The Ahmed ClearPath (New World Medical, Rancho Cucamonga, CA) is a non-valved glaucoma drainage device (GDD) used in the surgical management of glaucoma. It received FDA approval in the United States in 2019 and was introduced to the market.
Glaucoma drainage devices lower intraocular pressure by draining aqueous humor from the eye through a tube to a plate, where it is absorbed by surrounding tissues through a capsule formed around the plate 2). They are broadly classified into two types based on the presence or absence of a valve 2).
Non-valved (without valve): Baerveldt glaucoma implant, Ahmed ClearPath, Molteno implant
Valved (with valve): Ahmed glaucoma valve (FP7, FP8)
A survey by the American Glaucoma Society (AGS) reported that 17% of respondents prefer Ahmed ClearPath as a non-valved shunt.
Accessories: Includes a 23-gauge needle (for scleral incision)
The 250 mm² model can be placed between the rectus muscles without separating them.
QWhat is the difference between valved and non-valved glaucoma drainage devices?
A
Valved devices (e.g., Ahmed glaucoma valve) allow aqueous outflow immediately after surgery through a pressure-regulating mechanism, preventing excessive hypotony. Non-valved devices (e.g., ClearPath, Baerveldt) lack a pressure-regulating valve, so tube ligation is required to prevent early postoperative overfiltration. Non-valved devices generally provide better long-term intraocular pressure control than valved devices, but carry a slightly higher risk of postoperative hypotony4).
Glaucoma drainage devices have traditionally been used in cases where trabeculectomy has failed or is unlikely to succeed2). Specific indications include:
In recent years, the indications for glaucoma drainage devices have been expanding. Medicare data from 1994 to 2012 show an increase in shunt surgeries, while trabeculectomy numbers decreased during the same period2).
In Japan, two types of glaucoma drainage devices are covered by health insurance: the Baerveldt glaucoma implant and the Ahmed glaucoma valve. Good indications include eyes that have undergone previous trabeculectomy with poor outcomes, or glaucomatous eyes with a history of intraocular surgery.
For cases aiming for lower intraocular pressure, the Baerveldt glaucoma implant (non-valved type) is often selected. For cases where postoperative hypotony is risky (e.g., aphakic eyes, eyes with sutured IOL, history of expulsive hemorrhage, uveitic glaucoma), the Ahmed glaucoma valve (valved type) tends to be chosen.
5. Surgical Technique and Postoperative Management
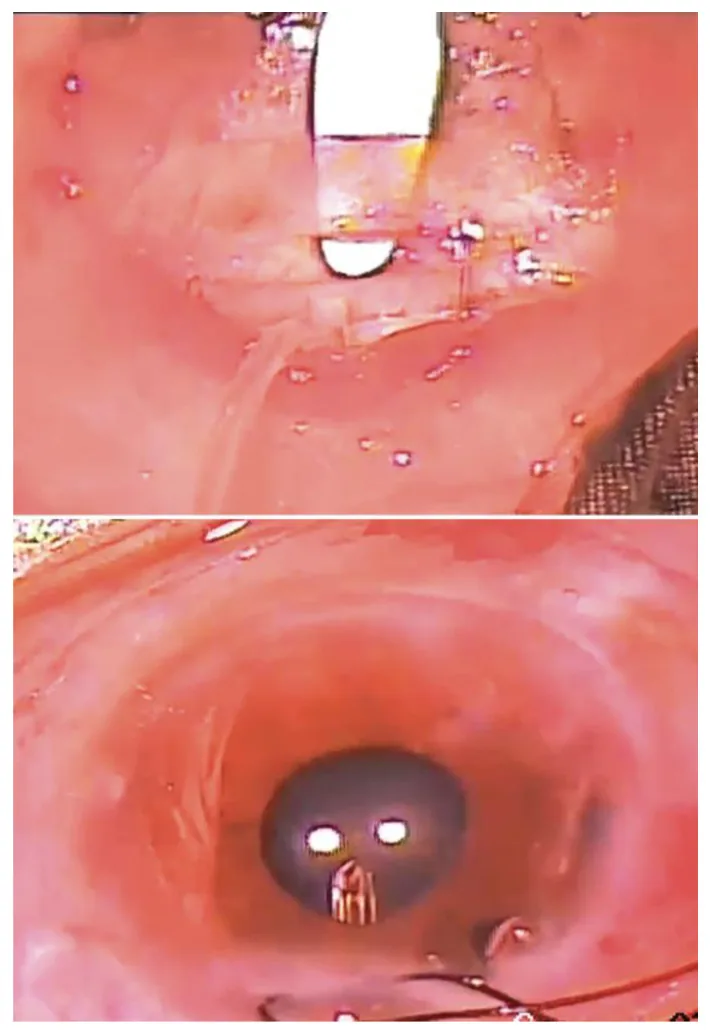
The upper panel shows creation of a lamellar scleral tunnel, and the lower panel shows the tube being passed into the posterior chamber. This illustrates the intraoperative procedure of guiding the tube into the eye after fixing the device plate.
The basic surgical technique for glaucoma drainage device surgery shares many common steps between valved and non-valved types.
Conjunctival incision: Performed at the limbal base or fornix base
Plate placement: Placed between two rectus muscles (often in the superotemporal quadrant). The plate is fixed posteriorly from the muscle insertion.
Tube insertion: A needle track is created with a 23-gauge needle 1.5–2 mm posterior to the corneal limbus, and the tube is inserted into the anterior chamber. The tube is trimmed bevel-up so that the tip protrudes about 2 mm into the anterior chamber.
Patch graft: The tube is covered with preserved sclera, cornea, or pericardium to prevent postoperative tube exposure 2)
For non-valved devices (ClearPath, Baerveldt), the following additional steps are required:
Tube ligation (ligature): The tube is ligated with 8-0 Vicryl suture, occluding the tube until it dissolves at 4–6 weeks postoperatively. This prevents hypotony due to excessive filtration 1)
Sherwood slit: A slit is made in the tube with a nylon needle to temporarily relieve intraocular pressure during ligation.
Ripcord: A non-absorbable suture is placed in the tube lumen. It is removed postoperatively under a slit lamp to adjust outflow1)
For the Ahmed glaucoma valve (valved type), priming of the pressure-regulating valve (verification of valve function by infusion of irrigation fluid) is necessary, but tube ligation or Sherwood slit is not required.
Non-valved type
ClearPath / Baerveldt
Intraocular pressure control: Depends solely on the resistance of the capsule. Achieves lower intraocular pressure in the long term4)
Early postoperative period: Ligature and ripcord prevent excessive filtration1)
Hypotony risk: Slightly higher than valved type (4.5% vs 0.4%)4)
Valved type
Ahmed glaucoma valve
Intraocular pressure control: The pressure-regulating valve theoretically prevents pressure below 8 mmHg. Intraocular pressure decreases immediately after surgery.
Early postoperative period: Priming only. No ligation or Sherwood slit required.
Complications: The frequency of postoperative complications is low, but long-term intraocular pressure control is inferior to the non-valved type4)
In the DBACS study (RCT of ClearPath 350 vs Baerveldt 350), no significant differences were observed between the two groups in surgical time, number of venting slits, number of wicks, surgical quadrant, graft type, or tube position1).
Surgical time: BVT group 43.5±11.2 min vs ACP group 46.9±18.4 min (p=0.802)1)
Most placed in the superotemporal quadrant, with scleral patch graft and tube placement in the anterior chamber
Postoperatively, antibiotic eye drops are used for about 2 weeks, and steroid eye drops are tapered over about 6 months. In non-valved devices, intraocular pressure often remains elevated around 20 mmHg until the ligature dissolves at 4–6 weeks, and follow-up is performed with concomitant use of pressure-lowering eye drops. Intraocular pressure often decreases after 1–2 months.
Tube exposure is more frequent with inferior placement. The risk of corneal endothelial damage increases when the tube is close to the cornea.
QWhat is a ripcord? When is it removed?
A
A ripcord is a thick non-absorbable suture (4-0 polypropylene) placed inside the tube lumen. It partially occludes the tube, limiting aqueous outflow. After the ligature naturally dissolves, the ripcord is removed under a slit lamp in the outpatient clinic, allowing a gradual increase in outflow and more precise intraocular pressure control 1).
Glaucoma drainage devices consist of a silicone tube and a plate. Aqueous humor from the anterior chamber is drained through the tube to the plate, where it is absorbed by surrounding tissues via a fibrous capsule that forms around the plate within weeks after surgery 2)3). Intraocular pressure reduction mainly depends on the outflow resistance of this capsule.
In non-valved devices, outflow resistance depends solely on the capsule, so tube occlusion with a ligature is essential in the early postoperative period until the capsule is sufficiently formed 1). In valved devices, a pressure-regulating valve provides additional outflow resistance, allowing immediate aqueous drainage while preventing hypotony.
ClearPath is a non-valved device similar to Baerveldt, but has the following unique design features:
Low-profile plate: Thin and flexible, suitable for cases with narrow orbits or pediatric glaucoma with buphthalmos
Winged design: The 350 mm² model allows posterior placement avoiding rectus muscle insertions
Anterior suture eyelets: Facilitate implant fixation without requiring deep posterior dissection
Pre-loaded ripcord: Eliminates the need for intraoperative ripcord preparation
In a laboratory study by Langenberg et al., the fluid resistance and suture eyelet integrity of ClearPath 350 and Baerveldt 350 were reported to be equivalent.
Theoretically, a larger plate area increases the bleb surface area and reduces outflow resistance. Multiple retrospective studies have shown that larger plate area is associated with lower intraocular pressure and fewer glaucoma medications 2). However, a prospective study comparing 350 mm² and 500 mm² Baerveldt implants reported that the 350 mm² group had a higher success rate at 5 years, suggesting that larger size is not always advantageous 2).
7. Clinical Outcomes and Recent Research (Investigational Reports)
Quist et al. (2025) conducted the first randomized controlled trial (DBACS) comparing ClearPath 350 and Baerveldt 350 at Duke University 1). Seventy-six patients were enrolled (BVT group 37, ACP group 39), 70 underwent surgery, and 61 completed 12-month follow-up. Baseline intraocular pressure was not significantly different between groups (BVT 21.7±7.1 vs ACP 22.4±6.7 mmHg).
The primary results of the DBACS trial are shown below 1).
Parameter
Baerveldt 350
ClearPath 350
p value
12-month IOP
14.1±4.3 mmHg
11.4±3.9 mmHg
0.010
IOP reduction rate
-30.7%
-44.1%
0.038
The ClearPath group achieved significantly lower IOP than the Baerveldt group at 6 weeks (12.1 vs 16.3 mmHg, p=0.032), 3 months (12.8 vs 16.5 mmHg, p=0.026), and 12 months 1). The number of glaucoma medications was similar between groups, and complications were infrequent and not significantly different. Although the study enrolled only 76 patients versus the target of 304, a statistically significant difference was detected for the primary endpoint 1).
Elhusseiny and VanderVeen reported initial outcomes of ClearPath in 7 eyes of pediatric glaucoma. At a median follow-up of 12 months, mean IOP decreased significantly from 36±3.5 mmHg to 12.4±2.8 mmHg (p<0.001). The number of medications also decreased from 2.7±0.6 to 0.7±0.8 (p=0.0009).
In a multicenter retrospective study by Grover et al., ClearPath outcomes were evaluated in 104 adult eyes (63.5% primary open-angle glaucoma [POAG]). At 6 months, mean IOP decreased significantly from 26.3±9 mmHg to 13.7±4.7 mmHg (p<0.0001), and 91.8% of eyes achieved IOP ≤18 mmHg. Main complications included anterior chamber inflammation (16.3%), hyphema (15.4%), and early hypotony (6.7%).
Comparison data with existing glaucoma drainage devices
Regarding long-term outcomes of glaucoma drainage devices in general, the 5-year results of the Tube Versus Trabeculectomy (TVT) study showed a cumulative failure rate of 29.8% in the Baerveldt group and 46.9% in the trabeculectomy group, which was significantly higher (p=0.02) 4).
In a 5-year comparison of the Ahmed glaucoma valve and Baerveldt glaucoma implant (meta-analysis of ABC/AVB studies), the Baerveldt group achieved lower IOP but had a significantly higher rate of hypotony (4.5% vs 0.4%, p=0.002) 4).
QWhich is better, ClearPath or Baerveldt?
A
In the DBACS study, the ClearPath 350 group achieved significantly lower IOP than the Baerveldt 350 group at 12 months 1). However, the study was small and follow-up was only 1 year, so further research is needed to evaluate long-term safety and efficacy. How the structural differences between the two devices affect clinical outcomes is expected to be examined in future large-scale, long-term studies.
Quist MS, Gross AW, Johnson NA, Stinnett SS, Wen JC, Challa P, et al. The Duke Baerveldt 350 Versus Ahmed ClearPath 350 Study (DBACS): A Randomized Control Trial In Adults With Medically Refractory Glaucoma. Clinical ophthalmology (Auckland, N.Z.). 2025;19:3449-3463. doi:10.2147/OPTH.S523294. PMID:40989068; PMCID:PMC12452963.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.