Visual evoked potential (VEP) is a test that records the response of the visual cortex to visual stimuli using electrodes placed on the scalp. It is performed to objectively evaluate the presence of visual pathway disorders and visual functions such as visual acuity.
The visual cortex is primarily activated by the central visual field, and the occipital lobe has a large projection area for the macula. VEP depends on the integrity of the entire visual pathway including the eye, optic nerve, optic chiasm, optic tract, optic radiation, and cerebral cortex, and reflects photopic visual function from the macular cones to the visual cortex.
As electrophysiological tests, the three main tests in ophthalmology are electroretinography (ERG), VEP, and electrooculography (EOG). VEP has unique value in detecting functional disorders of the upper visual pathway that cannot be detected by ERG, and in evaluating visual function in cases where subjective testing is difficult.
The International Society for Clinical Electrophysiology of Vision (ISCEV) revised and published a standard protocol in 2016, and it is recommended to record according to this protocol to eliminate inter-institutional differences 4).
The main indications for VEP are the following five points.
To investigate the presence of visual pathway disorders (especially optic nerve disorders)
Evaluation of visual function in cases where visual acuity testing is not possible, such as in infants and young children
Diagnosis of psychogenic visual disturbance and malingering
When the fundus cannot be visualized due to opacity of the ocular media
Evaluation of unexplained visual loss
QIn which patients is VEP particularly useful?
A
VEP is useful when objective evaluation of visual function is needed. Main indications include cases where cooperation for visual acuity testing is difficult (e.g., infants), cases where the fundus cannot be visualized due to cataract or vitreous hemorrhage, suspected psychogenic visual disturbance or malingering, detailed examination of optic nerve diseases, and unexplained visual loss.
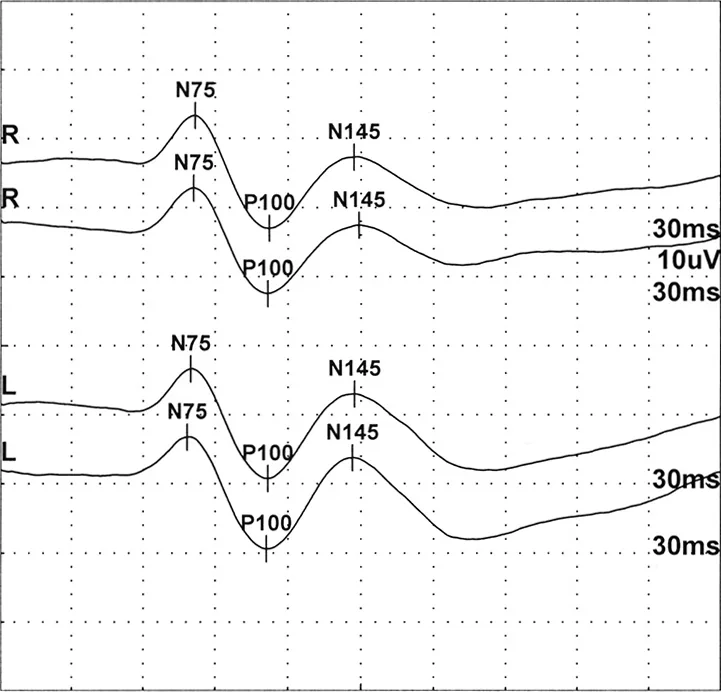
Medicus of Borg. VEP-normal.gif. Wikimedia Commons. 2015. Source ID: commons.wikimedia.org/wiki/File:VEP-normal.gif. License: CC BY-SA 4.0.
Representative pattern reversal VEP waveforms from the right and left eyes of a healthy adult. The negative component N75, positive component P100, and negative component N145 are labeled with their peak latencies (ms) and amplitudes (10 µV). This corresponds to the identification and normal value evaluation of the P100 component discussed in the section “2. Types of VEP and Main Findings.”
VEP waveforms vary depending on the stimulation method. Selection is based on whether the fundus can be visualized and the visual acuity.
Pattern Reversal VEP (PVEP)
Stimulation method: Pattern stimulation using reversal of a black-and-white checkerboard.
Waveform components: Three components: N75 (75 ms), P100 (100 ms), and N135 (135 ms).
Normal P100 latency: Approximately 90–120 ms (varies with age). High reliability with little inter-individual variation.
Amplitude measurement: Measured as the potential difference from the N75 peak to the P100 peak.
Indications: Cases where the fundus is visible. Highest sensitivity for diagnosing optic neuritis. Refractive correction is essential.
Flash VEP (FVEP)
Stimulation method: Stimulation using only light flashes.
Waveform configuration: Evaluated with N70 (approximately 70 ms) and P100 (approximately 100 ms). Due to large individual differences, evaluation is based on interocular differences.
Normal P100 latency: Approximately 90–120 ms (varies with age).
Amplitude in children: About 1.5–2.0 times that of adults. Becomes nearly equivalent to adults by 7–8 years of age.
Indications: (1) Cases where the fundus is not visible, such as cataract or vitreous hemorrhage; (2) Cases with severely reduced visual function where pattern stimulation yields no response; (3) Cases with difficulty in fixation, such as newborns.
Pattern VEP is broadly divided into transient VEP (t-VEP) and steady-state VEP (s-VEP). When the stimulation frequency is approximately 2 Hz or less, it is called t-VEP; at 4 Hz or more (steady state), it is called s-VEP. t-VEP can evaluate spatial frequency characteristics by changing the check size, and because it correlates with visual acuity, it is widely used for objective visual acuity estimation. s-VEP can be measured in a short time, but it provides only amplitude information, making evaluation of latency prolongation difficult.
Abnormal VEP findings are broadly classified into three types.
Non-recordable VEP (absent/flat type): Seen in the acute phase of optic neuritis or in optic nerve diseases with extremely reduced visual acuity (0.1 or less). Waveform absence is also observed in severe optic neuropathy or after enucleation.
Prolongation of P100 peak latency: Extreme latency prolongation is seen in demyelinating diseases such as multiple sclerosis, with high diagnostic value. It also prolongs in other optic nerve disorders such as optic neuritis. Prolongation also occurs in severe visual acuity loss (0.1 or less) due to macular disorders, but not as much as in optic neuritis.
Amplitude reduction: Seen in optic atrophy and high myopia. Due to large individual differences and age effects, evaluation of the affected eye/healthy eye ratio is useful in unilateral diseases. s-VEP has high sensitivity and shows interocular differences in unilateral optic nerve disorders or macular diseases.
QWhat diseases cause prolongation of P100 latency?
A
Prolongation of P100 latency is most prominent in demyelinating diseases such as multiple sclerosis and is highly valuable as a diagnostic aid. It also prolongs in optic neuritis and other optic nerve disorders. Severe visual loss due to macular disease (visual acuity 0.1 or less) also shows latency prolongation, but not as extreme as in optic neuritis. For details, see the section “Diagnosis and Testing Methods”.
Pattern VEP may also show abnormalities in macular disorders. By combining with ERG, the presence or absence of macular dysfunction can be confirmed, and the lesion site can be estimated.
Standard preparation items for VEP recording are shown below.
Patient Preparation
Pattern VEP is tested with glasses correction (refractive correction required).
Flash VEP should ideally be tested with dilated pupils to ensure uniform stimulation. Also dilate pupils when recording simultaneously with ERG.
Monocular recording (completely shield the non-test eye from light).
Perform in a comfortable, relaxed posture.
Electrode placement (based on the International 10-20 system)
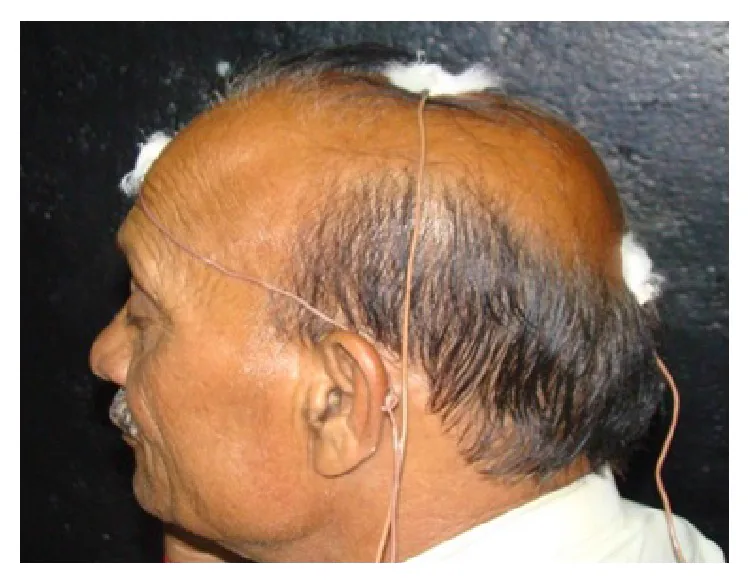
Shandilya M, Agrawal R. A Comprehensive Review on Methodologies Employed for Visual Evoked Potentials. Scientifica (Cairo). 2016;2016:9852194. Figure 3. PMCID: PMC4789528. License: CC BY.
Side view of a subject with EEG disc electrodes attached to the occipital region, earlobes, and forehead, showing the placement of active, reference, and ground electrodes based on the International 10-20 system. Corresponds to the electrode placement (International 10-20 system) discussed in the section “4. Diagnosis and Examination Methods”.
Place the active electrode at a point 5-15% of the distance from the inion to the nasion above the inion.
Attach the reference electrode and ground electrode to both earlobes.
Use EEG disc electrodes (silver chloride or gold electrodes) approximately 8 mm in diameter, and fix them with dedicated paste.
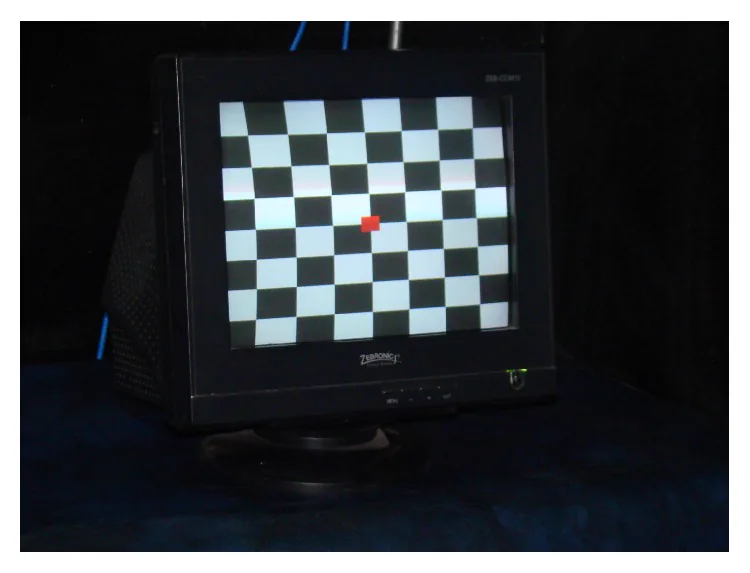
Shandilya M, Agrawal R. A Comprehensive Review on Methodologies Employed for Visual Evoked Potentials. Scientifica (Cairo). 2016;2016:9852194. Figure 2. PMCID: PMC4789528. License: CC BY.
Photograph of a pattern reversal VEP stimulus monitor displaying a black-and-white checkerboard pattern, with a red fixation point at the center and uniform check grid. Corresponds to the ISCEV standard pattern reversal stimulus settings discussed in the section “4. Diagnosis and Examination Methods”.
The three types of stimulation methods defined by ISCEV are as follows4).
Recording conditions: The amplification factor of the biological amplifier is 20,000 to 50,000 times, the bandpass filter has a high pass filter (low cut) of 1 Hz or less, and a low pass filter (high cut) of 100 Hz or more. The number of averaging is about 64 to 128 times. The analysis time is 250 ms or more, with a pre-trigger time of about 20 to 50 ms.
Evaluation of the chiasm and post-chiasmal pathways using half-field stimulation
In patients complaining of monocular visual loss, VEP can be measured; if results are normal and symmetric, non-organic visual impairment can be diagnosed.
For differentiating psychogenic visual disturbance, pattern-reversal VEP should be recorded regardless of visual acuity level. Typically, amplitude and latency are normal without interocular difference, but psychogenic patients may show better results than normal subjects because they cooperate and gaze at the stimulus intently. In suspected malingering, it is important to confirm fixation, and pattern onset/offset VEP is particularly useful.
Recordings should be performed with attention to the following four points:
Noise reduction: If noise is excessive, check electrodes and ground.
Prevention of EMG contamination: Excessive tension or stiff shoulders can cause EMG contamination. Have the patient relax during the test.
Prevention of alpha wave contamination: Drowsiness leads to alpha wave contamination. Ask the patient to come in good physical condition.
Fixation check: Ensure that the patient is correctly fixating on the stimulus screen while monitoring their behavior.
QWhat are the precautions when performing VEP in infants?
A
In infants with excessive movement, sedatives may be used, but better VEP waveforms are obtained when the infant is awake. Sedatives such as chloral hydrate suppositories (30–50 mg/kg) or triclofos sodium solution (0.8–1.0 mL/kg) are used. Recordings under sleep require interpretation considering sleep depth because sleep EEG may contaminate the VEP. Barbiturates such as phenobarbital are said to stabilize VEP waveforms, but caution is needed due to the risk of respiratory depression.
5. Clinical applications and use in treatment monitoring
When there is opacity of the ocular media such as cataracts, flash VEP can be used before surgery to estimate the function of the posterior pole and optic nerve, helping to predict postoperative visual prognosis. Abnormal flash VEP suggests the presence of visual pathway damage and serves as a reference for predicting poor postoperative visual acuity.
By performing VEP monitoring during surgery for skull base tumors or pituitary tumors, real-time detection of damage to the visual pathway and modification of the surgical approach become possible.
Conventional flash VEP intraoperative monitoring has been problematic due to instability and poor reproducibility under general anesthesia.
Foo et al. (2025) reported a case of skull base meningioma surgery in which, although flash (on-response) VEP showed no intraoperative changes, off-response VEP showed a 40% amplitude increase (from 2.8 V to 4.0 V) after resection of the tumor around the optic nerve, and postoperative visual acuity in the right eye improved markedly from 0.1 to 0.5 (Landolt C) 1). Off-response VEP independently records the potential generated at the end of light stimulation, providing more stable waveforms than conventional flash VEP and may have higher sensitivity for detecting visual function improvement.
Electrophysiological testing is particularly important in children because subjective functional tests such as visual acuity and visual field are less reliable, and VEP as an objective test becomes more significant.
The main indications for VEP in children are as follows:
Objective visual acuity estimation in infants: Sweep VEP uses pattern stimulation with gradually changing spatial frequencies to quantitatively evaluate visual thresholds, and is expected to be a more objective visual acuity measurement method than flash VEP.
Assessment of binocular vision and fusion development: VEP studies have shown that binocular vision exists by 2 months of age, and fusion begins by 3 to 5 months of age.
Evaluation of amblyopia: Assessed by VEP latency and amplitude. Pattern VEP (pVEP) is useful as an indicator of suprathreshold visual processing in amblyopic eyes. Prolonged P100 latency reflects slower visual information processing speed in amblyopic eyes.
In a series report of three cases of strabismic amblyopia by Blavakis et al. (2023), pVEP was evaluated before and after 20 hours (2–4 times per week) of dichoptic game training using a virtual reality (VR) system 2). In all three cases, P100 latency in the amblyopic eye improved (e.g., from 145 ms to 136 ms with 10 arcmin stimulus in case 1, and from 147 ms to 139 ms in case 2), and stereopsis also markedly improved (e.g., from 100 arcsec to 50 arcsec in case 1). It was suggested that improvement in visual processing speed assessed by VEP may precede visual acuity improvement.
Definitive diagnosis of psychogenic visual disturbance
In patients complaining of monocular visual loss, VEP measurement yielding normal and symmetric results can diagnose non-organic visual disturbance. In multiple sclerosis, VEP is also valuable as a diagnostic aid for detecting asymptomatic optic neuritis, with prolonged P100 latency being a key diagnostic finding.
6. Pathophysiology and theoretical background of visual pathway evaluation
VEP records potentials evoked in the primary visual cortex (V1) of the occipital lobe in response to visual stimuli. The P100 component is recognized as an electrical correlate of primary visual cortex activity.
The outline of signal transmission along the visual pathway is as follows:
Photoreception in the retina (cone cells)
Signal transmission from retinal ganglion cells to the optic nerve
Optic chiasm (crossing of nasal fibers)
Synaptic relay in the lateral geniculate nucleus (thalamus)
Via the optic radiation to the primary visual cortex (V1) in the occipital lobe
Pattern VEP reflects foveal function more strongly than flash VEP and is suitable for evaluating central visual acuity. Flash VEP assesses the entire visual pathway from the retinal ganglion cell layer to the visual cortex, but shows large individual variability.
Mechanisms of VEP abnormalities in demyelinating diseases
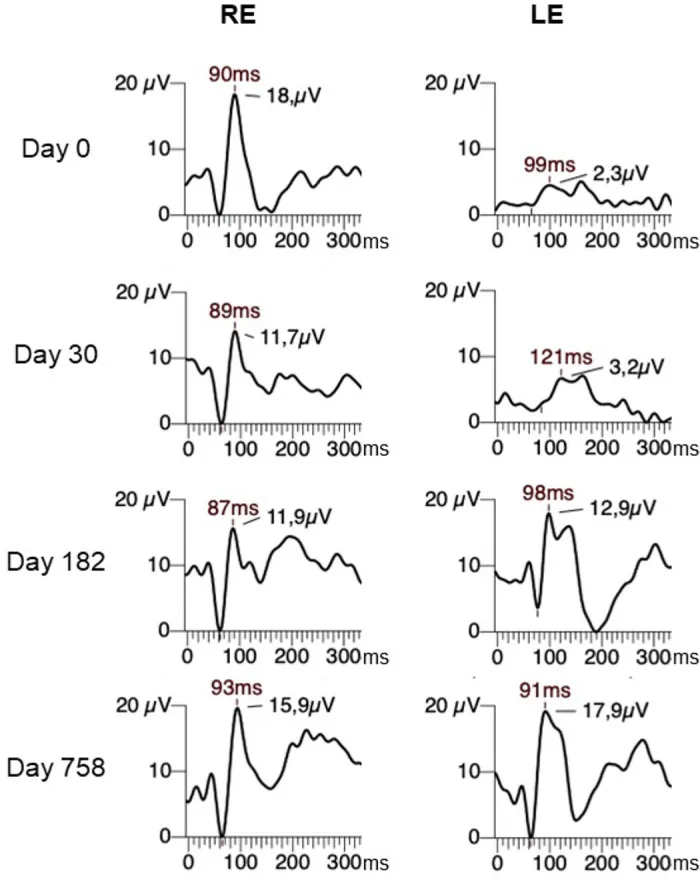
Alam MdM, Kasowski H, Cossette-Harvey M, et al. Simulating the Effects of Partial Neural Conduction Delays in the Visual Evoked Potential. Transl Vis Sci Technol. 2024;13(2):18. Figure 1. PMCID: PMC10896232. License: CC BY 4.0.
Pattern VEP follow-up waveforms of the right eye (RE, normal) and left eye (LE, affected eye) of a patient with optic neuritis at days 0, 30, 182, and 758 after onset, showing prolongation of P100 latency to 121 ms at day 30 and recovery to 91 ms at day 758. This corresponds to the mechanism of P100 latency prolongation in demyelinating diseases discussed in section “6. Pathophysiology and theoretical background of visual pathway evaluation”.
In multiple sclerosis, demyelination damages the myelin sheath, reducing nerve axon conduction velocity and significantly prolonging P100 latency. Even after demyelination improves, latency prolongation may persist for a long time, making it highly valuable as a diagnostic aid for detecting traces of asymptomatic optic neuritis.
Amplitude reduction often reflects loss of nerve axons themselves (axonal damage). When only latency prolongation is present, relatively good recovery is expected, whereas when accompanied by amplitude reduction, the prognosis tends to be poor.
In pediatric cortical visual impairment (CVI), flash VEP and pattern VEP have been applied for diagnosis and prognostic evaluation. However, there are limitations in interpreting VEP in children with CVI, and reports on the diagnostic usefulness of VEP are conflicting.
Clark et al. (44 infants) reported that 85% (11 of 13) of infants with normal flash VEP responses experienced significant visual improvement, compared to only 55% (17 of 31) in the abnormal VEP group3). On the other hand, some reports indicate that normal flash VEP responses do not correlate with visual outcomes, and differences in VEP paradigms (flash vs. pattern), subject age, follow-up period, and definition of visual improvement are thought to contribute to the discrepancies in results3).
Sweep VEP uses pattern stimuli with gradually changing spatial frequencies to quantitatively assess visual thresholds and is expected to be a more objective visual acuity measurement method than flash VEP. Studies in children with CVI have confirmed the reliability and validity of sweep VEP grating acuity compared to clinical visual acuity assessment3). However, difficulties in electrode placement due to structural brain abnormalities and the effects of epileptic seizures and antiepileptic drugs are cited as limitations in interpretation3).
Multifocal VEP: Using equipment similar to multifocal electroretinography, it is expected as an objective visual field testing method to detect visual pathway disorders above the retina. Its application for objective assessment of visual field defects in glaucoma is being investigated, but because the response to macular stimulation is large and peripheral responses are small, there are still challenges for widespread use as a general clinical test.
Event-related potential (ERP): Electrodes are placed on the vertex, and the P300 component appearing around 300 ms is evaluated. It is related to information processing and cognitive activity, and in ophthalmology, it is applied to diagnosis and pathophysiological elucidation in some cases of psychogenic visual disturbance.
7. Latest Research and Future Prospects (Research Stage Reports)
There is a single case report where off-response VEP detected improvement in visual function with high sensitivity even when conventional flash VEP (on-response) failed to capture intraoperative changes 1). This method records on-response and off-response separately by extending the duration of light stimulation, and is expected to yield more stable waveforms and improved sensitivity. Currently, it remains a single case report, and the minimum threshold for significant VEP amplitude increase is not yet determined, so further accumulation of multi-center data is necessary 1).
Refinement of objective visual acuity measurement using sweep VEP
Sweep VEP continues to be studied as an objective visual acuity measurement method for difficult-to-evaluate cases, including children with CVI. Sweep VEP grating acuity has lower detection sensitivity than vernier acuity but is consistently higher than behavioral visual acuity (FPL method) 3). Future expansion of application to pediatric diseases other than CVI is expected.
Dichoptic training and effect monitoring using VEP
pVEP is used to evaluate the effects of dichoptic game training using VR headsets. It has been suggested that improvement in visual processing speed (P100 latency) assessed by pVEP may precede visual acuity improvement 2), and future large-scale randomized controlled trials are expected to verify this. Recurrence of amblyopia occurs in up to 25% of cases within one year after treatment discontinuation, and the relationship between VEP changes during long-term follow-up and recurrence remains a challenge 2).
Development of portable VEP devices and AI analysis
In recent years, development of portable VEP devices that enable bedside or home measurement has progressed. In addition, AI-based automatic VEP waveform analysis is also at the research stage, and is expected to reduce inter-rater variability and improve examination accuracy.
Foo MX, Hardian RF, Kanaya K, Abe D, Kitamura S, Sato Y, et al. Postoperative Improvement of Visual Function Following Amplitude Increase in Intraoperative Off-Response Visual Evoked Potential (VEP) Monitoring During a Skull Base Meningioma Surgery. Cureus. 2025;17(4):e82563. doi:10.7759/cureus.82563. PMID:40390717; PMCID:PMC12088698.
Blavakis E, Spaho J, Chatzea M, Gleni A, Plainis S. Dichoptic Game Training in Strabismic Amblyopia Improves the Visual Evoked Response. Cureus. 2023;15(9):e45395. doi:10.7759/cureus.45395. PMID:37854740; PMCID:PMC10579841.
Chang MY, Borchert MS. Advances in the evaluation and management of cortical/cerebral visual impairment in children. Survey of ophthalmology. 2020;65(6):708-724. doi:10.1016/j.survophthal.2020.03.001. PMID:32199940.
Odom JV, Bach M, Brigell M, et al. ISCEV standard for clinical visual evoked potentials: (2016 update). Doc Ophthalmol. 2016;133(1):1-9.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.