PG accounts for 1–1.5% of all glaucoma cases 2). It is more common in myopic Caucasian men, with typical diagnosis between ages 30 and 50 2)3). The risk of progression from PDS to PG is reported as 10–50% in clinic-based studies, but this may reflect a population biased toward PDS patients with elevated intraocular pressure2)3). Population-based studies report a conversion rate of about 10% at 5 years and 15% at 15 years.
QHow are PDS and PG different?
A
PDS is a condition characterized by dispersion of iris pigment and deposition of pigment in the anterior segment; it can be diagnosed whether intraocular pressure is normal or elevated. PG is PDS accompanied by glaucomatous optic disc cupping or visual field defects 2). In other words, PDS is a precursor to glaucoma, and not all PDS patients progress to PG.
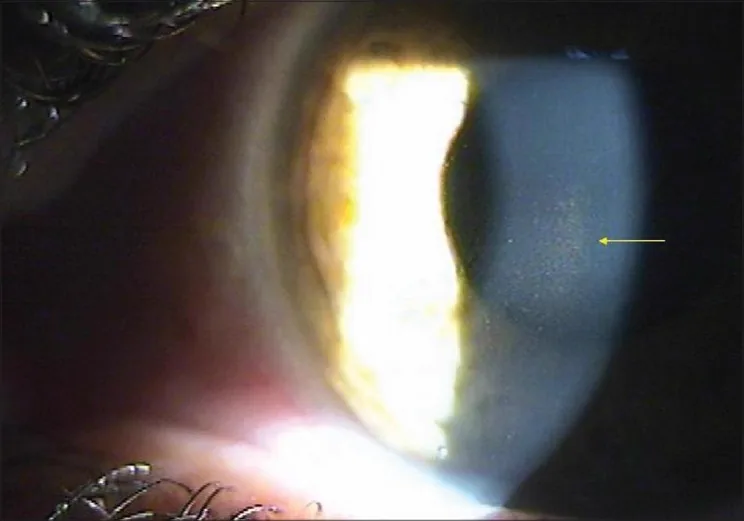
Bhallil S, et al. Pigment dispersion syndrome: An atypical presentation. Oman J Ophthalmol. 2010. Figure 1. PMCID: PMC2886225. License: CC BY.
Slit-lamp photograph showing fine pigment deposits gathered in a vertical spindle shape on the corneal endothelium. This is a representative finding of Krukenberg spindle and is suitable for explaining the clinical findings of pigment dispersion syndrome and pigmentary glaucoma.
PDS is often asymptomatic. Transient blurred vision due to intraocular pressure spikes after exercise or during mydriasis is a characteristic symptom2)3). Halos may also be seen. Visual field defects are noticed only when PG has progressed. In cases where patients notice blurred vision with exercise, checking the angle and intraocular pressure immediately after exercise can provide diagnostic clues.
Krukenberg spindle: Spindle-shaped pigment deposited vertically in the central corneal endothelium. It is oriented vertically due to convection. It is found in about 90% of PDS/PG patients but is not pathognomonic2)3).
Transillumination defects of the mid-peripheral iris: Present a spoke-like (radial) pattern. They correspond to the areas of maximum contact between the iris pigment epithelium and the lens zonules2)3).
Heavy pigmentation of the trabecular meshwork: On gonioscopy, the trabecular meshwork appears uniformly dark brown2)3).
Other findings
Scheie line (Zentmayer ring): Pigment deposition along the attachment of the zonules on the posterior lens capsule2)3).
Deep anterior chamber: Accompanied by posterior bowing of the peripheral iris (reverse pupillary block)2)3).
Pigment reversal sign: In elderly “burned-out” PG, pigmentation of the superior trabecular meshwork is stronger than that of the inferior.
Anisocoria and iris heterochromia: In cases with asymmetry, the pupil on the side of pigment loss may become larger.
Melanin pigment is released from the iris pigment epithelium 2)3). The cause is friction between the lens zonules and the posterior iris surface. Posterior bowing of the iris, called “reverse pupillary block,” is observed in many PDS/PG eyes 2)3).
With blinking, aqueous humor is pushed from the posterior chamber into the anterior chamber, creating a pressure gradient where anterior chamber pressure exceeds posterior chamber pressure. This results in posterior concavity of the iris and increased contact area with the lens. Mydriasis, accommodation, and vigorous exercise also promote pigment release.
Age of onset is in the 30s for men and about 10 years later for women. Flat cornea, concave iris, and posterior iris insertion are also associated factors. Autosomal dominant inheritance with incomplete penetrance has been suggested, and the GPDS1 locus (7q35-q36) has been identified by linkage analysis.
QWhat is reverse pupillary block?
A
In normal pupillary block, posterior chamber pressure exceeds anterior chamber pressure, causing the iris to bulge forward. Reverse pupillary block is the opposite: due to blinking or other factors, anterior chamber pressure exceeds posterior chamber pressure, causing the iris to become concave posteriorly 2)3). This posterior bowing of the iris increases contact between the iris pigment epithelium and the lens zonules, leading to pigment release from the iris pigment epithelium. Laser iridotomy may eliminate the pressure difference between the anterior and posterior chambers 1).
The diagnosis of PDS is based on the following three findings 2)3).
Transillumination defects in the mid-peripheral iris (radial pattern)
Pigment deposition on the corneal endothelium (Krukenberg spindle)
Dense, uniform pigmentation of the trabecular meshwork
If all three findings are present without other causes such as trauma, posterior chamber IOL, or uveitis, PDS is strongly suspected. Diagnosis of PG requires the criteria for PDS plus optic disc cupping and visual field defects.
Uveitis, trauma, sulcus IOL placement, and iris melanoma can also cause heavy trabecular pigmentation 4). Gonioscopy should be performed before pupil dilation to assess the distribution pattern of trabecular pigmentation 1).
UBM or AS-OCT can evaluate iris concavity, but it is not essential for diagnosis.
Eye drops used for primary open-angle glaucoma (prostaglandin analogs, beta-blockers, carbonic anhydrase inhibitors, alpha-2 agonists) are used 1). Pilocarpine reduces iris concavity and suppresses exercise-induced intraocular pressure elevation, but caution is needed for myopia, accommodative spasm, and risk of retinal detachment (lattice degeneration present in up to 20%).
Laser trabeculoplasty: Has efficacy comparable to medication, but due to heavy trabecular pigmentation, postoperative IOP spikes are more likely 2)3). It should be performed with lower energy than usual, and pretreatment to prevent IOP spikes should be given 1)2)3).
Laser iridotomy: Considered to relieve reverse pupillary block and reduce contact between the iris and zonules 1). However, its efficacy is debated 3). It may be beneficial in young patients with active pigment release.
Surgical Treatment
Lens extraction: Relieves reverse pupillary block and reduces pigment dispersion 1). It is considered useful for preventing irreversible trabecular damage.
Aqueous outflow pathway reconstruction: Trabeculotomy, etc., can be effective 1).
Filtration surgery: Indicated when medical and laser treatments are insufficient1)
QWhat are the precautions for laser trabeculoplasty in pigmentary glaucoma?
A
In pigmentary glaucoma, due to heavy pigmentation of the trabecular meshwork, laser energy absorption is high, and postoperative intraocular pressure spikes are likely to occur2)3). The procedure should be performed at lower energy than usual, and pretreatment to prevent intraocular pressure spikes (such as prophylactic administration of alpha-2 agonists or beta-blockers) should be performed1). Note that the intraocular pressure-lowering effect may diminish after several years2).
Release of melanin pigment from the iris pigment epithelium occurs due to mechanical friction between the lens zonules and the posterior iris surface2)3). The “reverse pupillary block” configuration causes the iris to bow posteriorly, increasing contact between the iris and zonules2)3).
The expulsion of aqueous humor into the anterior chamber with blinking (burp phenomenon) creates a pressure gradient between the anterior and posterior chambers, maintaining the concave configuration of the iris. Mydriasis, accommodation, and vigorous exercise also promote pigment release. The concentration of pigment granules in the aqueous humor of PDS/PG eyes reaches 15 times that of normal controls.
Melanin granules deposit in the aqueous outflow pathway and increase outflow resistance2)3). Trabecular meshwork cells phagocytose the pigment and subsequently undergo cell death2)3). This is the central understanding of the current pathogenesis of PG. Histopathologically, collapse of trabecular beams, free pigment granules, pigment-laden macrophages, and degenerated trabecular endothelial cells are observed.
With aging, the lens moves forward, reducing contact between the iris and zonules, so pigment release diminishes in older individuals. However, irreversible damage to the trabecular meshwork persists, so PG may become manifest in older patients.
In recent years, cases of bilateral severe pigmentary glaucoma after photoablative iridoplasty for cosmetic purposes have been reported5). A 32-year-old woman developed intraocular pressures of 50/42 mmHg after laser treatment to change iris color, requiring emergency bilateral trabeculectomy5). Paracentral acute middle maculopathy (PAMM) also occurred, resulting in irreversible visual impairment5).
Cases of PDS developing after placement of large-diameter (7 mm) intraocular lenses in the ciliary sulcus have also been reported 6). The cause is friction between the iris and the edge of the IOL optic, and improvement was achieved by switching to scleral-fixated IOL implantation 6).
Cases have been reported in which herpes simplex virus-1 anterior uveitis progressed to acute iris transillumination defect-like syndrome, leading to pigmentary glaucoma7). It has been suggested that steroid monotherapy without antiviral drugs may have exacerbated viral replication and promoted destruction of the iris pigment epithelium 7).
Linkage analysis has identified the GPDS1 locus (7q35-q36) as a genetic locus associated with PDS, but the causative gene has not yet been identified. The development of biomarkers to predict conversion from PDS to PG is also a future challenge.
QWhat types of iatrogenic pigmentary glaucoma exist?
A
Two main mechanisms have been reported. One is cosmetic iris color change laser (photoablative iridoplasty), which has caused severe pigmentary glaucoma and retinal damage (PAMM) due to massive pigment release 5). The other is the development of PDS due to friction between the iris and a large-diameter IOL placed in the ciliary sulcus after posterior capsule rupture during cataract surgery, which can be improved by changing the IOL fixation position 6). Although both have different etiologies from primary PDS/PG, they share the common mechanism of intraocular pressure elevation due to pigment dispersion.
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Liu J, Korban S, Moster MR, Rhéaume MA, Wang Q. Bilateral severe iatrogenic pigmentary glaucoma following laser treatment for cosmetic iris color change. American journal of ophthalmology case reports. 2023;32:101927. doi:10.1016/j.ajoc.2023.101927. PMID:37771388; PMCID:PMC10522941.
Nagata M, Matsushima H, Senoo T. A Case of Pigment Dispersion Syndrome after Placement of Sulcus Intraocular Lens with 7-mm Optic Diameter after Posterior Capsule Rupture. Case reports in ophthalmology. 2022;13(3):1003-1009. doi:10.1159/000527750. PMID:36605041; PMCID:PMC9808161.
Radmilovic M, Maric G, Vukojevic A, et al. An unusual manifestation of herpes simplex virus-1 uveitis transforming into an acute iris transillumination-like syndrome with pigmentary glaucoma. Life. 2025;15:1164.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.