LASIK is a refractive surgery in which a corneal flap approximately 100 μm thick is created under topical anesthesia, excimer laser is applied to the underlying corneal stroma, and the flap is repositioned. Flap complications are a general term for structural, inflammatory, and infectious disorders associated with flap creation, repositioning, and postoperative course.
After LASIK, complications such as flap abnormalities and diffuse lamellar keratitis (DLK) may occur, and early detection and appropriate management are important 1).
Flap complications are broadly divided by timing into intraoperative (during flap creation to repositioning) and postoperative (immediately after surgery to late phase). They can also be classified by pathology into structural, inflammatory, and epithelial types.
Flap creation devices include conventional microkeratomes and femtosecond lasers. Currently, most flaps are created with femtosecond lasers, which have improved flap accuracy and significantly reduced intraoperative complications such as free cap and irregular flaps. However, femtosecond laser-specific complications (e.g., OBL, vertical gas breakthrough) are also known.
SMILE is a procedure that creates a lenticule within the cornea without making a flap and removes it, thus avoiding complications associated with the LASIK flap itself. The absence of a flap is considered one of the safety advantages of SMILE2).
QDoes femtosecond laser eliminate flap problems?
A
The introduction of femtosecond lasers has significantly improved flap accuracy and markedly reduced microkeratome-specific issues such as free caps and irregular flaps. However, femtosecond laser-specific complications (e.g., opaque bubble layer [OBL], vertical gas breakthrough) can occur. Additionally, DLK, flap displacement, and epithelial ingrowth can still occur even with femtosecond lasers. Complications are not completely eliminated, and appropriate preoperative evaluation and intraoperative/postoperative management remain important.
Intraoperative flap complications are primarily related to the characteristics of the flap creation device. The complication profiles differ between microkeratome and femtosecond laser use. Timely recognition and management of intraoperative complications significantly affect final visual outcomes. Surgeons must be familiar with protocols for managing complications preoperatively and be prepared to make decisions without hesitation during surgery 1).
Microkeratome-Related
Incomplete flap: Incomplete incision due to keratome stopping mid-course. After flap repositioning, consider reoperation after 3–6 months.
Free cap: Complete separation of the flap without a hinge. The incidence with microkeratome is reported as 0.004–1.31% 3). If the stromal bed is smooth, proceed with laser ablation, then reposition the flap while keeping it moist with BSS and secure with a bandage contact lens.
Buttonhole: Perforation in the central flap. The incidence is reported as approximately 0.2% 3). Reposition the flap and postpone reoperation for 3–6 months.
Thin/thick/irregular flap: Deviation from the intended flap thickness. A flap that is too thin poses a risk of reduced corneal strength.
Femtosecond Laser-Related
OBL (opaque bubble layer): Bubbles generated during laser cutting that remain within the corneal stroma. Most resolve spontaneously, but invasion into the pupillary area may interfere with eye tracking.
Vertical gas breakthrough: Escape of gas bubbles from the incision plane toward the anterior chamber. Bubbles in the anterior chamber can cause a temporary increase in intraocular pressure.
Irregular flap edge: Irregular edges due to issues with laser parameter settings.
Spot cutting error: Incomplete flap deformation due to localized laser cutting failure.
When a free cap occurs, the surgeon must decide whether to continue or discontinue laser ablation. If the stromal bed is smooth, ablation can be continued. The free cap should be handled in a moist environment with BSS (balanced salt solution) drops to prevent deformation due to drying. After ablation is complete, the free cap is repositioned with the epithelial side up and in the correct orientation. Preoperative asymmetric markings are essential for confirming the correct orientation. If the stromal bed is irregular, the flap should be repositioned without laser ablation.
After repositioning, a bandage contact lens (BCL) is often placed. The endothelial pump function ensures firm readhesion of the cap. Keeping the eye closed with adhesive tape for about 30 minutes postoperatively is effective in preventing dislocation. A flat cornea (less than 40 D) and insufficient suction are major risk factors for free cap; preoperative corneal curvature measurement and appropriate suction ring selection are fundamental for prevention.
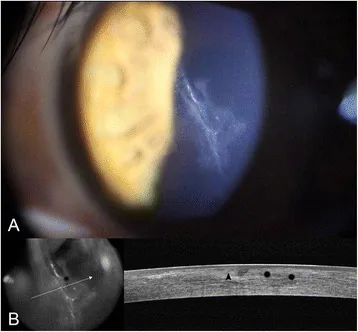
Inhibition of recurrence of epithelial ingrowth with an amniotic membrane pressure patch to a laser in situ keratomileusis flap with a central stellate laceration: a case report. BMC Ophthalmol. 2016 Jul 18;16:111. Figure 1. PMCID: PMC4950235. DOI: 10.1186/s12886-016-0291-4. License: CC BY 4.0.
Slit-lamp retroillumination image (A): A LASIK flap with a 5.0 mm vertical tear involving the central pupil is observed, with characteristic oblique bright line patterns in the corneal stroma indicative of flap displacement and wrinkles. Anterior segment OCT image (B): The tomographic image shows Bowman’s layer separation at the tear site (black arrowhead) and suspected epithelial ingrowth from the flap edge (black asterisk). This corresponds to flap displacement and flap wrinkles discussed in the section “Early Postoperative Flap Complications.”
Early postoperative flap complications (within 1 month after surgery) can be classified into three categories: structural, inflammatory, and epithelial-related.
Flap Structural Complications
Flap displacement: Occurs early postoperatively due to trauma or eye rubbing. Emergency flap lift, BSS irrigation, and repositioning are required. Particular caution is needed during the first postoperative week. The incidence is reported to be 0.1–0.3% within the first postoperative week4).
Flap striae/folds: Macrostriae (visible wrinkles) can affect visual function; if they do not decrease over time, early flap repositioning should be performed. Microstriae usually have little impact on visual function.
Inflammatory Complications
DLK (diffuse lamellar keratitis): Non-infectious interface inflammation under the flap. Punctate opacities are observed under the flap. The overall incidence in LASIK is reported to be approximately 0.1–1% 5). In Grade 1–2, frequent instillation of prednisolone 1% (or fluorometholone 0.1%) eye drops resolves most cases. In Grade 3–4, emergency flap lift and irrigation may be required.
Interface debris: Foreign material under the flap (from surgical instruments, talc, etc.). Usually harmless, but removal should be considered if located on the visual axis.
Epithelial-related complications
Epithelial ingrowth: Epithelial cells invade and proliferate at the interface from the flap edge. The incidence is reported to be 0.5–2% (up to 20% after enhancement) 6). Mild cases are observed. If progression exceeds 2 mm or visual acuity decreases, flap lift, scraping, and edge treatment are performed.
Flap edge epithelial defect: Epithelial irregularity or step at the flap edge. Most cases resolve with conservative treatment.
A four-grade classification based on the Linebarger/Goodman classification is used to determine treatment strategy 5).
Grade
Findings
Effect on vision
Treatment strategy
Grade 1
White granular infiltrates only in the periphery (central area normal)
Almost none
Frequent instillation of prednisolone 1% eye drops every 1–2 hours
Grade 2
Infiltration spreading toward the center
Mild decrease
Continue or increase steroid eye drops; re-evaluate the next day
Grade 3
Severe infiltration reaching the center, early signs of stromal melting
Moderate decrease
Continue steroid eye drops; strongly consider flap lift and irrigation
Grade 4
Central stromal melting (keratolysis) and scar formation
Marked decrease
Emergency flap lift and irrigation. Consider systemic steroid administration
QWhat happens if the flap is displaced?
A
If the flap is displaced in the early postoperative period, it can cause a sudden decrease in vision and irregular astigmatism. The cause is often trauma (rubbing the eye, impact during sports, etc.), and the first week after surgery is the highest risk period. If flap displacement is noted, urgent ophthalmologic evaluation is necessary. Treatment involves lifting the flap, irrigating the interface with BSS (balanced salt solution), accurately repositioning the flap, and fixing it with an air bubble. With appropriate management, vision often recovers, but if left untreated, the risk of irregular astigmatism and infection increases.
Flap-related problems occurring one month or more after surgery are classified as late postoperative complications.
Late flap displacement: Since the LASIK flap never fully heals even years after surgery, flap displacement can occur years later due to trauma (e.g., car accidents, direct ocular trauma during sports) 4). The principle of treatment is lift, wash, and reposition the flap as soon as displacement is recognized; the longer the delay, the higher the risk of epithelial ingrowth. Cases of trauma occurring five or more years postoperatively have been reported, emphasizing the importance of informing the attending physician about a history of refractive surgery from a patient education perspective 1).
Progression of late epithelial ingrowth: Mild epithelial ingrowth recognized early postoperatively may enlarge over several years, causing flap melting and irregular astigmatism. Enhancement surgery (re-treatment) is known to further increase the risk of epithelial ingrowth, and shorter follow-up intervals are recommended for eyes with a history of such surgery 6). The recurrence rate after flap lift and scraping is reported to be 5–20%, and additional procedures such as edge alcohol treatment or flap edge suturing (e.g., with Ethibond) are considered effective 6).
Persistent dry eye: Reflex tear secretion reduction due to corneal nerve transection after LASIK recovers in most cases within 6–12 months, but in some cases it persists as refractory dry eye7). Dry eye is one of the most common LASIK complications, and preoperative evaluation and postoperative treatment are important 1). Comparative studies of SMILE and FS-LASIK have shown that corneal nerve density recovers faster and tear parameters are less affected after SMILE7), which is a consideration in surgical technique selection.
Flap edge necrosis: As a rare complication, ischemic necrosis of the flap edge may occur. It is recognized on corneal topography as characteristic marginal undulation.
Postoperative ectasia (corneal ectasia): Corneal ectasia can develop postoperatively due to insufficient residual stromal bed (RST) after flap creation or the manifestation of pre-existing subclinical keratoconus. The prevalence of ectasia after LASIK is reported to be approximately 90 per 100,000 eyes 14), about 4.5 times that of PRK (approximately 20 per 100,000) 14). RST < 280 μm is a threshold for a sharp increase in ectasia risk, and percent tissue altered (PTA) ≥ 40% is also an independent risk factor 13). The Randleman scoring system enables preoperative risk stratification by comprehensively evaluating five factors: abnormal corneal topography, low RST, young age, thin cornea, and high myopia11).
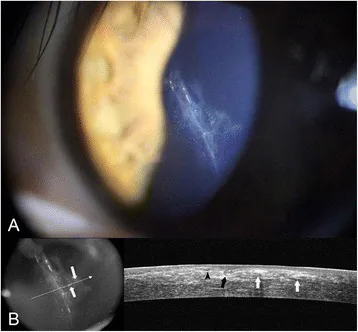
BMC Ophthalmol. 2016 Jul 18;16:111. Figure 2. PMCID: PMC4950235. DOI: 10.1186/s12886-016-0291-4. License: CC BY 4.0.
Slit-lamp photograph (A): Two weeks after LASIK, epithelial ingrowth and epithelial cysts (white arrows) are seen at the flap interface, with opacification spreading from the flap edge toward the center. OCT image (B): Tomography shows the tear edge of the flap and Bowman’s membrane (black arrowhead) and bending of the opposite flap edge (black arrow), confirming the depth of epithelial invasion into the interface. This corresponds to epithelial ingrowth discussed in the “Diagnosis and Management” section.
Standard practice includes slit-lamp examination the day after surgery to check for abnormalities, followed by follow-up for up to 6 months postoperatively 1).
Slit-lamp microscopy: Most important for diagnosis and monitoring of flap complications. Retroillumination is used to evaluate infiltration and interface conditions under the flap. In Grade 1–2 DLK, fine punctate infiltrates in the periphery are characteristic, and timely recognition of central spread is key for treatment decisions. Epithelial ingrowth appears as opacification extending inward from the flap edge; it is important to quantitatively record the distance (mm) from the edge to the center.
Anterior segment OCT (AS-OCT): Essential for evaluating flap thickness and residual stromal bed, confirming the depth and extent of epithelial ingrowth, and differentiating DLK from interface fluid syndrome (IFS). In IFS, a uniform low-reflectivity fluid layer is seen under the flap, while DLK shows predominantly punctate or linear high-reflectivity areas 8). AS-OCT also quantifies the degree of flap displacement (distance and depth), aiding in determining the urgency of treatment.
Corneal topography: Used to evaluate flap striae, irregular astigmatism, and ectasia. Serial postoperative observations can detect changes. After stromal melting due to Grade 4 DLK, it is important to assess posterior elevation changes using tomography (e.g., Pentacam) to evaluate for ectasia development.
Corneal culture and smear: If infection under the flap is suspected (e.g., anterior chamber inflammation, hyperemia, dense infiltrates, purulent discharge from the flap edge), cultures should be obtained during flap lift to identify the organism and drug sensitivity. Infectious keratitis can clinically resemble DLK, so early microbiological investigation is essential when suspected.
Protect with BSS, accurate repositioning after ablation, BCL fixation
Intraoperative management
Incomplete flap / buttonhole
Flap repositioning, surgery postponed
Consider reoperation after 3–6 months
QWhat to do if DLK is diagnosed?
A
Treatment strategy differs by DLK grade (severity). For Grade 1–2, treat with prednisolone 1% eye drops every 1–2 hours. Most cases improve with this steroid eye drop therapy. For Grade 3, consider flap lift and irrigation in addition to the above. Grade 4 (central stromal melting) requires urgent flap lift and irrigation, and systemic steroids may also be considered. Do not self-judge; if you notice flap opacity or vision loss after surgery, contact your ophthalmologist promptly.
The incidence of flap complications varies greatly depending on the surgical technique (microkeratome vs. femtosecond laser), facility experience, and patient selection criteria. The incidence rates obtained from major literature are shown below3)12).
With the widespread use of femtosecond lasers, severe intraoperative complications such as free caps and buttonholes have significantly decreased. However, it is important to note that DLK, flap displacement, and epithelial ingrowth can still occur even with femtosecond lasers 12).
Impact of flap-related complications on postoperative visual acuity
DLK Grade 3–4, severe epithelial ingrowth with flap melting, and large-area flap wrinkles can cause permanent vision loss if appropriate treatment is delayed. In an epidemiological study by Stulting et al. 12), approximately 0.1% of DLK cases progressed to stromal melting (Grade 4), and even with appropriate treatment, some residual irregular astigmatism has been reported. Daily or every-other-day examinations within the first postoperative week are recommended after LASIK during the high-risk early period 1).
A LASIK flap is created by making a lamellar incision approximately 100 μm deep from the anterior corneal surface using a microkeratome or femtosecond laser. The femtosecond laser forms the incision plane through photodisruption, creating plasma and a linear array of microbubbles. The microkeratome cuts mechanically. In cases with corneal opacity or after radial keratotomy (RK), a microkeratome may be used, or PRK may be selected.
DLK is a noninfectious interface inflammatory reaction. Corneal stromal debris, residues from surgical instruments, and epithelial irritants induce polymorphonuclear leukocyte infiltration at the flap interface. It often resolves spontaneously with transient inflammation, but progression to Grade 4 causes stromal melting (keratolysis), leading to permanent irregular astigmatism. Early detection and intervention during examinations within 1–3 days postoperatively determine the prognosis.
Epithelial cells at the flap margin invade and proliferate beneath the flap interface. The invading epithelial cells form cell nests under the flap, and as they enlarge, they cause flap melting, irregular astigmatism, and decreased visual acuity. The risk increases after enhancement surgery involving flap lift. Flap edge position and a history of previous surgery are risk factors 6).
After LASIK, the flap does not fully regain adhesion to the corneal stroma and contributes little to the structural strength of the cornea. The thicker the flap, the thinner the residual stromal bed (RST), leading to a greater impact on corneal biomechanics9). Thinning of the residual stromal bed is associated with an increased risk of corneal ectasia, with risk rising sharply when RST < 280 μm 2). LASIK results in greater corneal biomechanical vulnerability compared to SMILE, as reported by a significantly greater reduction in Corneal Resistance Factor (CRF) at 12 months postoperatively (MD, −1.13; 95% CI −1.36 to −0.90; P < 0.001) 2).
Finite element analysis simulation studies have quantitatively demonstrated the impact of flap thickness on biomechanics 9). As flap thickness increases, the forward displacement of the posterior corneal surface increases, indicating that thinner flaps are more favorable for posterior surface stability. However, excessively thin flaps pose challenges in manufacturing precision (e.g., irregularity, OBL). Femtosecond lasers can create flaps with ±10 μm accuracy, allowing safe creation of thin flaps around 100–120 μm, and a design balancing biomechanics and reliable flap creation is recommended. The absolute value of the postoperative residual stromal bed (RST) is the most important indicator for ectasia risk assessment in LASIK, and it is recommended to reconsider surgical indications when RST < 280 μm 2)15).
The closed space under the flap requires management different from that of typical corneal infections. Antibiotic eye drops must be selected according to the causative organism, and in severe cases, flap lift and irrigation are performed. Prevention requires strict adherence to high-level barrier precautions, instrument sterilization, and surgical field disinfection and draping 1).
Interface fluid syndrome (IFS) is fluid accumulation under the flap caused by steroid-induced intraocular pressure elevation, and differentiating it from DLK is a critical issue that changes the treatment strategy by 180 degrees. IFS presents with elevated intraocular pressure (caution: Goldmann applanation tonometry may show falsely low values), and anterior segment OCT reveals a homogeneous hyporeflective fluid layer. Since continued steroid administration worsens IFS, differentiation using anterior segment OCT and intraocular pressure measurement is essential 8). Late-onset IFS can occur months to years after surgery; if fluid under the flap is observed, intraocular pressure measurement (especially with peripheral or dynamic contour tonometry) must be performed 8).
Surgical technique improvements in femtosecond laser LASIK
Modifications of the flap creation angle (vertical and horizontal bevel angles) and adjustments of the flap hinge width and angle have improved flap security and reduced the risk of postoperative flap displacement. In particular, there are reports that a superior hinge provides better postoperative stability than a nasal hinge 10). Some opinions suggest that designing the flap edge with an acute side-cut angle (side-cut angle ≥90°) reduces the risk of epithelial ingrowth at the margin 10). Additionally, flap thickness uniformity is better with femtosecond laser than with microkeratome, and finite element analysis has quantified the impact of flap thickness on biomechanics 9).
Transition to SMILE and avoidance of flap complications
Since SMILE does not create a flap, LASIK flap-specific complications such as flap displacement, free cap, and buttonhole are avoided. The incidence of postoperative ectasia has been reported to be lower with SMILE than with LASIK 2). However, SMILE also has its own complications, such as interface inflammation (DLK-like), lenticule remnants, and capsulectomy.
Corneal cross-linking (CXL) for post-LASIK ectasia
When postoperative ectasia progresses, corneal cross-linking (CXL) is the first-line treatment. The Dresden protocol, which involves instillation of 0.1% riboflavin followed by UVA irradiation (3 mW/cm² for 30 minutes), is the standard method and halts progression in most cases 15). Accelerated CXL (9 mW/cm² for 10 minutes) can shorten treatment time 15). The efficacy of CXL for post-LASIK ectasia tends to be slightly lower than that for keratoconus, but early intervention improves prognosis 15). In Japan, CXL has been covered by insurance since 2022. It is important to maximize prevention of ectasia onset through preoperative risk assessment using the Randleman scoring system 11) and preoperative screening recommended by the AAO Corneal Ectasia PPP 17).
It is important to monitor the DLK incidence rate at the facility level and recognize cluster occurrences (multiple cases concentrated in a short period). Cluster occurrences often suggest contaminants in the operating room, inadequate sterilization of instruments, or issues with cleaning solutions 16). If the incidence rate exceeds 0.5%, a comprehensive inspection of the operating room, instruments, and cleaning solutions is recommended.
Wang Y, Xie L, Yao K, Sekundo W, Alió JL, Mehta JS, Goel S, Elmassry A, Schallhorn J, Shilova T, Cao H, Xu L, Chen X, Zhang F, Bai J, Zhang W, Liu Q, Zhou X, Chen Y, Wang Z, Jhanji V, Yang K, Writing Committee for the Guideline Working Group. Evidence-Based Guidelines for Keratorefractive Lenticule Extraction Surgery. Ophthalmology. 2025;132(4):397-419. doi:10.1016/j.ophtha.2024.11.016. PMID:39577672.
Sahay P, Bafna RK, Reddy JC, Vajpayee RB, Sharma N. Complications of laser-assisted in situ keratomileusis. Indian J Ophthalmol. 2021 Jul;69(7):1658-1669. doi:10.4103/ijo.IJO_1872_20. PMID:34146007; PMCID:PMC8374806.
Ursea R, Feng MT, Zhou M, Cain W, Weikert MP. Temporal analysis of LASIK flap displacement presenting as late complication. Clin Ophthalmol. 2011;5:1535-1538.
Johnson JD, Harissi-Dagher M, Pineda R, et al. Diffuse lamellar keratitis: incidence, associations, outcomes, and a new classification system. J Cataract Refract Surg. 2001;27(10):1560-1566. doi:10.1016/s0886-3350(01)00958-0.
Jabbur NS, Chicani CF, Kuo IC, O’Brien TP. Risk factors in interface epithelial ingrowth after LASIK. J Refract Surg. 2004;20(4):343-348.
Recchioni A, Sisó-Fuertes I, Hartwig A, Hamid A, Shortt AJ, Morris R, et al. Short-Term Impact of FS-LASIK and SMILE on Dry Eye Metrics and Corneal Nerve Morphology. Cornea. 2020;39(7):851-857. doi:10.1097/ICO.0000000000002312. PMID:32243424.
Vera-Duarte GR, Guerrero-Becerril J, Müller-Morales CA, Ramirez-Miranda A, Navas A, Graue-Hernandez EO. Delayed-onset pressure-induced interlamellar stromal keratitis (PISK) and interface epithelial ingrowth 10 years after laser-assisted in situ keratomileusis. American journal of ophthalmology case reports. 2023;32:101874. doi:10.1016/j.ajoc.2023.101874. PMID:38161519; PMCID:PMC10757168.
Fang L, Wang Y, Yang R, Deng S, Deng J, Wan L. Effects of the LASIK flap thickness on corneal biomechanical behavior: a finite element analysis. BMC ophthalmology. 2020;20(1):67. doi:10.1186/s12886-020-01338-8. PMID:32093676; PMCID:PMC7038569.
Stephen G Slade. The use of the femtosecond laser in the customization of corneal flaps in laser in situ keratomileusis. Current Opinion in Ophthalmology. 2007;18(4):314-317. doi:10.1097/icu.0b013e3281bd88a0.
Randleman JB, Woodward M, Lynn MJ, Stulting RD. Risk assessment for ectasia after corneal refractive surgery. Ophthalmology. 2008 Jan;115(1):37-50.e4. doi:10.1016/j.ophtha.2007.03.073. PMID:17624434.
Stulting RD, Randleman JB, Cowan LA, Thompson KP, Bradley EV, Lynn MJ. The epidemiology of diffuse lamellar keratitis. Cornea. 2004;23(7):680-688. doi:10.1097/01.ico.0000127477.14304.de.
Santhiago MR, Smadja D, Gomes BF, et al. Association between the percent tissue altered and post-LASIK ectasia in eyes with normal preoperative topography. Am J Ophthalmol. 2014;158:87-95.e1. doi:10.1016/j.ajo.2014.04.002. PMID:24727263.
Moshirfar M, Tukan AN, Bundogji N, Liu HY, McCabe SE, Ronquillo YC, et al. Ectasia After Corneal Refractive Surgery: A Systematic Review. Ophthalmology and therapy. 2021;10(4):753-776. doi:10.1007/s40123-021-00383-w. PMID:34417707; PMCID:PMC8589911.
Hersh PS, Stulting RD, Muller D, Durrie DS, Rajpal RK, U.S. Crosslinking Study Group. U.S. Multicenter Clinical Trial of Corneal Collagen Crosslinking for Treatment of Corneal Ectasia after Refractive Surgery. Ophthalmology. 2017;124(10):1475-1484. doi:10.1016/j.ophtha.2017.05.036. PMID:28655538.
Linebarger EJ, Hardten DR, Lindstrom RL. Diffuse lamellar keratitis: diagnosis and management. Journal of cataract and refractive surgery. 2000;26(7):1072-7. doi:10.1016/s0886-3350(00)00468-5. PMID:10946202.
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.