Hypertensive retinopathy is a disease in which systemic arterial hypertension damages the retinal microvessels and the retinal nerve fiber layer. Hypertension is defined as SBP ≥140 mmHg and/or DBP ≥90 mmHg 1). According to the 2017 ACC/AHA criteria, it is further classified into elevated blood pressure (120–129/<80 mmHg), Stage 1 (130–139/80–89 mmHg), and Stage 2 (≥140/≥90 mmHg).
The number of hypertensive patients worldwide exceeds 1.4 billion, and more than 10 million people die each year from hypertension-related diseases 1). It is projected to exceed 1.5 billion by 2025 1). Hypertensive retinopathy is detected in 6–15% of the non-diabetic population aged 40 years and older 1)3), and in 30.6–51% of all hypertensive patients 3)9). Approximately 50% of US adults have hypertension 7), and the prevalence of fundus changes is high. Arteriosclerotic changes due to chronic hypertension progress without subjective symptoms and are often discovered during health checkups.
Two processes are involved in the pathophysiology. Acute vasospastic changes are prominent in young individuals and secondary hypertension, and can be reversibly improved with appropriate blood pressure reduction. Chronic arteriosclerotic changes are predominant in middle-aged and elderly patients with long-standing hypertension and are irreversible.
This disease was first described by Marcus Gunn at the end of the 19th century. In the 1930s, the Keith-Wagener-Barker (KWB) classification was established and is still widely used today 1). Hypertensive retinopathy is not only an ophthalmological finding but also an important independent risk indicator for cardiovascular disease and stroke.
Cases have been reported where the underlying cause of secondary hypertension triggers fundus changes. In pheochromocytoma, malignant hypertension and retinopathy can be the initial symptoms 5). IgA nephropathy may be complicated by Purtscher-like retinopathy 8). Goodpasture syndrome 4) and tuberculosis 6) have also been reported to present with retinopathy via secondary hypertension.
QHow does hypertension affect the eyes?
A
Hypertension affects multiple tissues of the eye. In the retina, hypertensive retinopathy occurs, including vasospasm, hemorrhages, exudates, and papilledema. In the choroid, hypertensive choroidopathy occurs with Elschnig spots and Siegrist streaks. In the optic nerve, papilledema can lead to optic atrophy. Long-term, it is also known to increase the risk of retinal vein occlusion and glaucoma.
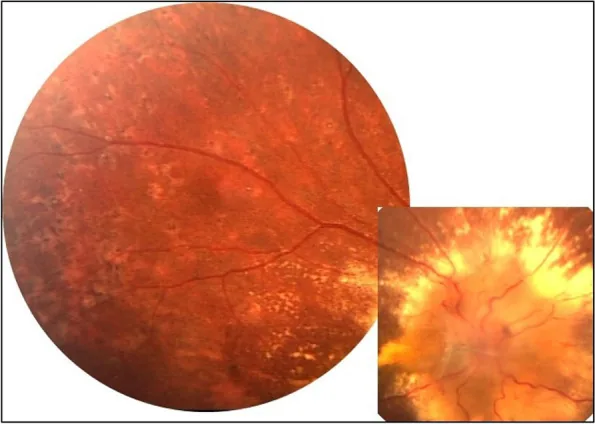
Özdal PÇ, et al. Choroidal involvement in systemic vasculitis: a systematic review. J Ophthalmic Inflamm Infect. 2022. Figure 2. PMCID: PMC8980189. License: CC BY.
Color fundus photograph showing marked edema of the optic disc and yellowish-white exudative spots. This directly shows fundus findings seen in severe hypertensive retinopathy and is suitable for explaining clinical findings.
Fundus findings in hypertensive retinopathy show characteristic changes according to the stage. Three stages—vasospastic, sclerotic, and exudative—progress sequentially.
Vasospastic Phase
Generalized arteriolar narrowing: The arteriovenous ratio (AVR) decreases from the normal 2:31)3).
Focal arteriolar narrowing: Observed as caliber irregularity1)3).
Vasospasm: Prominent in young individuals and secondary hypertension. This stage is reversible with appropriate blood pressure reduction.
Sclerotic Phase
Increased light reflex: The light reflex of the artery becomes broader, progressing to copper-wire and silver-wire arteries1)3).
Arteriovenous crossing phenomenon (AV nicking): The vein is compressed and narrowed at the arteriovenous crossing1)3). This is an indicator of current and past blood pressure persistence1). At the crossing, venous deflection (Salus sign), tapering of the vein on both sides of the crossing (Gunn sign), and right-angle deflection of the vein (Bonnet sign) are observed.
Sclerotic changes: Irreversible changes due to intimal thickening, medial hypertrophy, and hyalinization.
Exudative Phase
Hemorrhage: Flame-shaped, dot, and blot hemorrhages1)3).
Exudates: Hard exudates (lipoprotein deposits) and soft exudates (nerve fiber layer infarcts)1)3). In malignant hypertension, hard exudates arrange radially in the macula, forming a macular star.
Papilledema: A severe finding in malignant hypertension1). May be accompanied by Elschnig spots2).
Elschnig spots are yellowish-white lesions caused by damage to the retinal pigment epithelium (RPE) due to fibrinoid necrosis of choroidal arterioles2)7). On OCTA, they are observed as hypointense spots in the choriocapillaris layer2).
On OCTA, disruption of the tapering pattern (vessels becoming thinner toward the periphery) in the superficial and deep capillary plexuses and enlargement of the foveal avascular zone (FAZ) are observed2). Decreased vessel density in the superficial vascular plexus (SVP) is also a characteristic finding1).
In malignant hypertension, cases with vitreous cells of 2+ or more have been reported 7). Differentiation from endophthalmitis and uveitis may be necessary.
QHow is the severity of hypertensive retinopathy classified?
A
A representative classification is the KWB classification (Groups I–IV): Group I: mild arteriolar narrowing and sclerosis; Group II: marked narrowing and AV nicking; Group III: hemorrhages, exudates, and retinal edema; Group IV: papilledema. The Scheie classification independently evaluates hypertensive changes (H1–4) and arteriosclerotic changes (S1–4). The Wong-Mitchell classification (2004) has four stages: none, mild, moderate, and severe, and is used in modern epidemiological studies. A new OCT-based classification proposes three types: (1) mild to moderate, (2) malignant without SRF, and (3) malignant with SRF 1).
The presence of hypertension itself is essential for the development of hypertensive retinopathy, and the following factors increase the risk of retinopathy through hypertension.
Excessive salt intake, obesity, smoking, excessive alcohol consumption, family history: Major risk factors for essential hypertension
Oxidative stress: An association with elevated plasma ferritin has been shown 1)
Chronic low-grade inflammation: Elevated high-sensitivity CRP (hsCRP) correlates with the prevalence and severity of retinopathy 1)
Enhanced platelet activation: Urinary 11-dehydro-TXB2 shows a positive correlation with retinopathy 1)
SNPs associated with retinal vessel diameter have been identified: 8 SNPs for central retinal vein equivalent (CRVE) and 2 SNPs for central retinal artery equivalent (CRAE) 1).
Arteriolar narrowing is not only a result of hypertension but can also be a cause. A meta-analysis of 10,229 individuals showed that retinal arteriolar narrowing is associated with the risk of developing hypertension up to 10 years later 1).
Antihypertensive Medication Adherence and Risk of Progression
A meta-analysis of 12,603 individuals reported a high rate of non-adherence to antihypertensive medication at 45.1% 1). Poor adherence is directly linked to long-term progression of fundus lesions.
It is often discovered through fundus examination requests from internal medicine, and in some cases, visual impairment leads to the detection of kidney disease or secondary hypertension. At the initial visit, diagnosis is confirmed by blood pressure measurement and blood tests.
Fundus examination is the basis of diagnosis. Since direct ophthalmoscopy has high inter-observer variability, slit-lamp fundus examination under mydriasis or fundus photography is recommended 1).
The KWB classification is a classic severity classification for hypertensive retinopathy.
The Scheie classification independently evaluates hypertensive changes (H1 to H4) and arteriosclerotic changes (S1 to S4), allowing differentiation between acute effects of blood pressure and chronic sclerotic changes.
SD-OCT: Can measure central retinal artery and vein diameters (CRA and CRV diameters) and AVR1). Useful for monitoring retinal nerve fiber layer (RNFL) thickness1).
OCTA: Enables measurement of vessel density in superficial and deep capillary plexuses and quantification of FAZ area1)2). Can visualize ischemic areas and Elschnig spots in more detail than fluorescein angiography (FA)1)2). Suitable for repeated evaluation as it does not require contrast agents.
Adaptive optics (AO) fundus imaging: Allows measurement of wall-to-lumen ratio (WLR), which is significantly increased in hypertensive patients (0.370 vs. normal 0.240)1).
QWhat are the advantages of OCTA compared to conventional fluorescein angiography?
A
OCTA can visualize retinal and choroidal vascular layers in a layer-by-layer manner without contrast agents. In hypertensive retinopathy, it can quantitatively assess vessel density in superficial and deep capillary plexuses and FAZ area, and detect ischemic areas and Elschnig spots (hypointense spots in the choriocapillaris) in more detail than conventional fluorescein angiography1)2). It is noninvasive and suitable for repeated longitudinal evaluation.
The cornerstone of treatment for hypertensive retinopathy is systemic blood pressure control. For emergency blood pressure reduction in malignant hypertension, it is recommended to lower the mean arterial pressure (MAP) by 10–15% within the first hour and to within 25% of baseline within 24 hours. Rapid blood pressure reduction is contraindicated because it can cause ischemia of the retina, brain, and kidneys. The goal is to achieve SBP <130 mmHg and DBP <80 mmHg within 2–3 months.
Nicardipine continuous intravenous infusion / Nitroprusside: Used for emergency blood pressure reduction in malignant hypertension7)
ACE inhibitors (e.g., irbesartan): Have an inhibitory effect on the progression of hypertensive retinopathy and lead to structural improvement of arterioles (normalization of wall-to-lumen ratio)1)
A 10-month continuation of triple therapy with irbesartan + atenolol + amlodipine resulted in a four-stage improvement from KWB group IV to group I1).
Specific treatment for secondary hypertension is also important. In pheochromocytoma, after emergency blood pressure reduction with continuous intravenous labetalol (0.25 mg/kg/h), complete recovery of best-corrected visual acuity to 20/20 was achieved in a case that underwent laparoscopic adrenalectomy5).
With blood pressure control, hemorrhages and soft exudates may resolve within about 3 months4). On the other hand, arteriovenous crossing changes and arterial narrowing often remain irreversible. In many cases, these improve with renal function improvement, but irreversible damage due to hard exudate deposition and retinal pigment epithelium atrophy may persist. Regular collaboration with internal medicine to confirm systemic status is necessary.
Intravitreal anti-VEGF injection (bevacizumab, ranibizumab): Efficacy has been reported for macular edema and subretinal fluid in malignant hypertensive retinopathy1)
Retinal photocoagulation: Applied for neovascularization in proliferative hypertensive retinopathy
Khojasteh et al. (2021) reported improvement in best-corrected visual acuity from 20/400 to 20/50 after performing 23-gauge microincision vitrectomy surgery (MIVS) + direct drainage of hemorrhage with a 41-gauge needle + internal limiting membrane (ILM) flap technique for foveal intraretinal hemorrhage9).
QCan hypertensive retinopathy be cured by controlling blood pressure?
A
Whether improvement is possible depends on the disease stage. Changes in the vasospastic phase (arteriolar narrowing, hemorrhages, soft exudates) may improve within weeks to 3 months with appropriate blood pressure reduction 4). In contrast, arteriosclerotic changes due to chronic hypertension (copper/silver wire arteries, arteriovenous nicking) are essentially irreversible and persist after blood pressure control. See “Pathophysiology and Detailed Mechanisms” section for details.
Elevated intraluminal pressure triggers autoregulation, causing arteriolar vasospasm 1)3). For every 10 mmHg increase in mean arterial blood pressure (MABP), retinal arteriolar diameter decreases by approximately 3 μm 1). Changes at this stage are reversible.
Sustained hypertension leads to intimal thickening, medial smooth muscle proliferation, and hyaline degeneration 1)3). Degeneration and necrosis of medial smooth muscle cells, along with fibrotic thickening of the media and adventitia, cause organic narrowing, reflected in the fundus as enhanced blood column reflex (copper wire → silver wire arteries) and arteriovenous nicking. Sclerotic arteries compress adjacent veins, increasing the risk of venous thrombosis.
Breakdown of the blood-retinal barrier (BRB) allows plasma components to leak into the retina, resulting in hemorrhages, hard exudates, and soft exudates 1)3). Fibrinoid necrosis is the most severe change 3); fibrinoid necrosis of choroidal arterioles causes segmental infarction of the choriocapillaris, forming Elschnig spots 2). In end-stage chronic renal failure, choroidal circulatory disturbance may occur, leading to breakdown of the outer blood-retinal barrier, subretinal exudation, and serous retinal detachment. As capillary occlusion progresses, microaneurysms, venous caliber irregularity, and vascular anastomoses may appear; rarely, retinal nonperfusion areas and neovascularization develop, resulting in proliferative retinopathy.
Retinal vessels are characterized by the presence of the BRB, lack of sympathetic innervation, and blood flow autoregulation 3). These properties determine the response to systemic and local blood pressure changes.
RAAS (Renin-Angiotensin-Aldosterone System): An independent RAS pathway (ACE1-AngII-AT1R) also exists locally in the eye 1)3). The Mas receptor acts antagonistically to AT1R and plays a protective role 1).
VEGF: Released by hypoxic stimulation, it increases vascular permeability 1). Proliferative hypertensive retinopathy is a condition first reported in 2016, and VEGF is a major promoting factor 1).
NO (Nitric Oxide) Impairment: Impaired NO-dependent vasodilation leads to decreased retinal blood flow 1).
Endothelin-1 (ET-1): Involved in BRB disruption and VEGF stimulation; ET receptor antagonists have a protective effect 1).
QWhat are the prevention methods for hypertensive retinopathy?
A
Fundamental prevention is maintaining blood pressure within the normal range. Regular home blood pressure monitoring, lifestyle improvements such as salt reduction, moderate exercise, smoking cessation, and moderate alcohol consumption are effective. It is also important to continue taking prescribed antihypertensive medications; a meta-analysis shows a high non-adherence rate of 45.1%, which is a challenge 1). Regular fundus examinations can detect lesions at an asymptomatic stage, and early intervention can prevent progression to irreversible changes.
7. Latest Research and Future Perspectives (Research Stage Reports)
The fusion of adaptive optics (AO) and OCT/OCTA has enabled measurement of the wall-to-lumen ratio (WLR) of retinal arterioles in vivo 1). Quantification of microvascular density is being studied as an early diagnostic marker for hypertensive retinopathy 2). OCTA is superior to FA in detailed visualization of ischemic areas and Elschnig spots 2) and is expected as a non-invasive disease assessment tool.
Endocannabinoid System (ECS): Retinal protective effects mediated by CB1/CB2 receptors have been shown in animal models, attracting attention as a new therapeutic target 3).
Proteasome subunits: LMP10 inhibition and β5i subunit deletion may reduce retinal vascular damage1).
GPR174 knockout: Reduced vascular permeability has been confirmed in animal models1).
Endothelin receptor antagonists: Under investigation as therapeutic candidates to suppress ET-1-induced BRB disruption1).
NADPH oxidase (Nox) inhibition: BRB protection via Nox1/4 inhibition and neovascularization suppression via Nox5 inhibition have been reported1).
Serum uric acid (SUA), marinobufagenin, and GlycA are being evaluated as predictive biomarkers for hypertensive retinopathy1). Genetic studies have progressed in identifying SNPs associated with retinal vessel diameter, which may lead to early detection of genetically high-risk groups1).
Studies using BPH/2J mice (genetic hypertension model) have analyzed the autoregulatory mechanisms of retinal vessels in detail1). Due to homology with human hypertensive retinopathy, they are used for preclinical evaluation of novel therapies.
Dziedziak J, Zaleska-Żmijewska A, Szaflik JP, Cudnoch-Jędrzejewska A.. Impact of Arterial Hypertension on the Eye: A Review of the Pathogenesis, Diagnostic Methods, and Treatment of Hypertensive Retinopathy. Med Sci Monit. 2022;28:e935135. doi:10.12659/msm.935135. PMID:35046380; PMCID:PMC8790937.
Alswailmi FK. A cross talk between the endocannabinoid system and different systems involved in the pathogenesis of hypertensive retinopathy. Pharmaceuticals. 2023;16(3):345. doi:10.3390/ph16030345. PMID:36986445; PMCID:PMC10058254.
Eppenberger LS, Schmid MK, Clerici M. Acute Ocular Complications after Recently Diagnosed Goodpasture’s Syndrome - An Unusual Case of Hypertensive Retinopathy. Klinische Monatsblatter fur Augenheilkunde. 2023;240(4):505-508. doi:10.1055/a-2034-6314. PMID:37164428; PMCID:PMC10129409.
Billia F, Palmieri N, Maccari A, Menna F, Consigli A. Hypertensive Retinopathy as a Presenting Sign of Pheochromocytoma with Malignant Hypertension: A Child Case. Case reports in ophthalmology. 2023;14(1):348-352. doi:10.1159/000531663. PMID:37901632; PMCID:PMC10601789.
Mehta AA, Ashok A, Praveen VP, Kiran Kumar B. Tuberculosis presenting as uncontrolled hypertension. Respiratory medicine case reports. 2024;50:102063. doi:10.1016/j.rmcr.2024.102063. PMID:38903655; PMCID:PMC11186969.
Davis A, Blumenthal J, Hoyek S, Rizzo JF, Patel NA.. Atypical Presentation of Vitreous Inflammation in a Patient With Hypertensive Retinopathy. J Vitreoretin Dis. 2024;8(5):614-617. doi:10.1177/24741264241264361. PMID:39345867; PMCID:PMC11437536.
Çevik TS, Kocaman Ata S, Özdamar Erol Y, Eser EP. IgA Nephropathy Associated Hypertensive Retinopathy and Purtscher-Like Retinopathy. Journal of vitreoretinal diseases. 2025;9(6):24741264251366409. doi:10.1177/24741264251366409. PMID:40901630; PMCID:PMC12399575.
Khojasteh H, Akhavanrezayat A, Ghoraba H, Nguyen QD.. Novel surgical approach for removing intraretinal loculated foveal hemorrhage in a patient with hypertensive retinopathy. Am J Ophthalmol Case Rep. 2021;24:101217. doi:10.1016/j.ajoc.2021.101217. PMID:34646960; PMCID:PMC8501509.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.