Intracorneal ring segments (ICRS) are synthetic arcuate implants placed at approximately two-thirds depth of the corneal stroma (outside the central optical zone). Introduced in 1987 for myopia correction, they are now positioned as a therapeutic intervention for corneal ectatic diseases such as keratoconus and post-LASIK ectasia.
ICRS function as spacers between corneal lamellae. They shorten the arc length of the central cornea in proportion to the device thickness (arc shortening effect). As a result, the central anterior cornea flattens, and the peripheral area adjacent to the ring insertion is pushed forward.
According to Barraquer’s law, adding tissue to the corneal periphery flattens the central cornea. ICRS is a treatment based on this principle. The thicker the device and the smaller its diameter, the greater the refractive correction achieved.
ICRS is not a curative treatment for keratoconus, but rather a surgical alternative to delay the need for corneal transplantation. Combining ICRS with corneal cross-linking (CXL) can halt disease progression and provide synergistic effects.
QCan ICRS cure keratoconus?
A
ICRS is not a curative treatment for keratoconus. It is a surgical intervention aimed at reducing irregular astigmatism and improving vision, thereby at least delaying the need for corneal transplantation. Combining with CXL can halt disease progression.
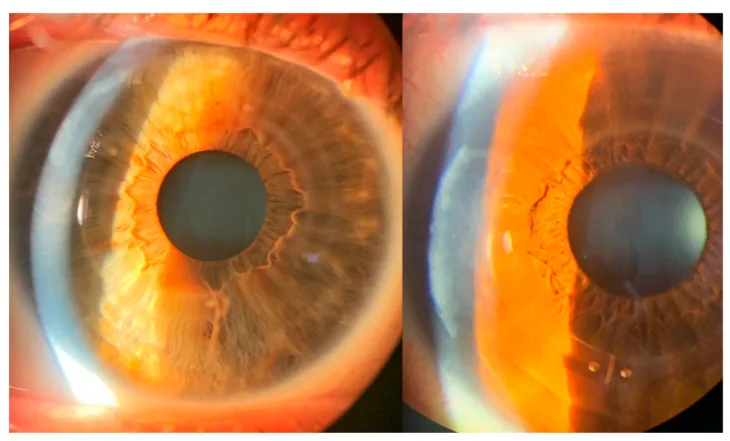
Albertazzi R, Zaldivar R, Rocha-de-Lossada C. ByLimb: Development of a New Technique to Implant Intracorneal Ring-Segments from the Perilimbal Region. Life (Basel). 2023;13(6):1283. Figure 5. PMID: 37374066; PMCID: PMC10302177; DOI: 10.3390/life13061283. License: CC BY.
Postoperative slit-lamp microscopy images showing ICRS placed in the peripheral corneal stroma and incision wound edges in two cases, with no corneal inflammatory findings. These correspond to the postoperative findings of intrastromal corneal ring segments discussed in section “2. Main Symptoms and Clinical Findings.”
Keratoconus is characterized by protrusion and thinning of the central to paracentral cornea. Corneal topography shows a steepening pattern 1). Changes in corneal biomechanics occur before morphological changes 1).
Characteristic findings include Vogt’s striae (fine vertical lines in the deep stroma), Fleischer ring (iron deposition in the epithelium at the base of the cone), and corneal scarring 2). Slit-lamp microscopy reveals forward protrusion and thinning of the cornea, slightly inferior to the center.
Topography after ICRS insertion shows overall corneal flattening, centralization of the corneal apex, maintenance of corneal asphericity, and reduction of surface irregularity.
The etiology of corneal ectasia, for which ICRS is indicated, is multifactorial.
Collagen degradation in the cornea is the essence of thinning 1). Increased matrix metalloproteinases (MMPs) and decreased TIMP are observed 1). Increased IL-6, TNF-α, and MMP-9 in tears induce keratocyte apoptosis1).
Eye rubbing is a major risk factor for keratoconus1). It is associated with atopic diseases (hay fever, asthma, eczema, vernal keratoconjunctivitis) 1).
Keratoconus is usually bilateral but often asymmetric in severity. It typically onsets in adolescence and tends to stabilize or progress slowly around age 30 2). Without treatment, about 20% of cases require corneal transplantation 2).
Post-LASIK ectasia can occur when laser refractive surgery is performed on a cornea with unrecognized subclinical keratoconus1). Thinning of the residual stromal bed and weakening of corneal structure are involved.
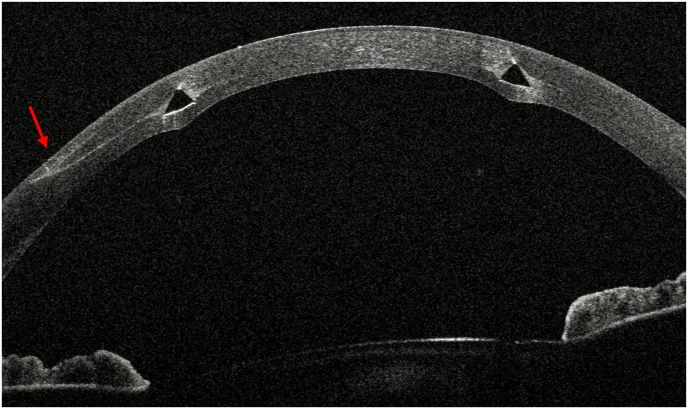
Luft N, Kassumeh S, Dirisamer M, et al. Femtosecond laser-assisted intracorneal MyoRing explantation - A novel rescue technique. Am J Ophthalmol Case Rep. 2025;38:102313. Figure 2. PMID: 40212378; PMCID: PMC11984991; DOI: 10.1016/j.ajoc.2025.102313. License: CC BY.
Preoperative horizontal AS-OCTB-scan shows a hyperreflective area (red arrow) indicating subepithelial stromal fibrosis at the temporal pocket entrance and the cross-sectional structure of the ICRS tunnel. This corresponds to the evaluation of ICRS position and depth by anterior segment OCT discussed in section “4. Diagnosis and Examination Methods”.
For the diagnosis of corneal ectasia, combined use of corneal tomography (Scheimpflug imaging or OCT) and corneal biomechanical assessment is recommended 3).
Key indices required for preoperative evaluation are shown below.
Index
Characteristics
TBI (Tomographic Biomechanical Index)
Integrated index of morphology and biomechanics. High diagnostic performance 3)
CBI (Corvis Biomechanical Index)
Index of corneal deformation response to air puff 3)
SimK1/Ks
Corneal curvature of the steep meridian
SAI / SRI
Symmetry and regularity of corneal shape
CRF (Corneal Resistance Factor)
Reflects overall corneal stiffness 3)
Since a single index may yield false negatives, comprehensive screening combining corneal tomography and biomechanical assessment is recommended 3). In keratoconus, biomechanical changes precede morphological changes, making this useful for early detection 1).
Anterior segment OCT (e.g., CASIA) can acquire tomographic images and corneal topography with high resolution (approximately 10 μm) and has excellent accuracy in detecting opacities. It is also useful for evaluating the depth and position after ICRS implantation.
In children and young adults with keratoconus, the progression may be rapid 4). The KERALINK study evaluated the efficacy of cross-linking in slowing progression in young patients 4).
QWhat tests are needed before ICRS surgery?
A
Preoperatively, corneal tomography (e.g., Pentacam) should be performed to obtain anterior and posterior curvature, corneal thickness map, and elevation map. Comprehensive evaluation combined with corneal biomechanical assessment (TBI, CBI, CRF) is recommended. It is important to measure corneal thickness at the ring insertion site using anterior segment OCT and confirm that it is 450 μm or more.
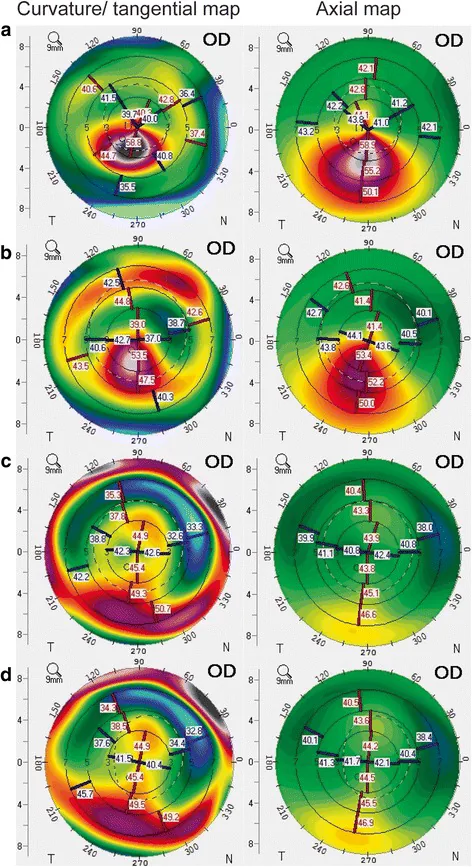
Lee H, Kang DSY, Ha BJ, et al. Visual rehabilitation in moderate keratoconus: combined corneal wavefront-guided transepithelial photorefractive keratectomy and high-fluence accelerated corneal collagen cross-linking after intracorneal ring segment implantation. BMC Ophthalmol. 2017;17(1):270. Figure 2. PMID: 29284455; PMCID: PMC5746954; DOI: 10.1186/s12886-017-0666-1. License: CC BY.
Corneal topography in a patient with moderate keratoconus before surgery (a), after ICRS insertion (b), and at 3 months (c) and 6 months (d) after tPRK + CXL, showing progressive flattening of the cone achieved by ICRS insertion. This corresponds to the improvement in corneal shape (arc shortening effect) after ICRS insertion discussed in the section “5. Standard Treatment.”
Channel creation methods include mechanical dissection and femtosecond laser1). The implantation depth of 70–80% of corneal thickness is the general standard for synthetic ICRS. With femtosecond laser, channels are created at precise depth and diameter based on pachymetry maps 1).
CAIRS can be inserted at shallower depths (35–70%) and is expected to provide a greater flattening effect 5).
The mean change in corneal curvature after ICRS insertion ranges from 2.14 to 9.60 D. Reductions in spherical power, astigmatic power, and spherical equivalent have been reported. It is considered most effective for moderate keratoconus (Kmax < 58.0 D)1). However, changes in astigmatism can sometimes be unpredictable1).
A meta-analysis (12-month follow-up, 6 studies) of simultaneous ICRS and CXL showed that simultaneous surgery yielded better results in spherical refractive error and steep-K than either CXL-first or ICRS-first approaches 1).
ICRS alone may not stop the progression of keratoconus. Simultaneous performance with CXL showed superior results in spherical refractive error and steep-K compared to CXL-first or ICRS-first approaches 1). Chan et al. reported that Intacs + CXL combination was more effective than Intacs alone for improving keratoconus6). In a three-step treatment of ICRS + CXL + tPRK (topography-guided PRK) by Hashemian et al., sustained improvement in Kmax values was confirmed at 6-month follow-up 8).
Faria-Correia et al. (2023) reported outcomes of ICRS implantation via a limbal incision approach 9). The limbal approach avoids the optical zone of the cornea and reduces the risk of postoperative corneal scarring. The AAO Corneal Ectasia PPP (2024) states that both mechanical dissection and femtosecond laser methods show equivalent outcomes, with the femtosecond laser providing more precise channel depth control 1).
The prevalence of keratoconus is reported as 50–230 per 100,000 in the general population (138 per 100,000 in a recent large meta-analysis) 15). Without treatment intervention, approximately 20% require corneal transplantation, making early intervention with CXL and ICRS important 2). A meta-analysis by Pédretti et al. (2022) confirmed significant improvements in mean UDVA and CDVA after ICRS insertion 11). A 5-year long-term follow-up by Vega-Estrada et al. showed that refractive and visual improvements after ICRS insertion were maintained for 5 years, confirming long-term efficacy and predictability 12). A 1998 review by Rabinowitz reported a prevalence of 0.05% 15), but the latest AAO Corneal Ectasia PPP (2024) suggests this value may be significantly higher 1).
CAIRS Salvage Surgery After Synthetic ICRS Failure by Nuzzi et al.
Nuzzi et al. (2025) reported a technique for replacing synthetic ICRS with CAIRS after long-term complications 7). In a case with subepithelial stromal fibrosis at the temporal pocket entrance assessed by anterior segment OCT, the synthetic ICRS was explanted and CAIRS was inserted 3 months later. Postoperative Kmax improved from 68.9 to 61.9 D, and UCVA improved from 20/400 to 20/30. CAIRS can be an effective salvage option even in cases where synthetic ICRS has failed.
In the treatment of corneal ectasia, ICRS is indicated for cases with contact lens intolerance and progressive visual impairment but with a clear central cornea. It is positioned as a precursor to full-thickness penetrating keratoplasty (PKP) and deep anterior lamellar keratoplasty (DALK). The AAO PPP notes that DALK has the advantages of no risk of endothelial rejection and a lower risk of globe rupture compared to PKP1). The recent decline in the number of corneal transplant surgeries is thought to reflect the widespread adoption of early intervention with CXL and ICRS. The Refractive Surgery Guidelines (8th edition) clearly state that keratoconus is a contraindication for excimer laser surgery and SMILE surgery10), emphasizing the importance of appropriate preoperative screening.
Key points of postoperative guidance for patients who have undergone ICRS implantation:
Do not rub your eyes: Eye rubbing is a major risk factor for keratoconus progression and is also involved in ICRS extrusion1). If allergic conjunctivitis is present, manage itching with antiallergic medications.
Reconsider contact lens use: Refitting with scleral lenses or hybrid lenses may be necessary after ICRS.
Inform about symptoms of ICRS extrusion: Sudden vision loss, irritation, or redness may be early signs of extrusion. Instruct patients to seek immediate medical attention.
Relationship with CXL: Maintain close follow-up after ICRS until stabilization with CXL alone is confirmed.
Diagnostic Criteria and Severity Classification of Keratoconus
QWhat are the advantages of combining ICRS and CXL?
A
ICRS improves corneal shape and visual acuity, but alone may not halt progression. CXL increases corneal rigidity through collagen cross-linking, providing a progression-stopping effect. Simultaneous performance has been reported to show the best results, yielding synergistic effects of shape improvement and progression arrest.
ICRS extrusion is a complication in which the ring protrudes from the corneal surface due to progressive corneal stromal thinning and epithelial breakdown. It accounts for 48.2% of all removal cases, with an average onset time of about 10 years, but it can occur at any time from 1 month to 20 years postoperatively.
Early postoperative risk stratification using CAS-OCT is useful. Cases with an average depth percentage of less than 60% or tunnel depth of less than 70% at the first week and first month after implantation are considered high risk.
Risk Factors
Details
Ring migration
ICRS width too wide for thin cornea, tunnel too shallow or narrow
Corneal melting
Ring placement near incision, inflammation due to infection, trauma, or stromal dissection
Removal is the definitive treatment for ICRS extrusion. Indications include extrusion, decreased or fluctuating visual quality, corneal melting, infectious keratitis, contact lens intolerance, and corneal perforation.
There are two incision methods depending on the situation. If the extrusion is near the incision site, open the previous entry with a sinskey hook. If the incision site has healed, create an incision window under the extruded ring with a diamond knife set to the original depth. In either case, close the defect with 10-0 nylon sutures.
When Complicated by Infectious Keratitis
Culture testing: Perform culture of conjunctival and corneal scrapings in all cases.
Treatment: High-concentration antibiotic eye drops combined with explantation. Antibiotics alone without explantation may also be effective in some cases.
Severe cases: Progression to endophthalmitis requires systemic antibiotics. Early full-thickness corneal transplantation may be an alternative.
Postoperative Management
Eye drops: Use antibiotic-steroid combination eye drops for 5 days.
Artificial tears: Use for 1–3 months, and instruct the patient to avoid eye rubbing.
After ring explantation, no worsening of corrected visual acuity, astigmatism, or myopia was observed. Traces of lamellar opacity decrease over time.
QHow can ICRS extrusion be prevented?
A
There are three main preventive measures: Adhere to the “pachymetry rule” and keep ring thickness less than half the corneal thickness at the implantation site. Use femtosecond laser to accurately create a tunnel with 80% channel depth. Place the ring tip away from the incision. Postoperatively, confirm early ring position stability with CAS-OCT.
The elastic modulus of the cornea is a quantitative measure of its tendency to deform elastically under force. In keratoconus, the elastic modulus is reduced due to pathological changes in the stroma.
The decrease in elastic modulus results from degradation and degeneration of collagen fibers 3). This initiates a biomechanical failure cycle. Stress levels increase and redistribute, leading to corneal steepening and thinning 3). In the thinned area, local stress further increases, forming a vicious cycle that worsens the protrusion.
ICRS intervenes in this vicious cycle through the following mechanisms.
Addition of peripheral tissue (Barraquer’s law): Inserting a spacer into the corneal stroma shortens the central arc length (arc shortening) and flattens the cornea.
Stress redistribution: ICRS absorbs and distributes stress, reducing concentration on the steepened cone area.
Stromal stabilization: The mechanical support of ICRS physically suppresses forward protrusion of the cone.
Andreassen et al. reported that the elastic modulus of keratoconic stroma is reduced to approximately 60% of that of normal cornea13). This reduction in elasticity is the primary biomechanical background of corneal ectasia, and ICRS functions as structural reinforcement.
The effect of ICRS is closely related to the structural properties of the collagen framework of the corneal stroma. The stroma accounts for 90% of corneal thickness, and its mechanical properties determine the overall biomechanics of the cornea.
The pathology of ICRS extrusion is broadly divided into two mechanisms: ring migration and corneal melting.
Ring migration results from shallow implantation. Placing ICRS too shallowly increases anterior tensile strain, leading to stromal compression. Progression of anterior stromal compression causes epithelial and stromal breakdown, leading to corneal thinning and eventual spontaneous extrusion.
Corneal melting reflects an underlying inflammatory process. Surgical trauma during incision and tunnel creation induces progressive keratocyte apoptosis and tissue degeneration. Involvement of MMPs has been suggested, and introduction of exogenous stimuli leads to degradation and thinning of the corneal matrix.
CAIRS (Corneal Allogenic Intrastromal Ring Segments) involves inserting stromal segments derived from donor corneal tissue into the stroma. They reduce the curvature of the cone area through an arch-shortening effect similar to synthetic ICRS.
While synthetic ICRS requires insertion into the deep stroma (70–80% depth), CAIRS can be inserted at shallower depths (35–70%), potentially producing a greater flattening effect 5).
Allogenic segments are implanted into the avascular, low-cell-density corneal stromal layer. This environment minimizes fibrous adhesion and preserves surgical reversibility. The risks of corneal melting, acute stromal necrosis, and corneal neovascularization associated with synthetic ICRS are also reduced 5).
Advances in corneal biomechanics evaluation are attracting attention. New indices such as TBI and CBI complement traditional morphological indices and improve the detection accuracy of early keratoconus3). Integrated evaluation of biomechanical indices and corneal tomography has been reported to improve the prediction accuracy of refractive surgery by more than 25% 3).
A meta-analysis on the combination of CXL and ICRS, including 6 studies with 12-month follow-up, showed that simultaneous surgery was superior to CXL-first in spherical refractive error and flat-K, and superior to both CXL-first and ICRS-first in steep-K. 1)
According to a systematic review (AlQahtani et al., 2025), after CAIRS implantation, mean UDVA improved from 0.83 to 0.40 logMAR, CDVA from 0.52 to 0.19 logMAR. Spherical equivalent decreased from −7.09 D to −2.34 D, Kmax from 57.8 to 53.6 D, and Kmean from 49.3 to 45.3 D 5). Regarding long-term effects of CXL, the Siena Eye Cross Study by Caporossi et al. (mean follow-up 6 years) reported that riboflavin-UV-A corneal crosslinking halted or improved progression in 74% of keratoconus cases 14).
Similar improvements have been reported for CTAK. Mean UDVA improved from 1.21 to 0.61 logMAR, and CDVA from 0.63 to 0.34 logMAR 5).
Complications of CAIRS are few and minor. Transient dry eye and intrastromal deposits are most common but not clinically significant. Glare and halos were significantly less frequent compared to synthetic ICRS5).
The complication rate of synthetic ICRS has been reported to be up to 30% 5). Multiple successful cases of CAIRS rescue for complications such as ICRS exposure, anterior chamber migration, and corneal melting have been reported 5). In a 49-year-old female with failed ICRS (UCVA 20/400), the synthetic ICRS was removed and CAIRS was inserted 3 months later, improving Kmax from 68.9 to 61.9 D and UCVA to 20/30 5).
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Meyer JJ, Gokul A, Vellara HR, McGhee CNJ. Progression of keratoconus in children and adolescents. The British journal of ophthalmology. 2023;107(2):176-180. doi:10.1136/bjophthalmol-2020-316481. PMID:34479856.
Wang Y, Xie L, Yao K, Sekundo W, Alió JL, Mehta JS, Goel S, Elmassry A, Schallhorn J, Shilova T, Cao H, Xu L, Chen X, Zhang F, Bai J, Zhang W, Liu Q, Zhou X, Chen Y, Wang Z, Jhanji V, Yang K, Writing Committee for the Guideline Working Group. Evidence-Based Guidelines for Keratorefractive Lenticule Extraction Surgery. Ophthalmology. 2025;132(4):397-419. doi:10.1016/j.ophtha.2024.11.016. PMID:39577672.
Larkin DFP, Chowdhury K, Burr JM, et al. Effect of corneal cross-linking versus standard care on keratoconus progression in young patients: The KERALINK randomized controlled trial. Ophthalmology. 2021;128:1516-1526. doi:10.1016/j.ophtha.2021.04.019. PMID:33892046.
Bader S. AlQahtani, Roaya Ayed Alsulami. The role of corneal allogenic intrastromal ring segments (CAIRS) implantation after failed synthetic intracorneal ring segments (ICRS): A rescuer. American Journal of Ophthalmology Case Reports. 2025;38:102287. doi:10.1016/j.ajoc.2025.102287.
Chan E, Snibson GR. Current status of corneal collagen cross-linking for keratoconus: a review. Open Ophthalmol J. 2018;12:181-213.
Nuzzi R, Tridico F, Carrai P, Dalmasso P. Corneal allogenic intrastromal ring segment implantation in failed synthetic intracorneal ring segments. Am J Ophthalmol Case Rep. 2025;38:102313.
Hashemian MN, Naderan M, Mohammadpour M, et al. Corneal collagen cross-linking combined with intracorneal ring segment implantation for keratoconus treatment. BMC Ophthalmol. 2017;17:270.
Faria-Correia F, Monteiro T, Franqueira N, Ambrósio R Jr. Limbal corneal incision for intrastromal corneal ring segment implantation. Life (Basel). 2023;13:1283.
Pedrotti E, Chierego C, Fasolo A, et al. Intrastromal corneal ring segments for keratoconus: systematic review and meta-analysis. Eye Vis (Lond). 2022;9:34.
Vega-Estrada A, Alio JL, Brenner LF, Burguera N. Outcomes of intrastromal corneal ring segments for treatment of keratoconus: Five-year follow-up analysis. J Cataract Refract Surg. 2013;39(8):1234-1240. doi:10.1016/j.jcrs.2013.03.019.
Andreassen TT, Simonsen AH, Oxlund H. Biomechanical properties of keratoconus and normal corneas. Experimental eye research. 1980;31(4):435-41. doi:10.1016/s0014-4835(80)80027-3. PMID:7449878.
Caporossi A, Mazzotta C, Baiocchi S, Caporossi T. Long-term results of riboflavin ultraviolet a corneal collagen cross-linking for keratoconus in Italy: the Siena eye cross study. American journal of ophthalmology. 2010;149(4):585-93. doi:10.1016/j.ajo.2009.10.021. PMID:20138607.