
Arcus Senilis
Key Points at a Glance
Section titled “Key Points at a Glance”1. What is arcus senilis?
Section titled “1. What is arcus senilis?”Arcus senilis is also called gerontoxon, arcus lipoides, or arcus corneae. It is an annular opacity caused by lipid deposition in the peripheral corneal stroma and is the most common finding among peripheral corneal opacities.
It is classified as age-related fatty degeneration of the cornea. A large epidemiological study of an Asian population reported corneal arcus in 73.2% of 3,260 individuals aged 40–80 years1). In Japan, it is generally observed in over 70% of people aged 60 years and older, and in nearly all individuals aged 80 years and older.
When similar findings appear in young individuals under 40, it is called arcus juvenilis. Arcus juvenilis is more strongly associated with dyslipidemia, and further evaluation for familial hypercholesterolemia (FH) is recommended2). The main components of the deposits are cholesterol and phospholipids, originating from leakage from limbal vessels.
Arcus senilis develops in the peripheral cornea and does not involve the visual axis, so it does not cause vision impairment. Treatment is also unnecessary. However, prominent arcus senilis may reduce visibility of the surgical field during cataract surgery.
2. Main Symptoms and Clinical Findings
Section titled “2. Main Symptoms and Clinical Findings”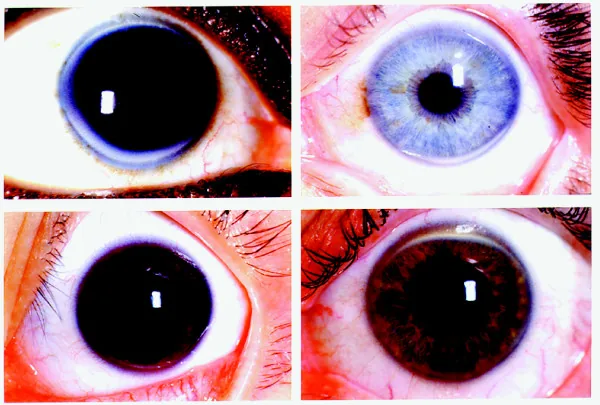
Subjective Symptoms
Section titled “Subjective Symptoms”Arcus senilis is usually asymptomatic and is often discovered incidentally during eye examinations. Rarely, family members or people around the patient may notice a white ring at the periphery of the cornea.
Clinical Findings (Findings Confirmed by the Physician)
Section titled “Clinical Findings (Findings Confirmed by the Physician)”The following findings are confirmed by slit-lamp microscopy.
- Annular opacity: A band-shaped opacity about 1 mm wide, matte white to yellowish-white, forming near the corneal limbus.
- Progression pattern: Begins in the inferior cornea, extends superiorly, and progresses circumferentially to become annular. The vertical width tends to be greater than the horizontal width.
- Clear zone (lucid interval): A clear zone remains between the corneal limbus and the arcus senilis. The peripheral border is distinct, but the central border is diffuse and indistinct.
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”The main cause of arcus senilis is age-related increased permeability of the limbal vessels, leading to leakage and deposition of low-density lipoprotein (LDL) in the corneal stroma.
The main risk factors are listed below.
- Age: The most important factor.
- Male sex: Tends to appear earlier than in females.
- Hyperlipidemia / Dyslipidemia: Associated with elevated serum triglycerides, total cholesterol, and LDL.
- Familial hypercholesterolemia (FH): According to FH clinical practice guidelines, a corneal arcus appearing before age 45, like tendon xanthomas, is a finding strongly suggestive of heterozygous FH 2). May be accompanied by xanthelasma palpebrarum.
- Smoking and systolic hypertension: Risk factors related to arteriosclerosis.
- Systemic lipid metabolism disorders: LCAT deficiency, fish eye disease, Tangier disease, and others can also be causes.
Association with Cardiovascular Disease
Section titled “Association with Cardiovascular Disease”Study results are inconsistent regarding the association between arcus senilis and cardiovascular disease (CVD).
In the Singapore Indian Eye Study (3,397 participants, ages 40–80), corneal arcus was independently associated with CVD even after adjusting for other risk factors 3). Even in the low-risk group (low Framingham score), the presence of corneal arcus was associated with increased CVD prevalence.
In the Singapore Malay Eye Study (3,280 participants), male sex, older age, BMI, CRP, total cholesterol, LDL, peripheral artery disease, chronic kidney disease, and current smoking were associated with corneal arcus 1).
In the prospective cohort of the Copenhagen City Heart Study (12,745 participants, mean 22-year follow-up, up to 33 years), xanthelasma independently predicted ischemic heart disease, myocardial infarction, and death, but corneal arcus had no value as an independent predictor 4).
Analysis of Framingham Heart Study data also reported that corneal arcus is not an independent predictor of CVD or CHD 5).
In the Lipid Research Clinics mortality follow-up study, arcus cornealis was associated with CVD mortality only in hyperlipidemic men aged 30–49 years (CHD mortality RR 3.7, CVD mortality RR 4.0) 6).
In a prospective study of Asian populations (median follow-up 10.8 years), arcus cornealis was not an independent predictor of CVD incidence after adjustment for traditional risk factors 7).
If arcus senilis (juvenile arcus) appears in a person under 40 years of age, evaluation for dyslipidemia including familial hypercholesterolemia is recommended. It is important to perform a fasting lipid profile and, if abnormalities are found, to proceed with medical evaluation and treatment.
4. Diagnosis and Differential Diagnosis
Section titled “4. Diagnosis and Differential Diagnosis”Diagnosis
Section titled “Diagnosis”Arcus senilis is a clinical diagnosis confirmed by slit-lamp examination. Imaging or pathological examination is not required.
Consider additional testing in the following cases:
- Arcus in young individuals (under 40 years): Fasting lipid profile (cholesterol, LDL, triglycerides), measurement of lipoprotein(a). Screening for familial hypercholesterolemia.
- Unilateral arcus senilis: Evaluation for carotid artery disease (e.g., carotid ultrasound).
Differential Diagnosis
Section titled “Differential Diagnosis”- Pseudogerontoxon: A superficial scar band adjacent to the corneal limbus associated with recurrent limbal disease. It may be seen in cases with a history of superior limbic keratoconjunctivitis.
- Terrien marginal degeneration: Presents with fine yellow-white stromal opacities, but differs in that it is accompanied by progressive corneal thinning.
- Schnyder corneal dystrophy: Presents with arcus-like limbal opacities from around age 20. It may also be accompanied by crystalline opacities in the central cornea.
Arcus senilis is an age-related change caused by lipid leakage from limbal vessels and is not accompanied by corneal neovascularization. In contrast, lipid keratopathy occurs secondary to corneal neovascularization, caused by lipid leakage from new blood vessels. Both share the common feature of lipid deposition, but their pathogenesis and clinical significance differ.
5. Pathophysiology
Section titled “5. Pathophysiology”With aging, the permeability of limbal vessels increases, causing LDL to leak and accumulate in the peripheral corneal stroma. Deposits mainly concentrate in two layers—Descemet’s membrane and Bowman’s layer—with more on the Descemet’s membrane side.
Histologically, it has the following characteristics.
- No increase in cell count or fragmentation of lamellae is observed.
- No phagocytosis or abnormal angiogenesis is observed.
- Tissue necrosis or atrophy does not occur.
Lipid deposition is not limited to the cornea; it may also be observed in the ciliary body, ciliary processes, and iris.
Unilateral arcus senilis is known as a phenomenon in which contralateral carotid artery stenosis reduces blood flow to the affected side, causing arcus senilis to appear only in the contralateral eye. Associations with ocular hypotension and cranial autonomic dysregulation have also been reported.
6. Management and Prognosis
Section titled “6. Management and Prognosis”No specific ophthalmic treatment is needed for arcus senilis. Since it does not cause visual impairment, routine follow-up during regular eye examinations is sufficient.
In cases of arcus juvenilis, medical treatment of the underlying dyslipidemia is important as systemic management, but no treatment is performed for the corneal finding itself. In patients with FH, a correlation between corneal arcus severity and coronary artery plaque burden has been reported, and systemic evaluation including family history, tendon xanthomas, and cholesterol levels is essential8).
The prognosis is excellent, and it does not affect vision or ocular health.
7. References
Section titled “7. References”- Wu R, Wang JJ, Tai ES, Wong TY. Cardiovascular risk factors, inflammation, and corneal arcus: the singapore malay eye study. American journal of ophthalmology. 2010;150(4):581-587.e1. doi:10.1016/j.ajo.2010.04.028. PMID:20630492.
- Turgeon RD, Barry AR, Pearson GJ. Familial hypercholesterolemia: Review of diagnosis, screening, and treatment. Canadian family physician Medecin de famille canadien. 2016;62(1):32-7. PMID:26796832; PMCID:PMC4721838.
- Ang M, Wong W, Park J, Wu R, Lavanya R, Zheng Y, et al. Corneal arcus is a sign of cardiovascular disease, even in low-risk persons. American journal of ophthalmology. 2011;152(5):864-71.e1. doi:10.1016/j.ajo.2011.04.014. PMID:21742308.
- Christoffersen M, Frikke-Schmidt R, Schnohr P, Jensen GB, Nordestgaard BG, Tybjærg-Hansen A. Xanthelasmata, arcus corneae, and ischaemic vascular disease and death in general population: prospective cohort study. BMJ (Clinical research ed.). 2011;343:d5497. doi:10.1136/bmj.d5497. PMID:21920887; PMCID:PMC3174271.
- Fernandez AB, Keyes MJ, Pencina M, D’Agostino R, O’Donnell CJ, Thompson PD. Relation of corneal arcus to cardiovascular disease (from the Framingham Heart Study data set). The American journal of cardiology. 2009;103(1):64-6. doi:10.1016/j.amjcard.2008.08.030. PMID:19101231; PMCID:PMC2636700.
- Chambless LE, Fuchs FD, Linn S, Kritchevsky SB, Larosa JC, Segal P, et al. The association of corneal arcus with coronary heart disease and cardiovascular disease mortality in the Lipid Research Clinics Mortality Follow-up Study. American journal of public health. 1990;80(10):1200-4. doi:10.2105/ajph.80.10.1200. PMID:2400030; PMCID:PMC1404822.
- Wong MYZ, Man REK, Gupta P, Lim SH, Lim B, Tham Y-C, et al. Is corneal arcus independently associated with incident cardiovascular disease in Asians? Am J Ophthalmol. 2017;183:99-106. doi:10.1016/j.ajo.2017.09.002.
- Zech LA Jr, Hoeg JM. Correlating corneal arcus with atherosclerosis in familial hypercholesterolemia. Lipids in health and disease. 2008;7:7. doi:10.1186/1476-511X-7-7. PMID:18331643; PMCID:PMC2279133.