Diffuse lamellar keratitis (DLK) is a non-infectious diffuse inflammatory reaction that occurs at the interface between the flap and the corneal stromal bed after LASIK surgery. It is characterized by fine white granular infiltrates scattered under the flap, described as “Sands of Sahara.”
DLK is a postoperative complication to be aware of after both excimer laser surgery and SMILE1). The overall incidence in LASIK is reported to be approximately 0.1-1% 2). Even in recent years when femtosecond laser flap creation has become mainstream, DLK occurs at a certain frequency, and DLK-like interface inflammation is also observed after SMILE surgery. The overall incidence of DLK after SMILE is reported to be 0.84%, with Grade I (peripheral localized) at 1.42%, Grade II (central extension) at 0.29%, Grade III (confluent/focal) at 0.08%, and Grade IV (severe) at 0.02% 3).
This condition is fundamentally different from infectious keratitis in that bacteria are not involved. On the other hand, distinguishing it from IFS (Interface Fluid Syndrome/PISK), an inflammatory disease with a similar appearance, is the most important clinical challenge because the treatment approach changes 180 degrees.
QAfter what type of surgery does DLK occur?
A
DLK most commonly occurs after LASIK surgery, but it can also occur after SMILE (Small Incision Lenticule Extraction). Both excimer laser surgery and SMILE require attention as a postoperative complication. PRK does not involve creating a flap, so its pathology differs from typical flap-associated DLK. Even after the widespread use of femtosecond lasers, DLK has not been eliminated; meticulous observation from postoperative days 1 to 5 and early intervention are key to a good prognosis. In particular, early detection of Grade 1–2 and prompt initiation of steroid therapy are most important to prevent progression to Grade 3–4. Note that PRK carries a risk of postoperative haze (subepithelial opacity), and prophylactic treatment with mitomycin C may be administered. Individualized patient explanations based on a thorough understanding of the surgical technique are required.
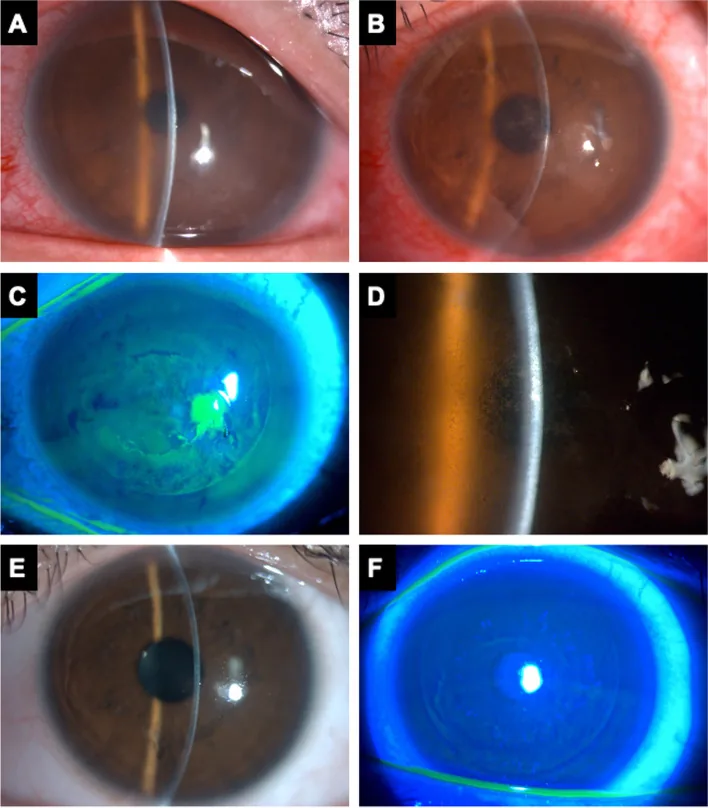
Lin H-Y, Ho W-T. Diffuse lamellar keratitis as a rare complication of diamond burr superficial keratectomy for recurrent corneal erosion: a case report. BMC Ophthalmol. 2022;22:362. Figure 2. PMCID: PMC9450270. License: CC BY 4.0.
Stage 3 DLK diagnosed on postoperative day 2 after LASIK: Slit-lamp microscopy and external photographs (A) Mild corneal edema and ciliary injection, (B–D) “Sahara sand”-like granular white infiltration spreading across the flap interface including the visual axis, (E–F) Resolution of infiltration after steroid eye drop treatment. Corresponds to the slit-lamp microscopy findings (granular infiltration, Grade classification) discussed in the “Main Symptoms and Clinical Findings” section.
The subjective symptoms of DLK depend on the severity (Grade).
Grade 1–2: Mild photophobia and decreased vision. May be asymptomatic. Visual acuity is usually maintained at 0.8 or better.
Grade 3: Clear decrease in vision (0.5–0.7), eye pain, and photophobia. Persistent blurred vision.
Grade 4: Severe decrease in vision (less than 0.5), intense eye pain, and photophobia. Marked blurred vision due to stromal melting. Rapid progression may occur from Grade 3 within 24 hours.
The typical onset is 1–5 days postoperatively, and it is thought that inflammatory mediators accumulate and manifest shortly after flap creation. However, late-onset cases occurring weeks to months after surgery have also been reported, and some cases recur when steroid eye drops are discontinued.
Retroillumination observation with a slit-lamp microscope provides the most important findings for diagnosing DLK. When observed with retroillumination, light comes from behind, making it easier to assess the status of cellular infiltration under the flap. Beginners may find the description “sandstorm-like appearance” intuitively difficult to understand, but with experience, it becomes recognizable as a very characteristic finding. In Grade 1 to 2, granular infiltration is mainly distributed in the periphery, and in Grade 2 or higher, infiltration progresses toward the center. The term “Sands of Sahara” is used as a clinical expression that accurately describes the spread of fine white granular infiltration.
Slit-lamp microscope findings
Granular infiltration: Fine white to gray-white granular infiltration scattered under the flap, resembling a “sand-like” appearance.
Distribution changes: Grade 1 is predominantly peripheral. Grade 2 or higher progresses toward the center.
Border characteristics: Lesions have indistinct borders and tend to spread from the flap edge toward the center.
Anterior chamber inflammation: Anterior chamber inflammation is usually mild or absent. If anterior chamber inflammation is severe, priority should be given to differentiating from infectious keratitis.
Anterior segment OCT findings
Hyperreflective areas: Punctate to linear hyperreflective areas are observed at the flap interface.
No flap dehiscence: Unlike IFS, physical dehiscence or fluid accumulation of the flap is not observed (except in Grade 4).
Monitoring of stromal melting: In Grade 3 to 4, anterior segment OCT can be used to evaluate the melting status of the stromal bed over time.
Differentiation from IFS: In IFS, a uniform fluid layer (hyporeflective band) is observed under the flap, whereas in DLK, punctate hyperreflective areas are predominant.
Multiple triggers are involved in the onset of DLK. All share a common mechanism: “inflammatory substances are enclosed in the closed space under the flap.”
Endogenous triggers:
Corneal stromal ablation debris and collagen fragments generated during flap creation.
Inflammatory cytokines derived from epithelial cells (IL-1, TNF-α, etc.) and lipid degradation products
Stimulatory substances from plasma formation and microbubbles generated by femtosecond laser
When limbal epithelial tissue is entrapped at the incision edge
Exogenous triggers:
Residual metal microparticles from surgical instruments (microkeratome, spatula)
Foreign substances such as glove talc or silicone oil
Corneal epithelial damage due to preservatives in preoperative eye drops (e.g., benzalkonium chloride)
Residues of chemicals used in sterilization (glutaraldehyde, hydrogen peroxide, etc.)
Impurities in irrigation solutions or BSS (e.g., endotoxin contamination)
Environmental and facility factors:
Cluster outbreaks of DLK (multiple cases occurring in a short period within a facility) often suggest contaminants in the operating room (volatile organic compounds, endotoxins, etc.)6). Monitoring the overall DLK incidence rate at the facility is important to identify the cause and implement environmental improvements. Associations with specific lots of cleaning agents, sterilization solutions, or eye drops have been reported.
Infectious inflammation (bacterial, fungal, Acanthamoeba) is excluded by definition from DLK, but infection can trigger a DLK-like reaction.
Factors affecting incidence:
Device: No significant difference in incidence between femtosecond laser and microkeratome2)
Surgeon experience: Incidence tends to be higher during the early learning curve
Preoperative eye drops: Use of BAK-free formulations may reduce ocular surface inflammation and lower DLK risk
Patient factors: Atopic predisposition and preoperative ocular surface inflammation increase the risk of occurrence.
IFS is fluid accumulation under the flap caused by steroid-induced intraocular pressure elevation, without inflammatory cells, and the core issue is elevated intraocular pressure. If DLK is misdiagnosed as IFS and steroid administration is continued, intraocular pressure rises further, worsening IFS4). Conversely, if IFS is misdiagnosed as DLK and steroids are withheld, DLK progresses to corneal stromal melting.
Discontinue steroids + use intraocular pressure-lowering medications
Differential diagnosis from infectious keratitis:
Infectious keratitis (bacterial, fungal, Acanthamoeba) often presents with anterior chamber inflammation. Stromal inflammation caused by highly virulent bacteria or fungi may show fibrin exudation in the anterior chamber. Non-infectious keratitis (including DLK) usually has mild anterior chamber inflammation. If localized infiltration, hyperemia, or discharge is severe, suspect infection.
Slit-lamp microscopy is performed on the first postoperative day, and the frequency of observation is adjusted according to the severity of DLK management 1).
Postoperative day 1 (next day): Examine the interface with slit-lamp microscopy and determine the presence and grade of DLK. If Grade 1–2 is observed, start or increase steroid eye drops and instruct the patient to return the next day.
Postoperative days 2–5 (suspected DLK): After starting steroid eye drops, re-evaluate daily or every other day to monitor grade changes. If progression from Grade 2 to 3 is noted, perform immediate flap lift and irrigation.
Postoperative day 7: Confirm improvement of DLK. If Grade 1 or lower, begin gradual tapering of steroid eye drops.
Postoperative day 14 and beyond: Continue intraocular pressure monitoring during steroid tapering, and prepare for transition to IFS.
Most Grade 1–2 DLK completely resolves within two weeks after surgery, but Grade 3–4 may leave permanent irregular astigmatism due to stromal melting, so follow-up with corneal topography analysis for 3–6 months after treatment completion is recommended 9).
QHow do you differentiate DLK from IFS?
A
The most important point in differentiating DLK from IFS (interface fluid syndrome) is intraocular pressure. In IFS, intraocular pressure is elevated, but central measurement with Goldmann applanation tonometry may show falsely low values due to the fluid cushion effect, so peripheral measurement or dynamic contour tonometry is recommended. On anterior segment OCT, DLK is characterized by punctate hyperreflective areas, while IFS shows a uniform hyporeflective fluid layer lifting the flap. DLK presents with pain and white granular infiltrates in the early postoperative period (1–5 days), whereas IFS primarily presents with blurred vision and elevated intraocular pressure without inflammatory cells. Because treatments are completely opposite (DLK → increase steroids, IFS → stop steroids + lower intraocular pressure), misdiagnosis leads to serious consequences.
Frequent instillation of steroid eye drops is the first-line treatment.
Prednisolone 1% (e.g., Prednisolone ophthalmic solution): Instilled every 1–2 hours. Efficacy is assessed within 24 hours. Antibiotic eye drops (e.g., fluoroquinolones) are often added concurrently.
Fluorometholone 0.1–0.5%: Lower risk of intraocular pressure elevation than prednisolone, but less effective; therefore, switching to prednisolone 1% is recommended for progressive Grade 2 cases.
For Grade I after SMILE, fluorometholone 6–8 times/day is standard 3).
Re-evaluate the next day to confirm grade improvement. If no improvement in Grade 2, consider flap lift the following day.
Measure intraocular pressure regularly during steroid eye drop administration to prepare for possible transition to IFS. In particular, steroid responders may experience rapid IOP elevation; re-measurement of IOP 3–5 days after starting treatment is recommended.
For Grade 2, peripheral IOP measurement using a Tono-Pen or similar device, in addition to Goldmann applanation tonometry, is useful to avoid falsely low values 4).
While continuing steroid eye drops, strongly consider flap lift and irrigation with balanced salt solution.
Flap lift (reopening): Carefully elevate the flap using a dedicated spatula. If adhesions remain at the flap edge, bluntly dissect to expose the interface.
Irrigation with BSS (balanced salt solution): Thoroughly irrigate the interface using a 30 mL BSS syringe to physically remove inflammatory cells, debris, and inflammatory mediators such as MMPs.
Flap repositioning: After irrigation, accurately reposition the flap, confirm air bubbles and interface uniformity, then close the eye.
Enhanced postoperative steroid eye drops: After flap lift, continue frequent administration of prednisolone 1% eye drops every 1–2 hours, and reassess the next day.
Eye patch management: After flap lift, consider using a BCL (bandage contact lens) to assist flap re-fixation.
For Grade III in SMILE, consider interface irrigation in addition to high-dose steroids 3). Interface irrigation after SMILE is more difficult to access than after LASIK, so it should be performed by an experienced surgeon.
Some facilities perform interface injection of dexamethasone 0.1% in addition to BSS irrigation (evidence is limited).
Consider short-term systemic steroids (oral prednisolone 0.5–1 mg/kg/day). Limit use to 1–2 weeks with tapering to manage side effects.
For Grade IV in SMILE, steroid interface irrigation is mandatory, and systemic steroids should also be added 3).
Since stromal melting often has already progressed in Grade 4, monitor the interface and extent of stromal melting over time with anterior segment OCT after flap lift and irrigation, and confirm no residual progression of melting.
If melting reaches deep or central areas, explain future options such as corneal transplantation (PTK, keratoplasty, corneal transplant) to the patient.
Consider flap lift if progression to Grade 2 or higher
2
Same as above, increase dose. Confirm at next day visit
Next day
If no improvement, flap lift the next day
3
Steroid eye drops + flap lift and irrigation
Same day to next day
Flap lift performed in principle
4
Emergency flap lift and irrigation (consider systemic steroids)
Same day emergency
Immediate intervention
QWhat should I do if I am diagnosed with DLK?
A
Treatment for DLK varies by grade. For Grade 1–2, treatment involves frequent instillation of prednisolone 1% ophthalmic solution every 1–2 hours. Most cases improve within 1–2 weeks with this treatment. For Grade 3, in addition to eye drops, flap lift (reopening the flap) and saline irrigation may be necessary. Grade 4 (stromal melting) requires urgent flap lift and irrigation, and systemic steroids may also be considered. Do not discontinue eye drops on your own; if you experience decreased vision or severe photophobia after surgery, contact your doctor immediately.
6. Pathophysiology and Detailed Mechanism of Onset
DLK is a non-infectious inflammatory reaction primarily involving polymorphonuclear leukocytes (neutrophils). When debris from flap creation, particles from surgical instruments, or biological irritants become trapped in the closed space of the corneal interface, local production of cytokines (IL-1β, IL-6, TNF-α, etc.) and chemokines (IL-8, MCP-1, etc.) occurs, leading to neutrophil accumulation. Unlike infectious inflammation, this inflammatory reaction does not involve bacterial or fungal proliferation.
Because the flap does not fully re-adhere after surgery, the interface functions as a semi-closed space. This structural characteristic of “containing” inflammatory cells and mediators limits the localization of DLK to the area under the flap.
Since the lumen of the flap interface has limited contact with the normal corneal stroma, the recruitment pathway for neutrophils is thought to primarily involve the limbal vascular network and existing cells within the corneal stroma (keratocytes and Langerhans cells). The speed of progression from onset to severe disease (Grade 1 to 4) varies greatly among individuals; in some cases, rapid progression to Grade 4 can occur within 1–2 days postoperatively. This is why meticulous observation during the first few days after surgery is absolutely essential for managing DLK.
Mechanism of Corneal Stromal Melting (Keratolysis)
In severe DLK (Grade 4), large amounts of matrix metalloproteinases (MMP-8, MMP-9, etc.) derived from neutrophils are released, breaking down collagen fibers and causing corneal stromal melting. If melting reaches the central area, it can lead to permanent vision loss and irregular astigmatism. Early intervention (flap lift and irrigation) to physically remove MMP-producing neutrophils is a key rationale for preventing progression of melting.
Pathologically, DLK shows accumulation of inflammatory polymorphonuclear leukocytes and mononuclear cells between layers, whereas IFS lacks inflammatory cells and shows only stromal edema 4). This pathological difference is the fundamental basis for distinguishing the treatment strategies for the two conditions.
Femtosecond laser flap creation improves flap accuracy compared to microkeratomes, but laser-induced opaque bubble layer (OBL) formation can cause transient interface reactions. Plasma formation and microbubbles from photodisruption may trigger local inflammatory responses 5). Although a specific increase in DLK associated with femtosecond lasers has not been consistently demonstrated, distinguishing between OBL-related inflammation and DLK is considered important.
OBL occurs in 10–30% of cases with femtosecond laser use and typically resolves spontaneously within hours to days postoperatively. However, extensive OBL can interfere with excimer laser eye tracking and reduce ablation accuracy, so if detected during surgery, waiting for resolution is common. OBL itself is not thought to cause inflammation, but when OBL and DLK are observed simultaneously, retroillumination is particularly useful for assessing DLK progression.
DLK after SMILE occurs in the interface beneath the cap (equivalent to the flap), and the same pathophysiology and treatment principles as LASIK apply 3). However, because instruments are inserted through a 2–3 mm small incision, interface irrigation is more difficult than in LASIK. With appropriate steroid treatment, lesions improve within one week in most cases, and symptoms reportedly resolve in about three weeks 3).
The incidence of DLK after SMILE (0.84%) is generally similar to that after LASIK (0.1–1%), suggesting that the presence of a flap/cap interface, rather than the specific procedure, is a common trigger. While SMILE does not involve flap-related complications (e.g., flap dislocation, free cap), similar caution is required in DLK management, and observation on postoperative days 1–5 is particularly important. Interface irrigation for Grade 3–4 DLK after SMILE should be performed only by surgeons with sufficient experience in SMILE postoperative management 3).
DLK is a complication of refractive surgery in which early diagnosis and appropriate treatment can significantly improve visual outcomes. Establishing a meticulous early postoperative observation schedule and thoroughly instructing patients to seek early care if symptoms worsen are fundamental and most important management strategies to prevent vision loss due to DLK.
The incidence of DLK is known to be reduced by improvements in the surgical environment. Specifically, quality control of irrigation fluids (purity of distilled water, BSS, etc.), changing surgical gloves (use of talc-free gloves), enhanced ultrasonic cleaning of instruments, and maintaining positive pressure in the operating room to prevent endotoxin contamination are considered important 6). Continuous monitoring of DLK incidence at the facility level is essential for identifying causes and developing countermeasures.
A 2022 review in the Brazilian Archives of Ophthalmology proposed an extended classification to complement the existing Grade 1–4 system, introducing concepts such as fibrotic response (Grade 5) and a severe type with anterior chamber infiltration (equivalent to Grade 6)7). However, the current international consensus still considers the Grade 1–4 classification as the standard.
Some reports suggest that using topical steroids (e.g., prednisolone) before or during surgery may reduce the incidence of DLK8). However, patients with high steroid sensitivity are at risk of increased intraocular pressure, so individual risk assessment is necessary.
Overview of DLK as a Complication After Refractive Surgery
DLK is a representative condition among post-refractive surgery complications that requires diagnostic and therapeutic decision-making. In a review by Swanson et al.9), the incidence, risk factors, and treatment outcomes of DLK, epithelial ingrowth, and flap-related complications after refractive surgery were summarized, confirming that DLK is the most frequent complication (0.1–1% after LASIK). A review by Phipps et al.10) systematically organized the latest evidence on the pathophysiology, grading, differential diagnosis, and treatment of DLK, emphasizing that Grade 1–2 cases recover in over 90% with conservative treatment, while for Grade 3–4, early flap lift and irrigation are critical for visual prognosis.
In a review of flap complications by Moshirfar et al.11), it was shown that DLK occurs at similar frequencies with both microkeratomes and femtosecond lasers, and the presence of the flap interface itself is discussed as a necessary condition for DLK. The possibility that femtosecond laser-specific opaque bubble layer (OBL) formation may trigger DLK onset is also examined11).
Venkataraman et al.12) reported a case series of late-onset IFS, including cases developing more than 10 years after LASIK, demonstrating that IFS can occur at any time after LASIK. They showed that intraocular pressure measurement (using peripheral measurement or dynamic contour tonometry) and anterior segment OCT are essential for differential diagnosis12).
Customization of Femtosecond Laser and Its Impact on DLK
Slade13) discusses the impact of femtosecond laser flap customization (flap thickness, hinge angle, side-cut angle) on flap security and the complication profile, showing that appropriate flap design (uniform thickness, appropriate hinge width, acute side-cut angle) contributes to reducing postoperative flap displacement and DLK incidence13).
Randleman et al.14) identified five factors—corneal topographic abnormality, low residual stromal thickness, young age, thin cornea, and high myopia—as predictors of postoperative ectasia in their ectasia risk scoring system. Although ectasia and DLK are independent complications, when stromal melting occurs in Grade 3–4 DLK, the structural vulnerability of the cornea increases, potentially raising the risk of latent ectasia14).
Corneal Ectasia PPP and Positioning of DLK Management
The AAO Corneal Ectasia PPP15) recommends CXL (corneal cross-linking) as the first-line treatment for managing postoperative ectasia, and indicates that CXL may be considered even in cases where stromal melting due to DLK has progressed. However, CXL is indicated only when progression is confirmed; DLK alone is not an indication for CXL15).
Johnson JD, Harissi-Dagher M, Pineda R, et al. Diffuse lamellar keratitis: incidence, associations, outcomes, and a new classification system. J Cataract Refract Surg. 2001;27(10):1560-1566. doi:10.1016/s0886-3350(01)00958-0.
Wang Y, Xie L, Yao K, Sekundo W, Alió JL, Mehta JS, Goel S, Elmassry A, Schallhorn J, Shilova T, Cao H, Xu L, Chen X, Zhang F, Bai J, Zhang W, Liu Q, Zhou X, Chen Y, Wang Z, Jhanji V, Yang K, Writing Committee for the Guideline Working Group. Evidence-Based Guidelines for Keratorefractive Lenticule Extraction Surgery. Ophthalmology. 2025;132(4):397-419. doi:10.1016/j.ophtha.2024.11.016. PMID:39577672.
Vera-Duarte GR, Guerrero-Becerril J, Müller-Morales CA, Ramirez-Miranda A, Navas A, Graue-Hernandez EO. Delayed-onset pressure-induced interlamellar stromal keratitis (PISK) and interface epithelial ingrowth 10 years after laser-assisted in situ keratomileusis. American journal of ophthalmology case reports. 2023;32:101874. doi:10.1016/j.ajoc.2023.101874. PMID:38161519; PMCID:PMC10757168.
Kymionis GD, Naoumidi TL, Aslanides IM, Pallikaris IG, Siganos CS. Diffuse lamellar keratitis after laser in situ keratomileusis with the IntraLase femtosecond laser. J Cataract Refract Surg. 2007;33(8):1471-1473.
Stulting RD, Randleman JB, Cowan LA, Thompson KP, Bradley EV, Lynn MJ. The epidemiology of diffuse lamellar keratitis. Cornea. 2004;23(7):680-688. doi:10.1097/01.ico.0000127477.14304.de.
Rosa DS, de Macedo ELS, Leal LA, et al. Diffuse lamellar keratitis after LASIK: literature review and proposed new grading. Arq Bras Oftalmol. 2022;85(2):198-204.
Linebarger EJ, Hardten DR, Lindstrom RL. Diffuse lamellar keratitis: diagnosis and management. Journal of cataract and refractive surgery. 2000;26(7):1072-7. doi:10.1016/s0886-3350(00)00468-5. PMID:10946202.
Swanson ME, Naidoo KS. Corneal complications following refractive surgery: a review. Cont Lens Anterior Eye. 2016;39(4):268-278.
Sahay P, Bafna RK, Reddy JC, Vajpayee RB, Sharma N. Complications of laser-assisted in situ keratomileusis. Indian J Ophthalmol. 2021 Jul;69(7):1658-1669. doi:10.4103/ijo.IJO_1872_20. PMID:34146007; PMCID:PMC8374806.
Venkataraman P, Shroff A, Prabu S, Senthilkumar N. Behind the blur: Understanding interface fluid syndrome in post-LASIK patients. Indian journal of ophthalmology. 2025;73(9):1396. doi:10.4103/IJO.IJO_399_25. PMID:40880161; PMCID:PMC12448521.
Slade SG.. The use of the femtosecond laser in the customization of corneal flaps in laser in situ keratomileusis. Curr Opin Ophthalmol. 2007;18(4):314-317. doi:10.1097/icu.0b013e3281bd88a0. PMID:17568208.
Randleman JB, Woodward M, Lynn MJ, Stulting RD. Risk assessment for ectasia after corneal refractive surgery. Ophthalmology. 2008 Jan;115(1):37-50.e4. doi:10.1016/j.ophtha.2007.03.073. PMID:17624434.
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.