Cicatricial conjunctivitis is a general term for chronic conjunctivitis in which scar formation is observed in the conjunctiva. Chronic inflammation of the conjunctiva stimulates fibroblasts, promoting the formation of extracellular matrix and leading to conjunctival fibrosis and alteration of the ocular surface.
The causes of scar formation are diverse. They include infectious conjunctivitis (such as trachoma and epidemic keratoconjunctivitis) that progresses to scarring in the chronic phase after pseudomembrane formation in the acute phase, non-infectious conjunctivitis such as Stevens-Johnson syndrome (SJS) and ocular pemphigoid, and external factors such as chemical trauma and drug toxicity.
The most common cause of active, progressive cicatricial conjunctivitis is ocular cicatricial pemphigoid (OCP). OCP is an autoimmune disease within the spectrum of mucous membrane pemphigoid (MMP), occurring in 1 in 10,000 to 50,000 people5). It predominantly affects elderly women, with a male-to-female ratio of approximately 1:25). A surveillance study in the UK reported an annual incidence of cicatricial conjunctivitis of about 1.3 per million population.
QWhat is the difference between ocular cicatricial pemphigoid and mucous membrane pemphigoid?
A
Mucous membrane pemphigoid (MMP) is a general term for autoimmune diseases that cause blisters and erosions in various mucous membranes including the oral cavity, eyes, nasopharynx, larynx, esophagus, and genitalia. In ophthalmology, cases with ocular involvement are called ocular cicatricial pemphigoid (OCP). OCP may target only the ocular mucosa, but about 50% of cases have extraocular involvement such as oral or skin lesions2).
Hwang S, et al. Corneal perforation in ocular cicatricial pemphigoid: A CARE-compliant case report. Medicine (Baltimore). 2021. Figure 3. PMCID: PMC8702268. License: CC BY.
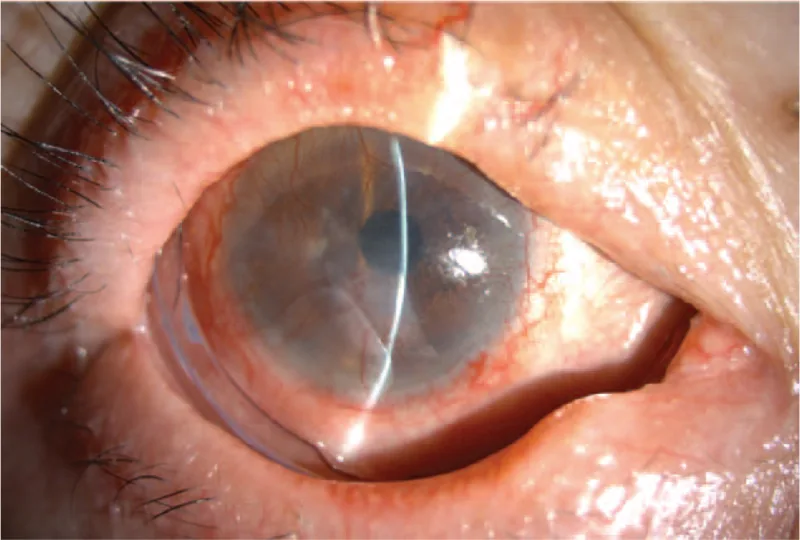
Slit-lamp photograph of the right eye at 1 year postoperatively. The amniotic membrane has completely disappeared, and a ComfortRING is placed to maintain its function as a conformer. This corresponds to symblepharon discussed in the section “2. Main symptoms and clinical findings.”
Chronic conjunctival hyperemia, dryness, foreign body sensation, burning sensation, and tearing are the main complaints. These symptoms are resistant to standard dry eye treatment 1). In advanced cases, impaired eye movement due to symblepharon, incomplete eyelid closure, corneal irritation from trichiasis, and decreased visual acuity are added.
OCP is insidious and may be asymptomatic for a long time. Cases first discovered due to decreased visual acuity have also been reported 2).
Ocular surface keratinization, ankyloblepharon, severe dryness
In mild cases, linear or patchy white tendon-like tissue is seen on the palpebral conjunctiva. In severe cases, extensive scar formation and scar contraction lead to symblepharon, loss of the palisades of Vogt (POV), conjunctivalization of the cornea, dry eye, trichiasis, and entropion.
In cicatricial conjunctivitis confirmed by conjunctival biopsy, histological findings include stromal fibrosis, goblet cell loss, and squamous metaplasia 1).
The causes of cicatricial conjunctivitis are broadly classified as follows.
Autoimmune: In OCP, autoantibodies against integrins and laminin in the conjunctival basement membrane are formed, triggering chronic inflammation via a type II allergic reaction (autoimmune type II hypersensitivity) 5). Stevens-Johnson syndrome/toxic epidermal necrolysis occurs as a reaction to drugs (sulfonamides, antiepileptics, etc.). GVHD is a complication after hematopoietic stem cell transplantation, and ocular surface fibrosis can progress in the chronic phase 4). Rare cases of sarcoidosis causing cicatricial conjunctivitis have also been reported 3).
Drug-induced: Long-term use of antiglaucoma medications (e.g., pilocarpine, timolol, latanoprost) is typical 7). Frequent long-term use of eye drops containing preservatives (benzalkonium chloride) can also be a cause. Fibrosis tends to concentrate in the inferior fornix and medial canthal area 7).
Infectious: In developing countries, trachoma is the main cause of cicatricial conjunctivitis. In developed countries, severe cases of adenoviral keratoconjunctivitis can lead to scarring.
Traumatic: Includes chemical injuries from alkali or acid, thermal burns, and surgical damage.
A detailed history is essential. Inquire about ocular trauma, eye infections, and past and current medication use. Perform a systemic review for systemic inflammatory or autoimmune diseases, and conduct a physical examination of the mucous membranes, skin, and joints.
In OCP, evaluate for oral mucosal lesions (desquamative gingivitis, blistering lesions), esophageal lesions (dysphagia), and laryngeal/tracheal lesions (hoarseness, dyspnea) 2). Laryngeal stenosis is a potentially life-threatening complication.
Conjunctival biopsy is essential for definitive diagnosis. A specimen is taken from the inferior bulbar conjunctiva and subjected to histopathological examination with formalin fixation and direct immunofluorescence (DIF) using Michel’s medium 5).
In OCP, linear deposits of IgG, IgA, IgM, and complement C3 are observed in the conjunctival epithelial basement membrane zone 5). However, false negatives are not uncommon. Since OCP cannot be ruled out even with negative DIF, repeat biopsy should be considered if clinically suspicious 4).
In sarcoidosis, non-caseating epithelioid granulomas and Langhans giant cells are observed, which is useful for differentiation from OCP3).
The following tests are performed to investigate underlying diseases: ESR, CBC, CMP, ANA, SS-A/SS-B (Sjögren’s syndrome), ANCA (granulomatosis with polyangiitis), ACE/lysozyme (sarcoidosis).
QWhy can OCP not be ruled out even if conjunctival biopsy is negative?
A
False negatives in DIF testing are not uncommon. Causes include quiescent disease, complete loss of the basement membrane (end-stage), inappropriate biopsy site, and local variation in immune response. If OCP is clinically suspected, repeat biopsy should be performed, and multiple biopsies have been reported to improve sensitivity 4). Results may also differ between the right and left eyes 5).
Treatment is individualized according to the underlying disease. The goals are to halt progressive scarring, prevent and correct corneal and eyelid complications, and relieve symptoms.
OCP is a systemic disease, and systemic immunosuppressive therapy is the mainstay of treatment. Collaboration with rheumatology is strongly recommended 2).
Systemic Therapy
Mild to moderate inflammation: Dapsone (diaminodiphenyl sulfone) is first-line. G6PD deficiency must be excluded 5)
End-stage: Corneal prosthesis (Boston KPro type 2, OOKP)
Surgical treatment should be performed after inflammation is adequately controlled. Surgery in a state of insufficient inflammation control may lead to rapid deterioration 2).
Treatment of Drug-Induced Cicatricial Conjunctivitis
Discontinuation of the causative drug is the first and most important step 7). Topical steroids are used to control ocular surface inflammation. For glaucoma, intraocular pressure is managed with oral acetazolamide or switching to preservative-free eye drops, and surgery is considered if necessary 7).
Treatment of Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis
In the acute phase, immediate discontinuation of the causative drug and supportive therapy are fundamental. Ocular surface care includes preservative-free lubricants, topical antibiotics, topical steroids, and amniotic membrane transplantation. In the chronic phase, management of sequelae such as trichiasis, entropion, and corneal pannus is continued.
QWhat is the most important point in the treatment of pseudopemphigoid?
A
Discontinuation of the causative drug is most important. Long-term use of drugs with epithelial toxicity (especially antiglaucoma medications containing preservatives) is the cause, and inflammation improves rapidly by discontinuing all suspected drugs 7). After drug discontinuation, inflammation is controlled with topical steroids, and glaucomaintraocular pressure management is switched to oral medications or preservative-free eye drops.
The pathophysiology of cicatricial conjunctivitis varies depending on the causative disease, but the common final pathway is chronic conjunctival inflammation leading to fibrosis. Chronic inflammation causes infiltration of macrophages and monocytes into the conjunctiva, releasing growth factors that stimulate fibroblasts. Fibroblasts produce extracellular matrix, leading to progressive conjunctival fibrosis.
Pathophysiology of OCP: Autoantibodies are formed against integrins and laminins in the hemidesmosome-epithelial membrane complex of the conjunctival epithelial basement membrane 5). This activates the complement system, recruiting inflammatory cells and inducing chronic inflammation and fibrosis. In the acute phase, eosinophils and neutrophils mediate inflammation, while lymphocytes predominate in the chronic phase 5).
Corneal Epithelial Stem Cell Exhaustion: Corneal epithelial stem cells reside in the palisades of Vogt (POV). As cicatricial conjunctivitis progresses and the POV disappears, corneal epithelial stem cells become exhausted, leading to conjunctivalization, corneal opacity, and vascularization. In advanced stages, the corneal surface becomes keratinized like skin.
Combination of oGVHD and OCP: In GVHD after hematopoietic stem cell transplantation, mild conjunctival fibrosis is usually observed, but if severe and progressive cicatricial changes (symblepharon formation) occur, the possibility of OCP should be considered 4). Although oGVHD and OCP are clinically similar, their treatment strategies differ, so biopsy is important for differentiation 4).
QWhat is corneal epithelial stem cell exhaustion in cicatrizing conjunctivitis?
A
This refers to the loss of corneal epithelial stem cells located in the palisades of Vogt (POV) at the corneal limbus due to chronic inflammation and scarring. When stem cells are exhausted, normal corneal epithelial regeneration becomes impossible, and conjunctival epithelium invades the corneal surface (conjunctivalization). This results in corneal opacity, vascular invasion, and keratinization, leading to severe visual impairment. This condition is commonly seen after ocular cicatricial pemphigoid, Stevens-Johnson syndrome, and chemical injury.
Successful cases of minimally invasive glaucoma surgery (MIGS) using the XEN gel stent have been reported in OCP patients with glaucoma6). After controlling ocular surface inflammation, the stent was inserted via an ab interno approach, achieving intraocular pressure control without eye drops and inflammation remission at one year postoperatively 6). This case demonstrates that surgery is possible even in patients with severe ocular surface disease under appropriate preoperative management.
Cultured mucosal epithelial sheet transplantation is a new approach useful for preventing persistent epithelial defects and progression of symblepharon. Biologics such as rituximab and JAK inhibitors are attracting attention as treatment options for refractory OCP.
Farrag A, Chan A, Tong L. Cicatricial Conjunctivitis and Concurrent Clinical Features: A Case Study. Clinical medicine insights. Case reports. 2022;15:11795476221100605. doi:10.1177/11795476221100605. PMID:35601266; PMCID:PMC9121463.
Razzak A, Ait Ammar H, Bouazza M, Elbelhadji M. Accidental Discovery of Ocular Cicatricial Pemphigoid. Cureus. 2025;17(1):e77425. doi:10.7759/cureus.77425. PMID:39949452; PMCID:PMC11823481.
Murati Calderon RA, López-Fontanet JJ, Ramirez Marquez E, Tavares Reigada AS, Oliver A. Sarcoidosis: A Mimicker of Ocular Cicatricial Pemphigoid. Cureus. 2025;17(10):e93862. doi:10.7759/cureus.93862. PMID:41194826; PMCID:PMC12584608.
Taketani Y, Dehghani S, Sinha S, Freitag SK, Papaliodis G, Foster S, et al. Concurrence of Ocular Cicatricial Pemphigoid in Chronic Ocular Graft-Versus-Host Disease. Cornea. 2024;43(3):387-390. doi:10.1097/ICO.0000000000003386. PMID:38128104; PMCID:PMC12703942.
Tesorero JCC, Sosuan GMN, Lim Bon Siong R. Ocular Cicatricial Pemphigoid in a Healthy Elderly Male Filipino Patient. Acta Med Philipp. 2025;59(18):117-123.