Ectropion refers to a condition in which the palpebral conjunctiva, which normally contacts the ocular surface (cornea and bulbar conjunctiva), turns outward and becomes exposed. It occurs when the anterior lamella (skin and orbicularis oculi muscle) is relatively deficient compared to the posterior lamella (tarsus and conjunctiva), or when the supporting tissues of the tarsus become lax. Due to gravity, it most commonly occurs in the lower eyelid.
The everted eyelid margin separates from the ocular surface, and the punctum also turns outward. This impairs normal tear drainage, leading to epiphora, discharge, and damage from corneal exposure. It is a frequently encountered condition in elderly outpatient clinics, affecting patients’ quality of life both cosmetically and functionally.
Based on the cause, it is broadly classified into four types: involutional (age-related), paralytic, cicatricial, and mechanical. Since the pathophysiology differs for each type, the choice of treatment also varies accordingly.
QWhat is the difference between ectropion and entropion?
A
Ectropion is a condition in which the eyelid margin is displaced outward (away from the eye). In contrast, entropion is a condition in which the eyelid margin is displaced inward (toward the eye), causing the eyelashes to rub against the cornea. Both conditions result from abnormalities in the supporting structures of the eyelids, but their symptoms and treatments differ.
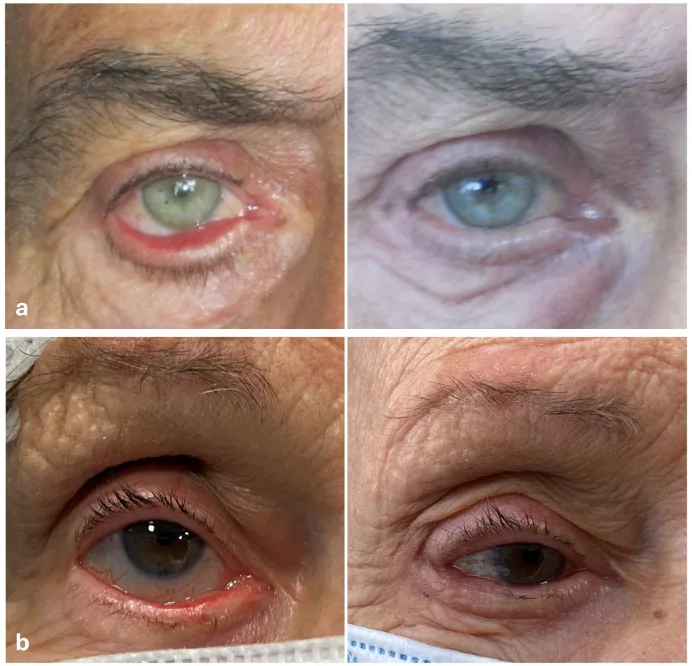
Rubino C, et al. 3-Step Combined Technique for Correction of Involutional Lower Eyelid Ectropion: A Case Series. J Clin Med. 2024;14(1):128. DOI: 10.3390/jcm14010128. Figure 2. License: CC BY 4.0. PMCID: PMC11721973.
Preoperative findings of involutional ectropion showing the lower eyelid margin separated outward from the bulbar conjunctiva, with extensive exposure and congestion of the tarsal conjunctiva (top: 73-year-old male, bottom: 81-year-old female). These correspond to the eyelid conjunctival exposure, punctal ectropion, and conjunctival congestion discussed in the section “Main Symptoms and Clinical Findings.”
The most common complaint in ectropion is epiphora (tearing). The outward displacement of the punctum disrupts the tear drainage pathway, causing continuous overflow of tears. Cosmetic concerns (the eyelid appearing turned outward) are often the most distressing issue for patients.
The main subjective symptoms are listed below.
Epiphora: Tear drainage disorder due to punctal ectropion. This is the most frequent complaint.
Mucous discharge: Increased secretion due to conjunctival exposure.
The following findings are confirmed by slit-lamp examination and visual inspection.
Exposure, keratinization, and thickening of the palpebral conjunctiva: When the conjunctiva is exposed to air for a long time, it becomes keratinized and thickened. In involutional ectropion, the everted conjunctiva may appear tumor-like, requiring differentiation from malignant tumors.
Punctal ectropion: The punctum is displaced away from the ocular surface and points away from the eye.
Corneal epithelial damage: Punctate keratopathy is observed with fluorescein staining. If left untreated, it may progress to keratitis, corneal ulcer, and perforation.
Scleral show: In lower eyelid retraction and ectropion associated with facial nerve palsy, the inferior sclera is exposed, resulting in a scleral show.
Lagophthalmos: In paralytic ectropion, relaxation of the orbicularis oculi muscle leads to incomplete eyelid closure, exposing the cornea even during sleep.
Characteristic clinical findings by type are shown in the table below.
Type
Characteristic Findings
Involutional
Laxity of the entire lower eyelid, conjunctival keratinization and thickening, punctal ectropion
Paralytic
Eyebrow drooping, mouth drooping, loss of nasolabial fold, scleral show, lagophthalmos
Cicatricial
Skin shortening at the scar contracture site, history of trauma or burns
Mechanical
Downward traction due to eyelid tumor/edema
QWhat is the most troubling symptom of ectropion?
A
Epiphora (tearing) is the most frequent complaint, but cosmetic concerns can be the most serious in some cases. If inadequate corneal protection persists, it can progress to punctate keratopathy, keratitis, and corneal ulcer, ultimately posing risks of corneal perforation and visual impairment. Particularly in paralytic ectropion, lagophthalmos (incomplete eyelid closure) can accelerate corneal damage, requiring caution.
Ectropion is classified into 4 types based on cause. The pathophysiology, characteristics, and frequency of each type are summarized in the table below.
Type
Pathophysiology
Age of Onset
Frequency
Involutional (degenerative)
Laxity of medial/lateral canthal tendons and orbicularis oculi muscle
Elderly
Most common
Paralytic
Orbicularis oculi muscle relaxation after facial nerve palsy
Age-related collagen degeneration and loss of elasticity of the medial and lateral canthal tendons lead to horizontal eyelid laxity. Weakening of the orbicularis oculi muscle also contributes to laxity. It commonly occurs in the lower eyelid and is the most frequently encountered type in geriatric ophthalmology clinics. It progresses gradually with age and does not resolve spontaneously.
Due to dysfunction of the facial nerve (cranial nerve VII), the tension of the orbicularis oculi muscle is lost, reducing support for the lower eyelid. Causes include Bell’s palsy, tumors, trauma, and after surgery. It is often accompanied by incomplete eyelid closure (lagophthalmos), increasing the risk of corneal damage. Since Bell’s palsy resolves spontaneously within 6 months in many cases, corneal protection should be maintained during this period while monitoring the condition.
This is a condition in which the anterior lamella (skin and orbicularis oculi muscle) is shortened due to scar contraction, pulling the eyelid margin outward. Causes include trauma, burns, chemical burns, Stevens-Johnson syndrome (SJS), after healing of a giant chalazion, and after eyelid surgery. If the underlying disease remains active, it is refractory, and surgery should be planned after the disease has subsided.
This is a condition in which the eyelid is pulled downward by the weight of an eyelid tumor or eyelid edema. Removal of the causative tumor or management of edema is the priority, and ectropion often improves after the cause is eliminated.
Involutional ectropion is the most common type, occurring frequently in the elderly (especially those aged 60 and older). Paralytic ectropion occurs at all ages, often due to Bell’s palsy (approximately 20–30 per 100,000 population per year 1)). Prevalence data for ectropion overall in Japan are insufficient (source_gaps recorded), and no consistent trend regarding sex differences has been shown 2).
Diagnosis of ectropion is easy by visual inspection to confirm exposure of the palpebral conjunctiva. In cases of facial nerve palsy, diagnosis is generally easy based on history and findings such as eyebrow droop, drooping of the mouth corner, and disappearance of the nasolabial fold.
The pinch test (snap-back test) is most widely used to evaluate horizontal eyelid laxity. The eyelid is pinched with fingers and pulled forward, and the return after release is assessed. If the eyelid separates more than 6–8 mm from the globe, horizontal laxity is considered present. If it does not return quickly to its original position without blinking after release, this is also evidence of laxity.
Other tests are shown below.
Distraction test: The eyelid is pulled forward, and the distance the tarsal plate separates from the globe is measured. Normal is considered less than 6 mm.
Snap-back test: The eyelid is pulled downward and released, and whether it returns to its original position without blinking is assessed. Slow or no return suggests laxity.
Fluorescein staining: Used to confirm corneal epithelial disorders (punctate keratopathy, corneal erosion, ulcer).
Slit-lamp microscopy: Evaluates the degree of conjunctival injection and keratinization, and details of corneal lesions.
Nerve conduction velocity test / Head MRI: Performed when facial nerve palsy is suspected to investigate the cause.
Eyelid malignancy: Age-related ectropion with keratinized and thickened conjunctiva may appear tumor-like. Differentiation from squamous cell carcinoma, basal cell carcinoma, etc., is necessary; biopsy should be performed if suspected.
Entropion: Entropion is the opposite condition where the eyelid margin turns toward the eye, causing lashes to irritate the cornea. The direction of displacement is opposite to ectropion.
Lagophthalmos (incomplete eyelid closure): Incomplete eyelid closure associated with facial nerve palsy often coexists with ectropion.
QThe everted conjunctiva is swollen and looks like a mass. Could it be a tumor?
A
In age-related ectropion, prolonged exposure of the conjunctiva can lead to keratinization and thickening, sometimes appearing as a tumor-like mass. Differentiation from malignant tumors (e.g., squamous cell carcinoma) is necessary. If ectropion treatment alone does not improve the condition or if rapid changes are observed, a biopsy should be performed.
Conservative treatment is indicated for mild cases or for paralytic cases soon after onset. Since Bell’s palsy often resolves spontaneously within 6 months, it is recommended to observe the patient while ensuring thorough corneal protection during this period.
Frequent instillation of artificial tears: Symptomatic treatment for corneal exposure. Use about 4 to 8 times daily. Preservative-free formulations (e.g., 0.1% sodium hyaluronate eye drops) are preferred.
Ophthalmic ointment application: Used before bedtime to protect the cornea (e.g., white petrolatum-based ophthalmic ointment). This is especially important in paralytic ectropion with lagophthalmos.
Taping: A simple method to temporarily correct ectropion by pulling the lower eyelid upward and outward. Useful for mild cases or during the preoperative waiting period.
Nighttime eye patch or moisture chamber: Used to protect the cornea during sleep in cases of lagophthalmos.
Surgery is indicated for cases that do not improve with conservative treatment, or for age-related, cicatricial, or other types where spontaneous resolution is not expected. Representative surgical procedures are shown in the table below.
Cut the lateralmost tarsal plate and suture it to the periosteum of the lateral orbital rim
Auricular cartilage graft
Posterior lamella reinforcement in severe cases
Conchal cartilage grafted as a spacer
Flap and skin graft
Cicatricial ectropion (skin deficiency)
Cover the skin defect with a flap or free skin graft
Most cases of eyelid ectropion can be managed with one of the following procedures: wedge resection, Kuhnt-Szymanowski method, or lateral tarsal strip method.
Lateral tarsal strip method is the first choice. It restores the fixation strength of the lateral canthal tendon and reliably corrects horizontal laxity.
Wedge resection: Selected when laxity is relatively mild.
Kuhnt-Szymanowski method: Suitable for cases with excess skin. Adds orbicularis oculi muscle shortening and skin excision to wedge resection.
Paralytic ectropion
Lower eyelid: Lateral tarsal strip method, wedge resection, and conchal cartilage graft are used.
Upper eyelid (lagophthalmos): Levator palpebrae superioris lengthening (lid loading with gold plate or fascia graft) is indicated.
Timing of surgery: Plan after a 6-month period of spontaneous recovery from onset.
Cicatricial ectropion
Principle: After releasing the scar tissue, perform a flap or skin graft according to the skin deficiency.
Timing of surgery: Plan after the underlying disease activity has subsided. Be especially cautious after SJS and chemical burns.
Full-thickness skin graft: For extensive skin defects of the lower eyelid, grafts from the postauricular area or supraclavicular fossa are performed.
Mechanical ectropion
Treat the cause first: Prioritize resection of the causative tumor or management of edema.
Eyelid reconstruction: Plan eyelid repair if ectropion persists after removal of the cause.
QWhich surgical method is most effective?
A
Most cases can be managed with wedge resection, Kuhnt-Szymanowski procedure, or lateral tarsal strip procedure. The technique is selected according to the degree of laxity and the type of cause. For age-related ectropion, the lateral tarsal strip procedure shows particularly stable results. Severe cases or cicatricial ectropion with skin deficiency may require additional procedures such as auricular cartilage grafting, flaps, or skin grafts.
QCan ectropion recur after surgery?
A
The prognosis for age-related and paralytic ectropion is generally good. However, with advancing age, eyelid laxity may progress again, sometimes requiring reoperation. Cicatricial ectropion tends to recur if the underlying disease remains active. Regular postoperative follow-up is important.
The eyelid is broadly divided into the anterior lamella (skin and orbicularis oculi muscle) and the posterior lamella (tarsus and conjunctiva). The tarsus maintains the shape as the eyelid skeleton and houses the meibomian glands. The medial canthal tendon (medial palpebral ligament) and lateral canthal tendon (lateral palpebral ligament) fix the medial and lateral ends of the tarsus to the orbital bone, maintaining the horizontal position of the eyelid. The orbicularis oculi muscle (innervated by the facial nerve) is responsible for eyelid closure and the lacrimal pump function. Disruption of these supporting structures is the essence of ectropion.
Age-related: Collagen degeneration of the medial and lateral canthal tendons → loss of elasticity → increased horizontal laxity. Weakening of the orbicularis oculi muscle also contributes to laxity. The horizontal tension of the eyelid is lost, and the eyelid margin separates from the ocular surface.
Paralytic: Damage to the facial nerve (cranial nerve VII) → loss of orbicularis oculi tone → decreased lower eyelid support + incomplete eyelid closure. The lower eyelid is pulled outward by gravity, and the upper eyelid also closes incompletely.
Cicatricial: Scar contracture of the anterior lamella (skin side) → shortening of the anterior lamella → the eyelid margin is pulled forward and outward. Since only the anterior lamella is shortened while the posterior lamella remains normal length, the eyelid margin is everted.
Mechanical: Weight of a mass or edema → downward traction → eversion of the eyelid. The condition resolves once the cause is removed.
Persistent ectropion leads to the following sequence of changes.
Punctal eversion → impaired tear drainage → epiphora: Normally, the punctum contacts the ocular surface, but when eversion causes the punctum to separate from the eye, tears overflow without being directed into the lacrimal sac.
Exposure of palpebral conjunctiva → dryness → keratinization and thickening: The conjunctiva that normally contacts the inner surface of the eye is exposed to air, leading to keratinization and thickening due to chronic irritation. It may appear as a mass.
Corneal exposure → increased evaporation → corneal epithelial damage → corneal ulcer → perforation: Especially in paralytic ectropion with incomplete eyelid closure, the cornea may be exposed even during sleep, leading to rapid progression of epithelial damage.
The prognosis for surgery for age-related and post-facial nerve palsy ectropion is generally good. The lateral tarsal strip procedure has been shown to be effective in various reports 3), and long-term correction of ectropion can be expected.
Cicatricial ectropion may be refractory when the underlying disease is active (e.g., after Stevens-Johnson syndrome or chemical burns), and multiple surgeries may be required. Inadequate corneal protection poses risks of corneal ulcer, perforation, and visual impairment.
Presence of recurrent laxity: Especially in age-related ectropion, recurrent laxity may occur with advancing age. Regular outpatient follow-up after surgery is recommended.
Confirmation of corneal epithelial improvement: Evaluate postoperative corneal findings with fluorescein staining to determine the need for eye drop treatment.
Course of the underlying disease in paralytic ectropion: Bell’s palsy recovers within 6 months in most cases. Follow the neurological recovery of the causative disease.
Scar maturation in cicatricial ectropion: Skin scars soften and mature over time. Surgery is performed when the underlying disease has subsided and the scar is stable.
QCan it heal without surgery?
A
Age-related and cicatricial ectropion do not resolve spontaneously and often require surgery. Paralytic ectropion may resolve spontaneously with recovery of the underlying cause such as Bell’s palsy, but surgery may be expedited if there is a risk of corneal damage. In mechanical ectropion, removing the cause may improve the ectropion.
Long-term outcomes of the lateral tarsal strip procedure: Long-term follow-up studies report high success rates over 5 years postoperatively 3,4). However, some relaxation may recur with aging, and reoperation rates vary by report.
Medial spindle procedure (medial triangular resection): This method involves triangular resection of the conjunctiva and tarsal plate near the medial canthus for ectropion with medial punctal ectropion. Its usefulness as a procedure specialized for correcting punctal ectropion has been reported 5).
Hyaluronic acid filler injection: As a non-surgical treatment for patients who do not wish for invasive surgery, filler injection around the orbit is being considered. Temporary improvement has been reported, but evidence for long-term outcomes is limited 6).
Botulinum toxin: Botulinum toxin injection into the orbicularis oculi muscle of the unaffected side may be performed to improve asymmetry due to facial nerve palsy. Some reports indicate effectiveness for aesthetic symmetrization 7).
Peitersen E. Bell’s palsy: the spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta Otolaryngol Suppl. 2002;549:4-30.
Damasceno RW, Osaki MH, Dantas PE, Belfort R Jr. Involutional entropion and ectropion of the lower eyelid: prevalence and associated risk factors in the elderly population. Ophthal Plast Reconstr Surg. 2011;27(5):317-20.
Schaefer AJ. Variation in the technique of the lateral tarsal strip procedure. Ophthalmology. 1983;90(5):588-92.
Benger RS, Frueh BR. Involutional ectropion: a review of the management. Ophthalmic Surg. 1987;18(2):136-9.
Rougraff PM, Tse DT, Johnson TE, Feuer W. Involutional entropion repair with fornix sutures and lateral tarsal strip procedure. Ophthal Plast Reconstr Surg. 2001;17(4):281-7.
Goldberg RA, Lee S, Jayasundera T, Tsirbas A, Douglas RS, McCann JD. Treatment of lower eyelid retraction by expansion of the lower eyelid with hyaluronic acid gel. Ophthal Plast Reconstr Surg. 2007;23(5):343-8.
Salinas NL, Jackson O, Walker NJ. Treating facial paralysis: the plastic surgeon’s role. Clin Plast Surg. 2016;43(2):367-80.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.