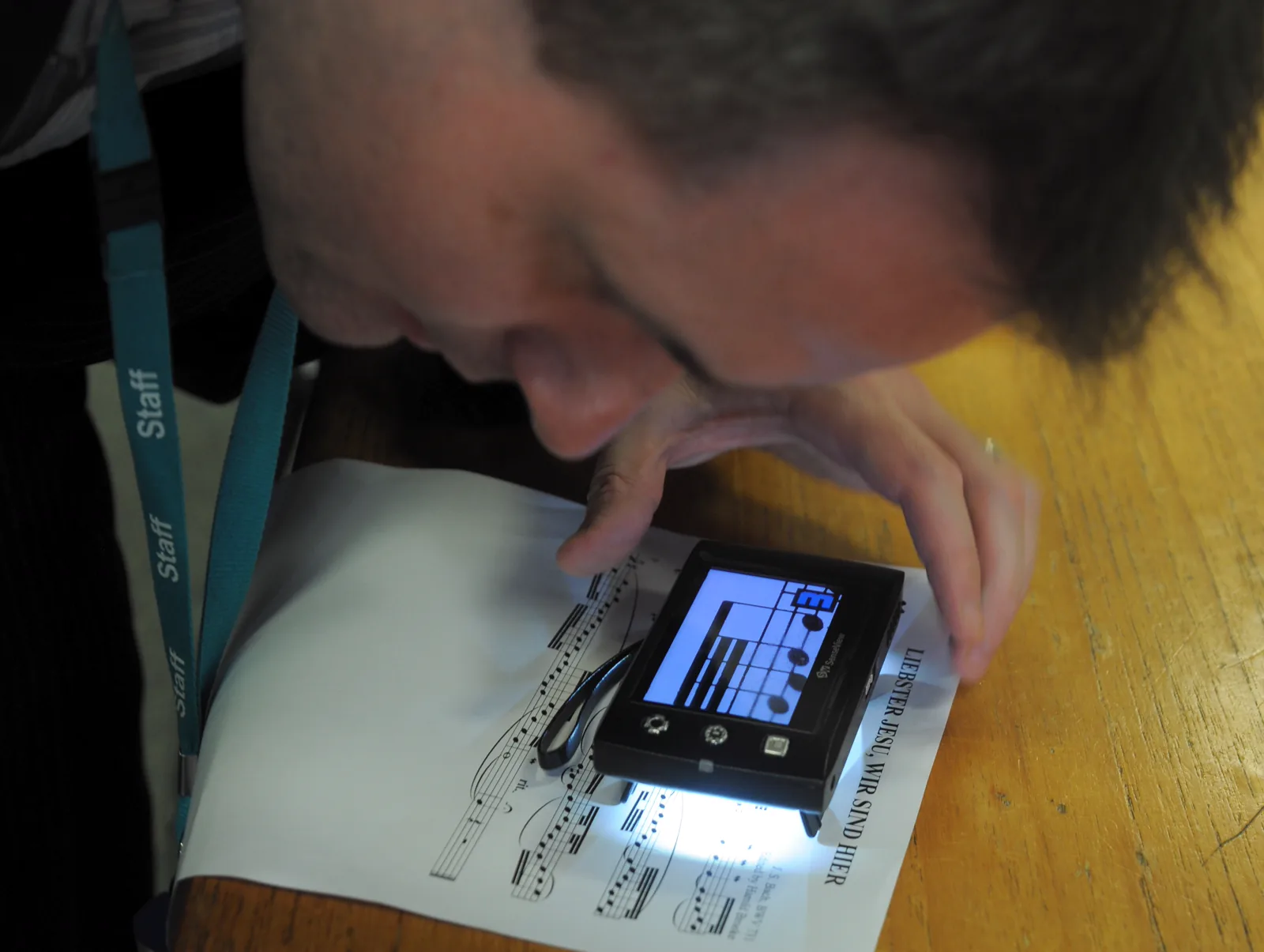
MuseScore. Small CCTV reader for low vision users. Wikimedia Commons. 2013. Source ID: File:Small_CCTV_reader_for_low_vision_users.jpg. License: CC BY 2.0.
A photo of a low-vision user placing a small CCTV video magnifier on sheet music to read, showing enlarged musical notes displayed on the monitor screen. This corresponds to the video magnifier discussed in the section “5. Visual aids and support systems.”
Desktop magnifier (loupe): Start with a low magnification of 3-4x. Use a book stand to avoid lowering the head. A magnifier with a light is useful.
Monocular telescope: A distance and intermediate vision aid. It can be used by elementary school students and older, with a magnification of usually 6–8×. An orthoptist provides detailed instruction on its use.
Video magnifier (CCTV): A device that uses a built-in camera to display a highly magnified image on a monitor. Types include near, distance, bifocal, desktop, and portable models. A color autofocus type is preferable, and a bifocal type is useful for viewing the blackboard at school.
Tinted glasses (filter lenses): These cut short-wavelength blue light (<500 nm), which is the main cause of glare. Unlike regular sunglasses, they do not significantly reduce the amount of light entering the eye, so the sensation of brightness is less affected. They are indicated for photophobia due to albinism, congenital aniridia, corneal diseases, and intraocular diseases. Two types are provided: outdoor and indoor. The prescription opinion must include three items: “photophobia is present,” “the lenses are effective,” and “no other treatment is prioritized.”
Tablet device (e.g., iPad): Can be used with voice apps, magnification functions, and as an electronic textbook. The voiceover function on smartphones (e.g., VoiceOver) is also useful.
Assistive device provision system and daily living aids
Assistive devices are provided by municipalities as a support for independence (user cost: generally 10%). Daily living aids are determined by the municipality, so items and amounts vary by local government5).
The main items and standard amounts are shown below.
Information/communication support devices (PC, etc.)
100,000 yen
5 years
Print document reading device for visually impaired
99,800 yen
6 years
According to Yokohama City’s guidance, daily living aids generally require a 10% copayment and prior application, and a video magnifier is listed as an example of information and communication support aids 5).
In Yokohama City, all 18 municipal libraries lend audio and braille materials and provide face-to-face reading services, and the Central Library also offers online face-to-face reading 4). At the Osaka City Hayakawa Welfare Hall Braille Library, braille books and audio books are produced and lent, face-to-face reading is provided, and materials can be ordered from nationwide braille libraries, with free round-trip postage via fourth-class mail 6). The Ministry of Health, Labour and Welfare’s reading support photo report also introduces the Daisy Network (Sapie) at braille libraries nationwide 3).
QHow can I receive assistive device benefits?
A
First, obtaining a physical disability certificate is a prerequisite. Then, apply for assistive device cost benefits at the welfare counter of your municipality. Attach a prescription opinion from an ophthalmologist (for tinted glasses, three items must be described). The user copayment is generally 10%, and there are reduction measures for low-income individuals. Prior application before purchase is required; applications after purchase may not be accepted 5).
There are four levels of school placement depending on the degree of visual impairment.
Placement
Criteria
Special Needs School (Visual Impairment)
Students with corrected binocular visual acuity less than 0.3, or with severe visual impairment unable to recognize visual information even with magnifiers.
Special Support Classroom for Low Vision (Low Vision Class)
Students who have difficulty recognizing standard characters and figures even with magnifiers.
Itinerant Instruction Classroom for Low Vision
Students with visual impairment similar to those in low vision classes but who can generally participate in regular class learning.
Regular Class
Students who can be accommodated with individual adjustments based on their actual visual condition.
Free provision of enlarged textbooks has been established through a 2010 law amendment. The choice of school placement is made collaboratively by parents, ophthalmologists, the board of education, and the special needs education coordinator.
Early Infancy (0–3 years): The most critical period for habilitation and early intervention. Focus is on visual function assessment (ERG, VEP) and guidance for parents.
Late infancy (3–7 years): This is the period when the use of assistive devices becomes possible. Issues regarding preschool and school selection arise. Eye-use training (coloring, mazes, block play, etc.) is also important.
School age (7–12 years): Formal instruction in visual assistive devices is provided. The focus is on solving school-related problems and arranging the learning environment.
Student age (12–18 years): Counseling on schooling, higher education, and employment, as well as vocational training, become key issues.
The procedure for utilizing support systems for children and adults with visual impairments is as follows.
Obtaining a disability certificate (at the municipal office)
Financial support (medical): Medical assistance for persons with disabilities, medical care for independent living, and medical care for development
Financial support (income security): Employees’ Pension Insurance, etc.
Provision and loan of welfare equipment (subsidy for assistive devices, provision of daily living aids)
Daily living support
Use of facilities and schools
Vocational training and employment support
The employment rate for visually impaired individuals is 22.9% (Ministry of Health, Labour and Welfare, 2006), and by occupation, the largest proportion (29.6%) are engaged in the three therapies (anma, massage, acupressure, acupuncture, and moxibustion).
QWhat school can a child with low vision attend?
A
There are four levels of options depending on the degree of visual impairment and the individual’s situation. For those with corrected binocular visual acuity less than 0.3, special support schools (for visual impairment) are an option. If recognition of normal print is difficult even with magnifiers, a special support classroom for low vision (low vision class) is available. If the child can generally participate in regular classes, a low vision resource room (itinerant instruction) is used. If individual accommodations suffice, the child attends regular classes. The school placement is decided collaboratively by parents, ophthalmologists, and the board of education.
The Japan Ophthalmologists Association established a Low Vision Network Study Group in 2011, and by 2021, the creation of Smart Site leaflets was completed in all 47 prefectures 2). These are now also used for welfare collaboration across prefectural borders.
The Japan Ophthalmologists Association positions low vision care as part of primary eye care and promotes the dissemination of “Quick Low Vision Care” that all ophthalmologists can provide in daily practice 2).
The use of AI voice reading and smartphone apps (such as VoiceOver) is expanding, and the use of electronic textbooks combined with tablet devices is also becoming more widespread.
Systematization of specialized vision rehabilitation techniques, such as eccentric viewing training (PRL training) and visual attention training, is progressing.
Since April 2024, the Act for Eliminating Discrimination against Persons with Disabilities has mandated reasonable accommodation provision for private businesses as well. Interest in low vision support in the workplace is increasing.